
Abstract
Monkeys with insulin-dependent diabetes are important experimental models for islet xenotransplantation. However, with regard to diabetes induction, total pancreatectomy is a difficult operation with a high complication rate, while streptozotocin (STZ) administration may cause serious toxic effects and individual difference in metabolism. We compared two strategies involving pancreatectomy and STZ to successfully and safely induce diabetes in rhesus monkeys. Thirteen rhesus monkeys were divided into two groups: single high-dose STZ administration (80, 100 and 120 mg/kg, n = 3 for each dose) (group 1) and partial pancreatectomy (70–75%) combined with low-dose STZ (15 mg/kg, n = 4) (group 2). Induction of diabetes was evaluated by blood glucose, insulin, C-peptide, intravenous glucose tolerance test (IVGTT) and arginine stimulation test (AST). Detection of hematological and serum biochemical parameters and biopsies of pancreas, liver and kidney were periodically performed. In our study, animals in both groups developed diabetes. Serum C-peptide levels in groups 1 and 2 decreased to 0.08 ± 0.07 and 0.35 ± 0.06 nmol/L, respectively. IVGTT and AST indicated severely impaired glucose tolerance. Immunohistochemistry demonstrated that rare insulin-positive cells remained in the pancreas. In terms of STZ toxicity, four monkeys died 8–14 days after STZ administration (3 with 120 mg/kg STZ and 1 with 100 mg/kg STZ). Group 1 animals developed liver and kidney injury evidenced by increased alanine aminotransferase, aspartate aminotransferase, total cholesterol, LDL, triglyceride and blood urea nitrogen for one month, and histological abnormality including hepatic steatosis, renal glomerulus and tubular injury. Nevertheless, moderate histological injuries were seen in animals with 80 mg/kg STZ, with subsequent recovery. In contrast, group 2 animals displayed normal biochemical parameters and histology, with generally less risk of postoperative complications. We conclude that injection of 80 mg/kg STZ could induce diabetes with moderate injuries. Partial pancreatectomy with low-dose STZ is a safer and more reproducible method for inducing diabetes in rhesus monkeys.
Introduction
Type 1 diabetes mellitus (T1DM), which is the result of an autoimmune attack against the insulin-producing β cells of the endocrine pancreas, 1,2 is a common disease and the second most prevalent chronic illness in children. Current treatment for patients with T1DM is subcutaneous injection of recombinant DNA-derived insulin (T1DM is also termed insulin-dependent diabetes mellitus, IDDM). Islet transplantation can potentially permanently cure the disease. However, the shortage of human pancreas donors for transplantation is not likely to be alleviated soon. Consequently, IDDM continues to be a therapeutic challenge.
A reliable animal model of IDDM could be particularly helpful. 3 Non-human primates (NHPs) with induced diabetes can serve as ideal models because of their close phylogenetic relationship to humans and high similarities in metabolic, hormonal and pathological abnormalities 4,5 to diabetic patients.
IDDM is often induced by pancreatectomy and streptozotocin (STZ) administration. 6–8 However, total pancreatectomy is associated with high surgical morbidity and mortality. The tight adherence of the pancreas to the intestine in monkeys makes total pancreatectomy a difficult procedure, whereas the potential for continued functioning or regeneration of β cells in a partial pancreatectomy is also a big challenge for successful induction of IDDM. 9,10 STZ, derived from the bacteria Streptomyces achromogenes, is widely used to induce diabetes in NHPs. 9,11 . The compound is transported into β cells by the glucose transporter-2 receptor. 12,13 Therein, STZ induces DNA strands to break and subsequently activates repair mechanisms that result in a reduction in cellular nicotinamide adenine dinucleotide and subphysiological adenosine triphosphate levels, causing death of β cells. 14 The disadvantages of STZ are nephrotoxicity and hepatotoxicity, particularly at high dose. Therefore, there is a need to determine the optimal dose of STZ in NHPs.
Accordingly, in this study, we evaluated whether partial pancreatectomy or STZ administration (at doses of 80, 100 and 120 mg/kg) could more successfully and safely induce IDDM in rhesus monkeys.
Materials and methods
Animals
Thirteen male rhesus monkeys (age, 2–3 y; weight, 3.4–6.2 kg) were obtained from Chengdu Ping'an Experimental Animal Reproduction Center (Sichuan, China). All animals were maintained in the approved Experimental Animal Center at Sichuan University. Animals were housed in separate cages and fed monkey chow twice a day. The procedures described in this study were conducted according to the principles set forth by the Institute of Laboratory Animals Resources Guide for the Care and Use of Laboratory Animals.
Intravenous glucose tolerance tests
IVGTT was used to diagnose diabetes when normal animals were selected before STZ administration. Animals underwent IVGTT after overnight fasting and were anesthetized by an intramuscular ketamine injection (15 mg/kg body weight [BW]). A 20-gauge intravenous catheter was inserted into the greater saphenous vein and glucose at 0.5 g/kg BW was injected over 30 s. Blood samples were taken before glucose injection (0 min) and at 1, 3, 5, 10 and 30 min after glucose injection. The blood glucose (BG) levels were estimated at 0, 1, 3, 5, 10, 30, 60 and 120 min. Insulin and C-peptide were analyzed by radioimmunoassay.
Induction of diabetes
Thirteen rhesus monkeys were divided into two groups: group 1, single high-dose STZ administration (80, 100 and 120 mg/kg, n = 3 for each dose); group 2, partial pancreatectomy (70–75%) combined with low-dose STZ (15 mg/kg, n = 4).
Streptozotocin injection
Monkeys were fasted overnight. STZ (Yuyang High-tech Developing Co Ltd, Chengdu, China) was administered by intravenous injection after dissolution with citrate sodium at doses of 80, 100 and 120 mg/kg BW (n = 3 for each dose) over 30 s. BG levels were determined twice a day commencing 72 h after STZ induction. Hematological and serum biochemical parameters were assessed once a month. Serum C-peptide levels were measured by radioimmunoassay.
Partial pancreatectomy combined with low-dose STZ
The procedure for partial pancreatectomy was consistent with that for total pancreatectomy as described by Qiao et al. 15 with some modifications. The pancreas was dissected but the caput pancreatis and uncinate process were reserved. Tramadol hydrochloride injection (100 mg intramuscularly every 12 h) was administered for postoperative analgesia within 24 h and total parenteral alimentation was given for three days. Sutures were removed seven days after surgery. The low-dose STZ administrations (15 mg/kg BW, 1–5 times every 4 days) via intravenous injection were performed based on the postoperative BG levels. 15
Animal models were considered to be successfully established if the fasting blood glucose (FBG) values remained >11.1 mmol/L for two consecutive days and the C-peptide concentration was <0.5 nmol/L.
After successful induction of diabetes, monkeys were treated with porcine insulin (Wanbang Biopharma Co Ltd, Xuzhou, China) to avoid metabolic dysfunction and maintain good general condition. Routine complete blood count and serum biochemical testing were performed periodically before and after diabetes induction. If any animal appeared to have multiple organ failure in the experiment, euthanasia would be performed in order to reduce their suffering.
Abdominal computed tomography scan
Abdominal computed tomography scans were carried out according to Qiao et al. 15 The monkeys were examined with non-contrast-enhanced abdominal spiral computed tomography (CT) scans through a bolus injection of iohexol 10 s before the contrast-enhanced CT scan. The location and condition of the pancreas before and after surgery were compared. 15
Arginine stimulation test
Arginine stimulation test (AST) was performed before and after STZ administration, helping to judge the function of β cells. AST used an intravenous injection of 2 g arginine (Jinyao amino acids Co Ltd, Tianjin, China) administered over 30 s with time 0 set at the beginning of the arginine injection. Blood samples were collected at 0, 2, 3, 4, 6, 8 and 10 min after arginine injection. Acute insulin response to arginine was defined as the peak insulin value following the arginine injection minus the basal value.
Histology
Biopsies were carried out one month after the animals developed diabetes. Samples of the pancreas, kidney and liver were fixed in 10% formalin, embedded in paraffin, sectioned and stained with hematoxylin and eosin. Pancreas tissues were stained for insulin and glucagons by immunohistochemistry.
Statistical analysis
All data are presented as mean values ± standard deviation at three stages (normal, after STZ and insulin control). The results were analyzed using one-way analysis of variance. P values <0.05 were considered to be significant.
Results
Mortality
All three animals of the STZ 120 mg/kg group and one of three animals of the STZ 100 mg/kg group died within 8–14 days (the mortality was 100% and 33.3%, respectively). All animals survived in the STZ 80 mg/kg group and the partial pancreatectomy combined with low-dose STZ (15 mg/kg BW) group.
Single high-dose STZ to induce diabetes
After STZ injection, all animals in group 1 developed diabetes within a week. After five days, the average FBG level of animals increased from 4.34 ± 0.37 to 19.93 ± 5.03 mmol/L (P < 0.01), and the serum C-peptide levels decreased from 4.30 ± 2.12 to 0.08 ± 0.07 nmol/L (P < 0.01). After insulin administration twice a day, the FBG returned to 6.48 ± 1.49 mmol/L.
The results of diabetes induction were confirmed by histological observation of the pancreas after STZ injection. In the STZ 80 mg/kg group, the number of normal islets was reduced. The endochylema of islets appeared to have granular degeneration and even necrosis (Figure 1D). In the STZ 100 mg/kg group, we observed more serious necrosis and disappearance of islet cells. The normal structure of islets was destroyed (Figure 1G), characterized by rare insulin-positive staining (Figures 1F and I) and increased staining for glucagon (Figures 1E and H).
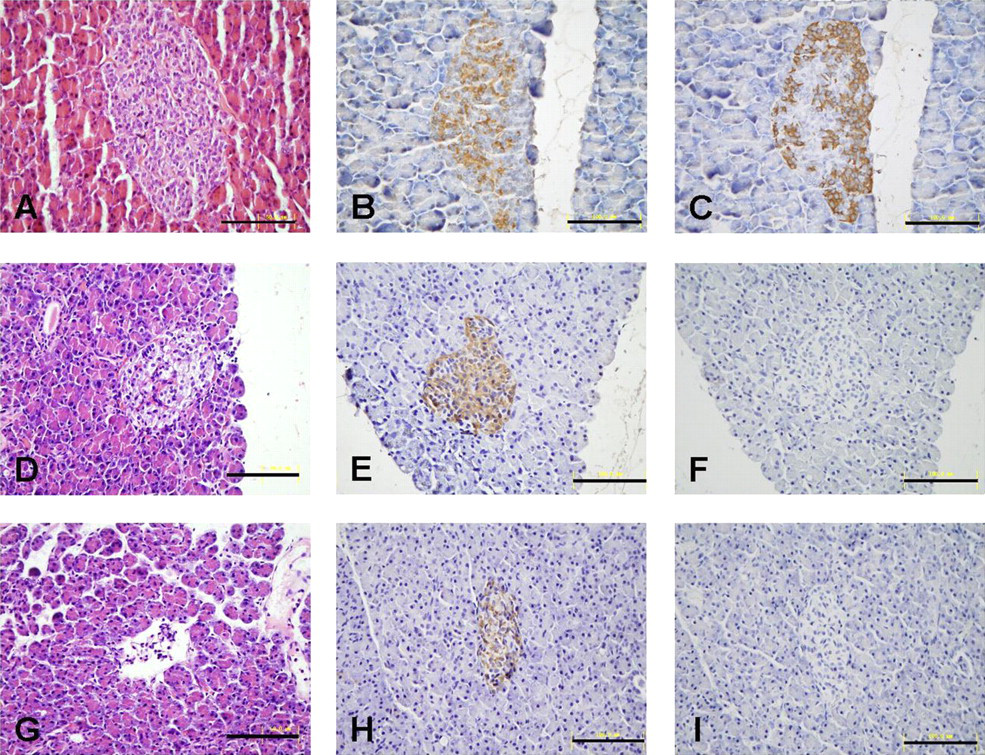
Histology (H&E stain) and immunohistochemistry of pancreatic biopsies of STZ treated and normal monkeys. Normal monkey islets (A) (n = 13) show normal glucagons (B) and insulin (C) stain. In the STZ80 group (n = 3), the number of normal islets is reduced. The islet cells appeared to have granular degeneration and even necrosis (D). Islets show rare insulin-positive cells (F) and increased glucagon stain (E). In the STZ100 group (n = 3), there are few infiltrating inflammatory cells. Islets display necrosis with destructed structure and even disappeared (G). In remaining islets, almost no insulin-positive cells were found (I) and glucagon staining cells were increased (H) (black scale bar: 100 μm). (Pancreatic biopsies were performed on each animal in each group. We found similar islets damages in these animals, so we chose the typical figures to show the islets' condition.) H&E, hematoxylin and eosin; STZ, streptozotocin (A color version of this figure is available in the online journal)
To confirm the persistence of diabetes in animals, IVGTT and AST were performed before and after STZ injection, respectively. The findings showed normal insulin secretion and BG curves before STZ injection (Figures 2a–d), and abnormal insulin release and BG values after STZ injection (Figures 2e and f). Insulin levels during the AST were lower in the STZ100 group than in the STZ80 group.

Insulin secretion and blood glucose of IVGTT and AST. Insulin secretion and blood glucose during the IVGTT and AST in normal animals were shown as control group (a–d), and during the AST in diabetic animals were shown as (e) and (f), respectively. Group 2: partial pancreatectomy combined with low-dose STZ. IVGTT, intravenous glucose tolerance test; AST, arginine stimulation test; STZ, streptozotocin
Hematological and serum biochemical parameter before and after STZ injection are shown in Table 1. After STZ administration, animals developed liver and kidney injury evidenced by increased alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum creatinine (CREA), total cholesterol (T-CHOL), lactate dehydrogenase (LDH), low-density lipoprotein (LDL), triglyceride (TG), uric acid (UA) and blood urea nitrogen (BUN) for one month.
Complete blood count and serum biochemical parameters before and after high-dose STZ administration (group 1)
STZ, streptozotocin; WBC, white blood cells; NEU, neutrophilic granulocyte, neutrophil; LYM, lymphocyte; MONO, monocyte; EOS, eosinophils; BASO, basophilic cells; RBC, red blood cells; HGB, hemoglobin; HCT, hematocrit; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; PLT, platelet; PDW, platelet distribution; ALB, albumin; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; DBIL, direct bilirubin; CREA, creatinine; T-CHOL, total cholesterin; CK, creatine kinase; GGT, γ-glutamyltransferase; GLU, glucose; HDL, high-density lipoprotein; LDH, lactate dehydrogenase; LDL, low-density lipoprotein; TBIL, total bilirubin; TP, total protein; TG, triglyceride; UA, uric acid; BUN, blood urea nitrogen
*Mean difference is significant at the 0.05 level when the group of seven days after STZ is compared with insulin control group
†Mean difference is significant at the 0.05 level when the group of seven days after STZ is compared with normal group
‡Mean difference is significant at the 0.05 level when insulin control group is compared with normal group
Partial pancreatectomy with low-dose STZ to induce diabetes
The average weight of the excised pancreatic tissue of the rhesus monkeys was 10.8 g. The FBG values fluctuated between 3.3 and 21.6 mmol/L after the partial pancreatectomy and returned to normal within three days. An abdominal CT scan showed that the head of the pancreas still remained. After one to five times injection of STZ (15 mg/kg), FBG levels increased to 19.53 ± 2.72 mmol/L (P < 0.01), while serum C-peptide levels decreased to 0.35 ± 0.06 nmol/L (P < 0.01). After insulin administration, the FBG returned to 6.73 ± 1.10 mmol/L.
Hematological and serum biochemical parameter before and after STZ injection are shown in Table 2. To confirm the persistence of diabetes, IVGTT and AST were performed before and after STZ injection, respectively. The IVGTT showed normal insulin secretion and BG curves before STZ injection (Figures 2a and b), but lower insulin secretion and abnormal BG after STZ injection (Figures 2e and f).
Complete blood count and serum biochemical parameters before and after low-dose STZ administration (group 2)
STZ, streptozotocin; WBC, white blood cells; NEU, neutrophilic granulocyte, neutrophil; LYM, lymphocyte; MONO, monocyte; EOS, eosinophils; BASO, basophilic cells; RBC, red blood cells; HGB, hemoglobin; HCT, hematocrit; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; PLT, platelet; PDW, platelet distribution; ALB, albumin; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; DBIL, direct bilirubin; CREA, creatinine; T-CHOL, total cholesterin; CK, creatine kinase; GGT, γ-glutamyltransferase; GLU, glucose; HDL, high density lipoprotein; LDH, lactate dehydrogenase; LDL, low-density lipoprotein; TBIL, total bilirubin; TP, total protein; TG, triglyceride; UA, uric acid; BUN, blood urea nitrogen
*Mean difference is significant at the 0.05 level when the group of after low-dose STZ is compared with normal group
†Mean difference is significant at the 0.05 level when the group of after low-dose STZ is compared with insulin control group
‡Mean difference is significant at the 0.05 level when insulin control group is compared with normal group
Diabetes status induced by different methods
Animals in both groups developed diabetes with FBG levels >11.1 mmol/L after induction. There was no statistical difference in BG levels after STZ injection between the two groups. Serum C-peptide levels in both groups decreased from 4.30 ± 2.12 to 0.08 ± 0.07 and 0.35 ± 0.06 nmol/L, respectively (P < 0.01). The findings showed that these two methods can successfully induce diabetes in rhesus monkeys, which was confirmed by the AST analysis (Figure 2).
After the successful induction of diabetes, monkeys were treated with identical doses of porcine insulin to avoid metabolic dysfunction and maintain a good general condition for islets transplantation. In the statistical analysis, we considered one day's observation of one monkey as a unit (one monkey-day). Over 1617 monkey-days, there were no cases of hypoglycemia in group 2. However, over 1626 monkey-days, there were seven cases of hypoglycemia in group 1, which corresponded to a frequency of 0.43 (time/hundred monkey-days).
The hematological and serum biochemical parameters showed higher BUN, UA, CREA, ALT and AST levels for group 1 than that for group 2. The results indicated that kidney and liver injuries were more severe in animals of group 1 (Table 3).
Comparisons of the complete blood count and serum biochemical parameters between groups 1 and 2
WBC, white blood cells; MCV, mean corpuscular volume; MCH, mean corpuscular hemoglobin; MCHC, mean corpuscular hemoglobin concentration; ALB, albumin; ALT, alanine aminotransferase; AST, aspartate aminotransferase; DBIL, direct bilirubin; CREA, creatinine; HDL, high-density lipoprotein; LDH, lactate dehydrogenase; LDL, low-density lipoprotein; TG, triglyceride; TBIL, total bilirubin; UA, uric acid; BUN, blood urea nitrogen
*Mean difference is significant at the 0.05 level when the group 1 compared with group 2
Liver and kidney biopsies from animals of group 1 showed hepatic steatosis, renal glomerulus and tubular injury (Figures 3C, D and 4C, D). In contrast, biopsies from animals of group 2 showed little liver and kidney injuries (Figures 3B and 4B). The results confirm that induction of diabetes using partial pancreatectomy combined with low-dose STZ is safer and has a lower risk of complication than using high-dose STZ to induce diabetes in rhesus monkeys.

Histology of liver biopsies (H&E stain). (A) Normal monkeys (n = 13), (B) partial pancreatectomy combined with low-dose STZ group (n = 4), (C) STZ80-treated monkeys (n = 3) and (D) STZ100-treated monkeys (n = 3). The liver of monkeys with partial pancreatectomy combined with low-dose STZ shows normal structure, but partial hepatocyte endochylema shows lipid droplets. The liver of monkeys with high-dose STZ shows marked steatosis (black scale bar: 50 μm). (Each animal in each group developed similar liver injuries after STZ injection. In the results, we chose the typical pictures to show the injuries.) H&E, hematoxylin and eosin; STZ, streptozotocin (A color version of this figure is available in the online journal)
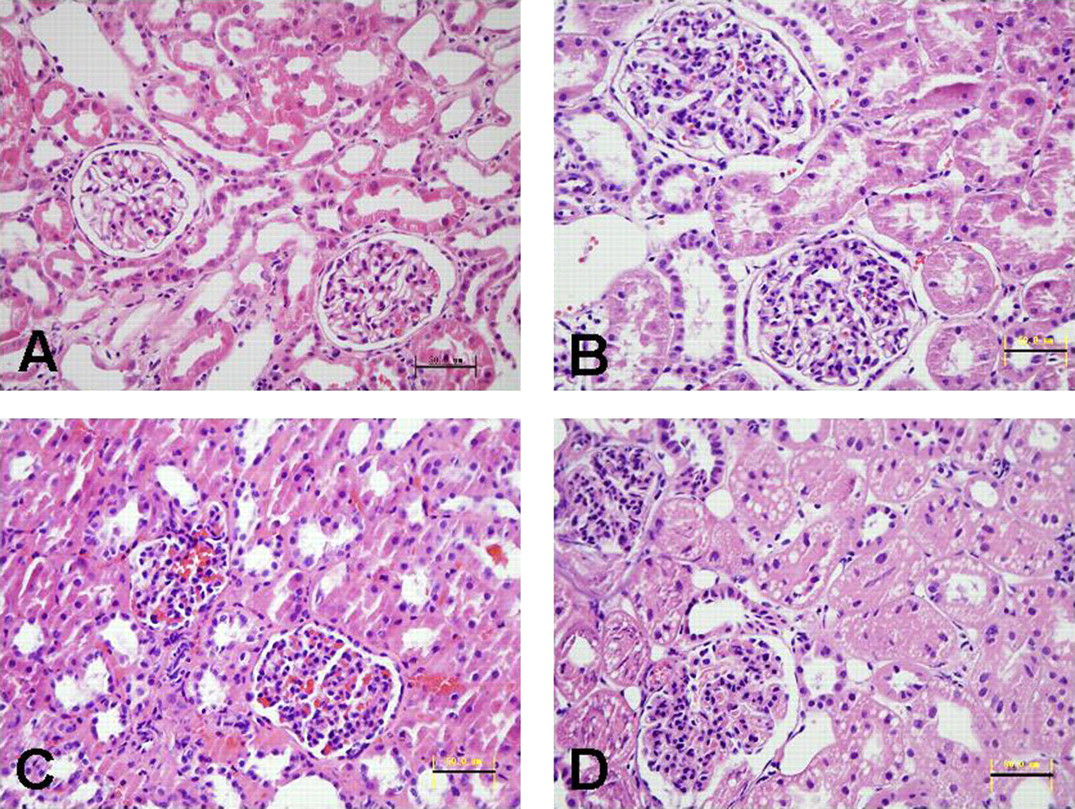
Histology of kidney biopsies (H&E stain). (A) Normal monkey kidney (n = 13), (B) the kidney from group 2 of partial pancreatectomy combined with low-dose STZ (n = 4) shows renal glomerulus intumescence with few infiltrating inflammatory cells, (C) in the high-dose STZ80 group (n = 3), renal glomerulus appears hypertrophic with infiltration of inflammatory cells and glomerular capillary swells, dilates and congests and (D) the kidney from high-dose STZ100 group (n = 3) shows hypertrophy of renal glomerulus with inflammatory cell infiltration, and tumescence of tubular epithelial cell and glomerular capillary accompanying lipid droplets (black scale bar: 50 μm). (Each animal in each group developed similar kidney injuries after STZ injection. In the results, we chose the typical pictures to show the injuries.) H&E, hematoxylin and eosin; STZ, streptozotocin (A color version of this figure is available in the online journal)
Discussion
STZ is widely used to induce diabetes in animals, but the optimal dose of STZ in NHPs is still undetermined. Reports show that a dose of 55–150 mg/kg STZ can successfully induce diabetes, but with some adverse reactions and complications. 3,16–19 However, our results are inconsistent with these studies: three monkeys induced by 120 mg/kg STZ and one of three animals injected with 100 mg/kg STZ died of acute pancreatitis and acute liver and kidney injury within 8–14 days, accompanied by increased BUN, UA, TG, CREA, AST and ALT. Shibata et al. 3 reported that the 100 mg/kg STZ administration failed to develop diabetes, evidenced by a virtually unchanged basal insulin. However, in our study, we successfully induced diabetes with 80 and 100 mg/kg STZ. Results of the AST showed very low insulin secretion compared with normal animals. The discrepancy between our results and the above studies may be attributed to the differences in the species and ages of the monkeys and the different manufacturers of STZ we used. Total pancreatectomy is also commonly used to induce diabetes in preclinical models. 20 However, it is a technically difficult operation and causes complete exocrine and endocrine deficiency, 10 which may result in high risk of operative complications and mortality. 10,21,22 In our study, we used partial pancreatectomy combined with low-dose STZ to induce diabetes and avoid the complications and mortality caused by total pancreatectomy. In partial pancreatectomy, the head and uncinate process of pancreas are reserved in order to prevent damage to important blood vessels and the bile duct system. This method not only reduces the difficulties and risks of total pancreatectomy, but also partially preserves the exocrine glandular function, which helps postoperative recovery. 15 The remaining pancreatic β cells would be destroyed by low-dose STZ to avoid liver and kidney damage in monkeys caused by high-dose STZ. Monkeys that underwent partial pancreatectomy combined with low-dose STZ had normal serum biochemical parameters and histology (Table 2, Figures 3 and 4), indicating considerably less kidney and liver injury, and the risk of obviously reduced complications.
After the successful induction of diabetes, monkeys were administered porcine insulin to avoid metabolic dysfunction and to maintain a good general condition for islet transplantation. Although there was no difference in the dose of exogenous insulin between the two groups, different hypoglycemic incidences were observed. There was no hypoglycemia in the group of partial pancreatectomy combined with a low-dose STZ, but the incidence of hypoglycemia for the high-dose STZ group was relatively high (0.43 time/hundred monkey-days). This suggests that the method of partial pancreatectomy combined with low-dose STZ to induce diabetes is more stable and safer. The possible reason for the different risk of hypoglycemia between the groups may be that the two methods destruct the pancreatic islets at different patterns and cause diverse pathophysiologies of diabetes.
In conclusion, we successfully induced diabetes in rhesus monkeys using two methods: high-dose STZ administration and partial pancreatectomy combined with low-dose STZ administration. Single high-dose STZ injections (80 mg/kg) could induce diabetes with moderate injuries, whereas partial pancreatectomy combined with low-dose STZ may be a safer, more reproducible and more stable method to induce diabetes in rhesus monkeys.
Footnotes
ACKNOWLEDGEMENTS
This study was supported by the National Program for High Technology Research and Development of China (No. 2006AA02A117), Key program of National Nature Science Foundation of China (No. 30930088) and Program of Natural Science Foundation of China (No. 30872382).