
Abstract
Genes could be used to treat atherosclerosis. The key problem is how to target a gene through the walls of arteries in free-flowing blood. TFPI-2 has been shown to suppress thrombosis and arterial re-stenosis, which indicates its potential function in gene therapy for atherosclerosis. The microbubble ultrasound contrast agent is widely applied in diagnostic imaging, and could be used for transferring genes into arteries. By transfecting TFPI-2 into arteries using SonoVue (a kind of microbubble ultrasound contrast agent), we identified TFPI-2 as an available factor for inhibiting the proliferation of vascular endothelial cells in vivo. Compared with adenovirus, SonoVue showed similar gene transfection efficiency, but the latter showed stronger inhibition of thrombosis and arterial re-stenosis with a high expression of TFPI-2 protein in vitro and in vivo. SonoVue was less damaging when transfecting genes into the arterial wall. These data indicate that transfecting human TFPI-2 into the arterial wall may suppress thrombosis and arterial re-stenosis, and reduce atherosclerosis.
Keywords
Introduction
Atherosclerosis is characterized by thrombosis and arterial re-stenosis within the intima of the arterial wall, and is a multifactorial chronic inflammatory disease. 1 It is the leading cause of morbidity and mortality worldwide. To suppress thrombosis and arterial re-stenosis, 2 targeting a drug or gene through the walls of arteries in free-flowing blood is believed to be feasible for atherosclerosis treatment. There is currently no ‘ideal’ treatment for atherosclerosis. Gene therapy for atherosclerosis has been studied extensively, 3 but clinical application has not transpired.
It is well known that tissue factor (TF), a transmembrane protein that triggers blood coagulation in vivo, 4 contributes to atherosclerosis development. 5 TFPI-2 inhibits TF activity by forming a TF–FVIIa–FXa–TFPI complex, which causes sustained repression of the TF pathway and regulates digestion and remodeling of the extracellular matrix. 6 Both FVIIa and FXa are active factors of FVII and the FX, respectively, which are two enzymes of the coagulation cascade. Therefore, TFPI-2 is a potential mechanism for preventing atherosclerosis. TFPI-2 may therefore be a candidate gene for suppressing thrombosis and arterial re-stenosis. Transporting the candidate gene into the targeted diseased tissue for reversal of the features of atherosclerosis is the main barrier.
The interaction of microbubble contrast agents with ultrasonic waves has been extensively studied, mostly in diagnostic imaging. 7,8 Insonation of microbubbles can produce liquid jets and local shear stress, which would alter biological membranes and facilitate gene transport into cells. 9,10 Insonation of microbubbles may therefore be a potential method of gene delivery into arterial walls.
In the present study, we successfully delivered the TFPI-2 gene by SonoVue (a kind of microbubble ultrasound contrast agent, Bracco Imaging B.V., Geneva, Switzerland) and observed the effects of this atherosclerosis gene therapy strategy in vitro and in vivo.
Materials and methods
Plasmid construction
Construction of pEGFP-TFPI-2, pcDNA3.1-TFPI-2 and Ad-EGFP-IRES-TFPI-2
The 753-bp human TFPI-2 gene (NM_001032281, Proteintech Group Inc, Chicago, IL, USA) was inserted into compatible enzyme restriction sites (XhoI and BamHI) of pEGFP-N1 (Invitrogen Life Technologies, Carlsbad, CA, USA) to generate pEGFP-TFPI-2. The forward primer was TGTGGGATCCATGATTTACACAATGAAG and the reverse primer was TATACTCGAGCGACATAGGCATGAAATGCTATC, the polymerase chain reaction (PCR) product of TFPI-2 gene was digested with restriction enzymes BamHI and XhoI and the desired fragment was cloned into pcDNA3.1 (Invitrogen Life Technologies) to generate pcDNA3.1-TFPI-2. The Ad-EGFP-IRES-TFPI-2 recombinants were prepared as described 11 using the AdEasy-1 System Kit (Stratagene, La Jolla, CA, USA). Constructed plasmids were confirmed by DNA sequencing. High-purity plasmids were prepared on a large scale in the experiments described below.
Animals
Healthy New Zealand white rabbits of both sexes (∼2.5 kg) were obtained from the Center of Medical Experimental Animals (Hubei Province, China). They were maintained in our laboratory under standard conditions. All rabbit studies were approved by the Institute of Animal Care and Use Committee. Intravenous injection of pentobarbital sodium (25 mg/kg; Invitrogen, Carlsbad, CA, USA) was used for anesthesia in all animals. Animals in all control groups were still examined with conventional baseline ultrasound using carotid artery examination settings.
In the damage-mode group, there were six rabbits whose right carotid artery constituted a damage-mode group and the contralateral side was used as a control.
In vivo, the transfection efficiency group had 18 rabbits, which were divided into three groups: control group (n = 6), adenovirus group (n = 6) and SonoVue group (n = 6). No other treatment was applied to the animals in the control group except anesthesia and shaving. Animals in the adenovirus group were transfected by Ad-EGFP-IRES-TFPI-2. The pEGFP-TFPI-2 plasmids were transfected into the SonoVue group of animals.
A total of 30 rabbits, being used for the analysis of thrombosis and re-stenosis of arteries, were divided into five groups: first group (n = 6), second group (n = 6), positive group (n = 6), SonoVue group (n = 6) and adenovirus group (n = 6). Rabbits that did not receive any treatment were the first negative control group. The second negative control group was treated by phosphate-buffered saline (PBS) (pH 7.4), plasmids and ultrasound. The damage-mode group was the third group and considered to be the positive control. The SonoVue group received treatment of plasmid, SonoVue and ultrasound. The adenovirus group animals were infected by adenovirus.
SonoVue adherence ratio to plasmids
To evaluate the adherence ratio of SonoVue, varying amounts of SonoVue (45 μg/mL), which were prepared according to the manufacturer's instructions, were mixed with the same amount of plasmids (1 μg/μL). The total volume was the same after 0.9% sodium chloride (NaCl) solution was added to each mixture (Table 1). The mixture was incubated for 15 min at room temperature and separated into two layers. The upper layer is a very thin white layer that SonoVue adhere to plasmids. The down layer is a thick solution including plasmids. After incubation, using ultraviolet spectrophotometry to test the plasmid concentration in the down layer, absorbency (A) of every mixutre was measured using the optical density at 260 nm (A
260) and 280 nm (A
280). Using the equation

Procedure of the SonoVue adherence ratio
Tube 0 was the blank one. All tubes of the adherence ratio were high, and tube 2, tube 3 and tube 4 of the adherence ratio were higher than tube 1. Tube 1 of the adherence ratio was about 10% as low as that of tube 2, tube 3, tube 4 and tube 5
Baseline and contrast-enhanced ultrasonography examination 12
A clinical ultrasound scanner (Siemens Acosun Sequia512, Siemens, Germany) and a convex probe with a frequency range of 10–14 MHz (15L8W-S, Siemens) were used in the present study. For baseline ultrasound examination, the conventional carotid artery examination mode was used, and the mechanical index (MI) was 1.5 as read on the screen. The carotid artery was scanned thoroughly with baseline ultrasound for five minutes. The imaging settings of the ultrasound scanners were optimized to get the best depiction of the carotid artery (Table 2). For low MI real-time contrast-enhanced ultrasonography (CEUS) examination, the contrast pulse-sequencing imaging mode was used and MI was 0.18 as read on the screen. SonoVue was used as a contrast agent. After the initiation of contrast-specific imaging mode, the imaging settings, including the depth and focus, were readjusted for best visualization of the carotid artery (Table 2). A volume of 0.2–0.3 mL (0.1 mL/kg) of a contrast agent was injected into the ear vein in 10 s, followed by a flush of 2 mL of 0.9% normal saline solution. No animal received an additional administration of the contrast agent in this study. The timer was activated simultaneously at the beginning of ultrasound contrast agent (UCA) administration. The carotid artery was first observed continuously for five minutes after UCA administration as a vascular phase, and then from the 10th to 15th min as a Kupffer phase under contrast-specific imaging, and high MI (1.5) imaging mode for three minutes to break the microbubbles in the end. The digital cine clips of both baseline grey-scale ultrasound and the whole process of CEUS images were stored in the hard disk incorporated in the scanner.
Setting of ultrasound scanner used in the study
Parameter setting of ultrasound scanner in the study
CEUS, contrast-enhanced ultrasonography; MI, mechanical index
Arterial tension
Examination of arterial tension (Dual Wire Myograph System-410A, DMT-USA Inc, Atlanta, GA, USA) was used to estimate artery function. Measurement of arterial tension was carried out as reported. 13 Acetylcholine (ACh) stimulates endothelium cells to produce nitric oxide, which can cause smooth muscle relaxation. By testing arterial tension, the arterial endothelium of function can be indirectly posted out. So the ACh was applied to test the tension in this study. The tension changes in the arteries in the control group and other experimental groups by different doses of ACh can show the arterial function in each group.
Transfection efficiency in vitro and in vivo
To compare the efficiency of different transfection methods in vitro, transfection of pEGFP-TFPI-2 into human umbilical vein endothelial cells (HUVECs) (China Type Culture Collection) by liposome (Invitrogen) was carried out following the manufacturer's protocol. The ratio of liposome to plasmid was 4 μL to 1 μg. 14 The other two methods, SonoVue and adenovirus, were carried out in parallel to transfer pEGFP-TFPI-2. The ratio of SonoVue to plasmid was 200 μL to 4 μg, and the diagnostic ultrasound of the mechanical index was 1.5. 15 Cells were transfected with Ad-EGFP-IRES-TFPI-2 at a multiplicity of infection (MOI), which is the ratio of infectious agents (e.g. phage or virus) to infection targets (e.g. cell), of 200 plaque-forming unit (pfu)/cells. 11 After 48 h, the assortment of treated cells was observed and imaged using a fluorescence microscope for detecting transfection efficiency by EGFP expression. Reverse transcriptase (RT)-PCR 16 and Western blotting 4 were used to detect TFPI-2 expression.
In vivo, the efficiency of the two transfection methods, SonoVue and the adenovirus method, was evaluated by transfecting the TFPI-2 gene into the wall of the common carotid artery wall. Initially, the pEGFP-TFPI-2 plasmid was delivered into the arterial endothelium by SonoVue. The ratio of SonoVue to plasmid was 10 μg to 40 μL. After the SonoVue mixture was injected into the origin of the otogenic vein, the common carotid artery was quickly exposed for three minutes under ultrasound (set at the diagnostic ultrasound at a mechanical index of 1.5). The adenovirus method was used to carry the Ad-EGFP-IRES-TFPI-2 into the arterial wall. The 0.5 mL adenovirus solution (at a MOI of 200 pfu/cell) was placed for one hour in a special segment of the common carotid artery, which was similar to the artery mode segment but damaged using a 2.0 Fogarty catheter. The artery mode segment is damaged at a segment of the common carotid artery for artery endothelium proliferation. Control group rabbits were left untreated. The artery experimental segments were harvested after the transfection of 48 h. Fast-frozen sections were prepared for viewing EGFP expression using fluorescence microscopy and for testing the TFPI-2 level in arterial tissue by Western blot.
Damage mode on the right common carotid artery
After the damage-mode group rabbits were anesthetized, and a mid-cervical incision was made, the right common carotid artery and its bifurcation were exposed. To prevent acute thrombosis during the procedure, heparin sodium (200 IU/kg) was intravenously injected five minutes before the balloon injury. The right common carotid artery was balloon-injured three times with a 2 F balloon catheter (2 F Fogarty, Baxter Healthcare Corp., Santa Ana, CA, USA) inserted through the external carotid artery. Two vascular clips were placed at the distal end and in the middle of the injured arterial segment. A 24-gauge annula was introduced into the common carotid artery via the external carotid artery. The lumen of the injured segment between the two clips (10 mm long) was washed with 9.57 mmol/L PBS. Then the instillate was retrieved, the cannula was removed and the blood flow was restored. After confirmation of the carotid arterial flow, the wound was sutured. All procedures were performed under sterile conditions. Intra-muscular injection of penicillin solution (80 pan-U/day) was given for three days to prevent infection. Ultrasound, tension testing and pathological methods were used to examine the arteries of the damaged mode and the control group after 10 days. 17
Suppression of arterial thrombosis and re-stenosis by TFPI-2
To examine TFPI-2 suppression in vivo, arteriae carotis communis of damage mode (used to test if TFPI-2 inhibits proliferation of artery-damaged endothelium) was established to mimic the positive group of atherosclerosis.
Rabbits were divided into five groups. The first negative group rabbits did not receive any treatment. Like the SonoVue group method for testing transfection efficiency above, the mixture of PBS and plasmids replacing the solution of SonoVue and plasmids were transfected into the second group rabbit carotid arteries. The damage-mode group was the third group and considered to be the positive control. Like the transfection efficiency method of SonoVue and Adenovirus groups, the TFPI-2 gene was transfected into the arterial endothelium of the SonoVue and Adenovirus groups. After 24 h the two group rabbits of carotid arteries were damaged as the mode group. All the rabbits' wounds were washed with gentamicin sodium chloride (1.6 mg/mL) and sutured. Intra-muscular injection of penicillin solution (80 pan-U/day) was given for three days to prevent infection. On the tenth day, five group rabbits of arterial tissue were checked by ultrasound and assessed for arterial tension, pathology and Western blot.
Statistical analysis
All experiments were carried out at least three times. Results are mean ± standard deviation. An unpaired Student t-test was carried out to determine statistical significance. P < 0.05 was considered significant.
Results
SonoVue adherence rate
The adherence of SonoVue was analysed by ultraviolet spectrophotometery. Different doses (0, 5, 10, 15, 20 and 25 μL) of SonoVue (45 μg/mL) were mixed with 1 μg plasmid DNA. Three doses of SonoVue (10, 15 and 20 μL) showed the highest efficiency of plasmid adherence (90.1%; Table 1). From the standard curve of SonoVue adherence ratio (Figure 1a), the SonoVue adherence ratio increased by linearity (between 0 and 10), ranged from 0% to 90.1% and at the point of 25 it was 88.5%.

SonoVue adherence ratio and efficiency of transferring pEGFP-TFPI-2 into human umbilical vein endothelial cells. (a) As shown in Table 1, the standard curve of SonoVue adherence ratio was performed. The x axis is the volume ratio of SonoVue and plasmids, and the y axis point to the SonoVue adherence ratio. (b) Using visible light and blue excitation light, each group of cells was observed in the same visual field and photographed by fluorescence microscopy. (c) The transferring efficiency of SonoVue and adenovirus groups was higher than in all other groups. Between the two former groups, SonoVue proved to have the higher transferring efficiency. These data are representative of three independent experiments. n = 3. **P < 0.01, *P < 0.05 (A color version of this figure is available in the online journal)
Transfection efficiency and expression of TFPI-2 in HUVECs
Compared with the liposome transfection method, transfection efficiencies were significantly higher using the SonoVue and adenovirus. SonoVue and adenovirus did not show differences in transfection efficiency. Transfection efficiency of the control, liposome, SonoVue and adenovirus groups were 0 ± 3.3%, 22 ± 2.3%, 73 ± 3.6% and 77 ± 4.2% transfected cells, respectively (Figure 1b and c).
To determine the levels of TFPI-2 expression in different groups, RT-PCR and Western blot were carried out. Standardizing against β-actin, the electrophoresis strips' greyscale values of RT-PCR and Western blotting reaction products for the TFPI-2 gene were obtained from Bio-Rad image system analysis (Bio-Rad Laboratories Inc, Philadelphia, PA, USA). The RT-PCR values for the control, liposome, SonoVue and adenovirus groups were 0.58 ± 0.08, 0.72 ± 0.06, 1.56 ± 0.17 and 1.63 ± 0.20, respectively (Figure 2a). Levels of TFPI-2 mRNA from the SonoVue and adenovirus groups were significantly higher than those of the control and liposome groups, but there were no differences among the SonoVue and adenovirus groups. Western blotting of the SonoVue and adenovirus TFPI-2 protein expression was greater than in the other groups. The respective Western blotting ratios (the control, liposome, SonoVue and adenovirus groups) were 0.31 ± 0.05, 0.42 ± 0.08, 0.84 ± 0.10 and 0.88 ± 0.09, respectively (Figure 2b). These results supported a viable method for transfecting TFPI-2 into the arterial endothelium.

Expression of transferring pEGFP-TFPI-2 into human umbilical vein endothelial cells. TFPI-2 mRNA (a) and protein (b) levels in the SonoVue and adenovirus groups were higher than in the other tested groups. These data are representative of three independent experiments. n = 3. **P < 0.01, *P < 0.05 (A color version of this figure is available in the online journal)
Assessing the transfection efficiency of TFPI-2 in vivo
To examine if pEGFP-TFPI-2 could be transfected into the artery by SonoVue in flowing blood in vivo, the transfection of pEGFP-TFPI-2 plasmid into the arterial endothelium was carried out. The fluorescence intensity of the SonoVue group was much higher than that of the adenovirus group (Figure 3a). According to a peak ratio of TFPI-2 to β-actin, the adenovirus, control and SonoVue group values were 0.42 ± 0.07, 0.31 ± 0.05 and 1.2 ± 0.13, respectively. Protein expression was increased more in the SonoVue group than in the adenovirus group (Figure 3b), demonstrating that the pEGFP-TFPI-2 plasmids had been successfully transfected into arterial tissue using the SonoVue method.
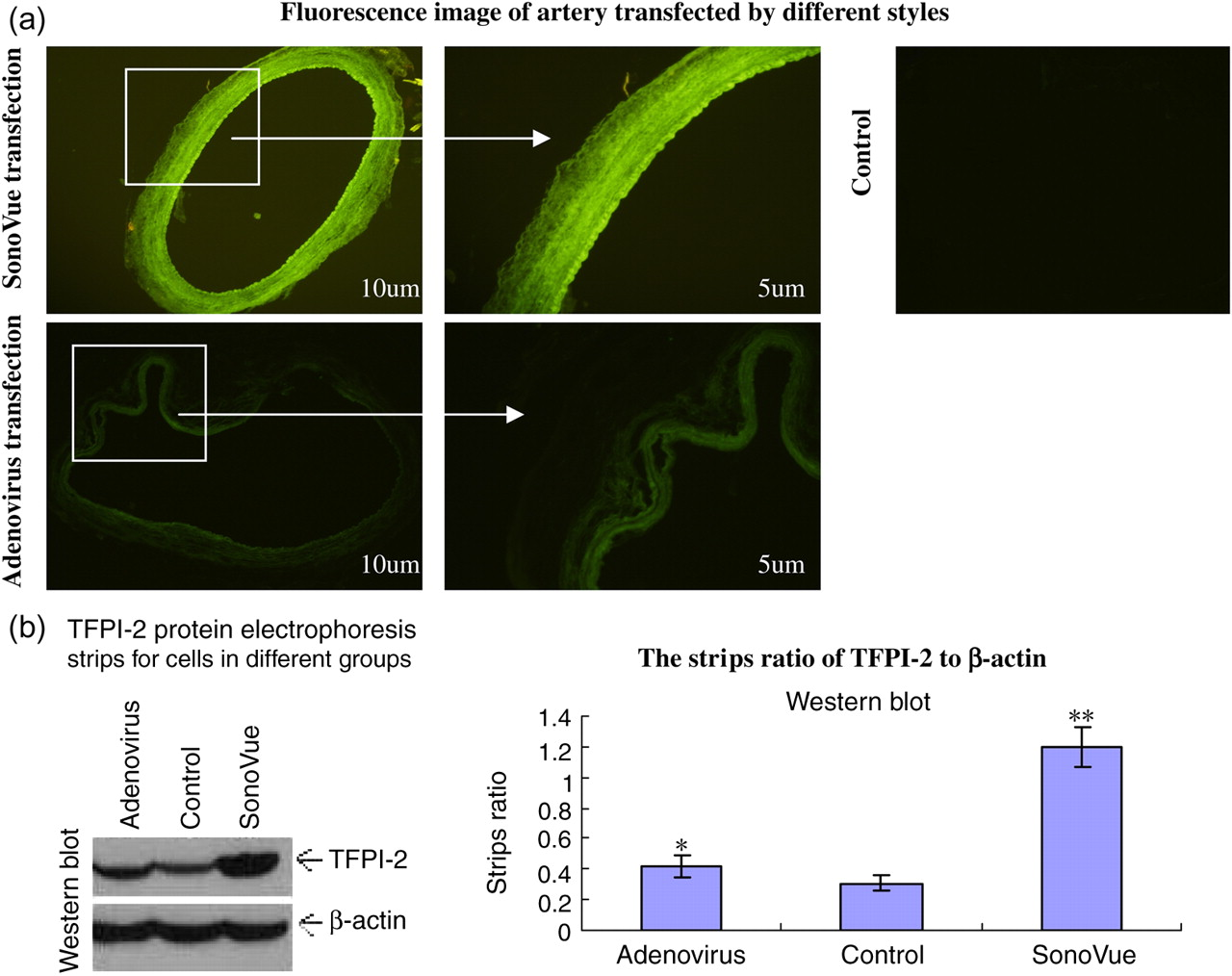
(a) Efficiency of transferring TFPI-2 into the artery using different methods. Using fluorescence images, the SonoVue group showed an intensity that gradually increased from the intima to the adventitia of the artery. SonoVue also showed the greatest fluorescence compared with all the other groups. (b) Western blot assay of transferring TFPI-2 into the artery. The TFPI-2 protein level in the SonoVue group was the highest in all the groups. These data are representative of three independent experiments. n = 3. **P < 0.01, *P < 0.05 (A color version of this figure is available in the online journal)
Artery damage-mode analyses
Before the experiments, a rabbit model of a damaged carotid artery was established to test whether TFPI-2 could suppress thrombosis and re-stenosis of the artery (data not shown). The lumen of the damage-mode artery had more plaques and lower tension than that of the control artery, in which there were no plaques (Figure 4a). Relative to the control, the damage-mode arterial tension significantly decreased (Figure 4b). Histological images indicated that the lumen of arterial endothelium in the damage-mode group was increased by about 2 mm compared to the control in which there was no increase (Figure 4a). The damage-mode arterial diameter decreased more, but the blood flow velocity was higher than the control one (Table 3). These data suggested that the arteriae carotis communis of the damage-mode artery would be appropriate for subsequent experiments.
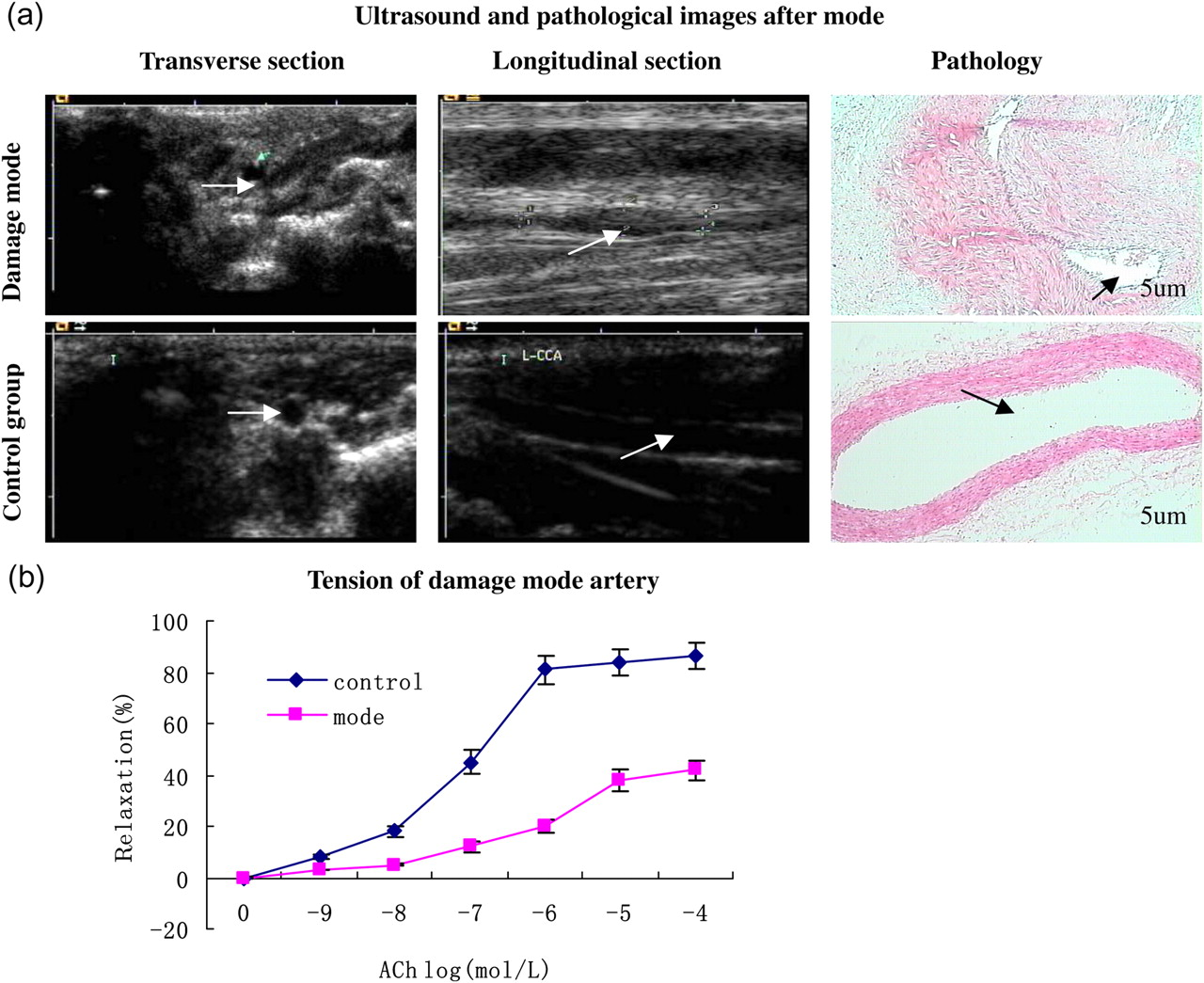
(a) Images of rabbit common carotid artery of damage mode obtained by ultrasound and pathological examination. The white arrows indicate the lumen of the artery. A significant difference was found in the arterial lumina for the experimental groups. There were more plaques and proliferation than in the control. This demonstrates that there are beneficial results when trying to correct the common carotid artery damage-mode group. (b) Arterial tension of the control and mode group. The control-group tension was significantly higher than the mode of the tension group. This shows that the mode group arterial function was not as strong as that in the control group. These data are representative of three independent experiments. n = 3. **P < 0.01, *P < 0.05 (A color version of this figure is available in the online journal)
Blood flow velocity and arterial diameter in control group and mode group
The blood flow velocity in the control group was lower than that of the damage-mode group, but the control group of arterial diameter was bigger than that of the damage-mode group. These data are representative of three independent experiments. n = 3. *P < 0.05 vs control group; **P < 0.001 vs control group
Detection of various methods transfecting TFPI-2 into the arterial endothelium
To study the effect of TFPI-2 transferred by SonoVue on thrombosis and arterial re-stenosis, we evaluated different experiment groups of arterial ultrasound images, histological pathological images, diameter, tension, blood flow velocity and TFPI-2 expression by Western blot. In parallel, TFPI-2 transfection mediated by adenovirus was also examined. The arterial lumen of the two control groups (first group and second group) did not show plaques or re-stenosis. There was minimal evidence of plaques and arterial re-stenosis detected in the SonoVue and adenovirus groups, but significantly less than in the positive control (Figure 5a). With a peak ratio of TFPI-2 to β-actin, the first, second, positive, SonoVue and adenovirus group values were 0.31 ± 0.06, 0.33 ± 0.07, 0.38 ± 0.07, 1.65 ± 0.11 and 1.1 ± 0.09, respectively (Figure 5b). TFPI-2 protein expression in the SonoVue and adenovirus groups was significantly higher than that of the other groups. Arterial tensions of all experimental groups were changed by various doses of Ach stimulation (Figure 5c). The arterial tension in the control group was higher than in other groups. It was obviously known from Figure 5c that the arterial tension in the positive, SonoVue and adenovirus groups was lower than that in the control group. However, in the SonoVue and adenovirus groups, arterial tension was higher than the positive. The arterial diameter value in the SonoVue and adenovirus groups was larger than the positive one, but smaller than the control group. Compared with the arterial diameter, the arterial blood flow velocity in those groups was reverse to the control group (Table 4). From these results, we concluded that, using the SonoVue method, the TFPI-2 gene was transferred into the arterial intima and suppressed the thrombosis and arterial re-stenosis.

(a) Analyses of TFPI-2 inhibition on thrombosis and re-stenosis of arteries in different experimental groups. Rabbit common carotid arteries of each group were detected by ultrasound and imaged at the cross-section and longitudinal section of the artery. Once imaging was complete, the artery was removed and pathological examination was done. The white arrows indicate the lumina of arteries. No significant amounts of plaque or signs of re-stenosis were observed in the negative control group. The positive control groups had a significant amount of plaque and re-stenosis within the artery. The plaques and arterial re-stenosis in the experimental groups were less than those of the positive control group, signifying the ability of TFPI-2 to inhibit arterial proliferation. (b) TFPI-2 protein expression in the SonoVue and adenovirus groups was greater than in the other groups. (c) The two control groups of tension were much higher than that of other groups. Arterial tension in the SonoVue and adenovirus group was higher than in the positive group; and the arterial tension in the SonoVue group was higher than the adenovirus group. These data are representative of three independent experiments. n = 3. **P < 0.01, *P < 0.05 (A color version of this figure is available in the online journal)
Blood flow velocity and arterial diameter in all experimental groups
The blood flow velocity in the control groups was smaller than that of other groups, but the control group of arterial diameter larger to other. The SonoVue and adenovirus groups of blood flow velocity was lower than that of the positive group, and yet their arterial diameter was long. These data are representative of three independent experiments. n = 3. *P < 0.05 vs First and Second groups; **P < 0.001 vs First and Second groups
Discussion
In the present study, we proved that TFPI-2 was expressed in vitro using the SonoVue technique. In vivo, it proved to be an effective, safe and specific method for preventing thrombosis and suppressing new intima hyperplasia. Several recent studies 18,19 have reported that TFPI-2 has a major role in the inhibition of thrombosis and arterial hyperplasia. SonoVue is a type of microbubble ultrasound contrast agent, the size of which is between 1 and 10 μm and their membrane is a bipolar molecule. It can increase image definition in ultrasonic diagnostic imaging, and has been used for the delivery of drugs. 20 Ultrasound, an ideal technique in diagnostic imaging, has been used in the treatment of many diseases. The permeability of biological membranes can be altered by ultrasonic waves; hence, some researchers have attempted to deliver drugs into cells using this method. 21 We decided to establish a new approach for transferring TFPI-2 with SonoVue and ultrasonic waves into the intima of arteries to suppress thrombosis and arterial re-stenosis.
Optimizing the experimental conditions of the assay is required before experiments could be carried out and analyzed. We initially examined the cytotoxicity of SonoVue and ultrasound to HUVECs (data not shown). SonoVue and ultrasound did not cause significant harm to HUVECs, which was in accordance with other studies. 10 Plasmids were not broken down by ultrasound waves (data not shown). Originally, we did not know whether the SonoVue could adhere to plasmids and how many plasmids might be adhered to. Through preparative experiments, the SonoVue could adhere to plasmids and the maximal adherence ratio of SonoVue was about 90.1%. The adherence effect reason of SonoVue and plasmids could be the static gravitation of DNA and bipolar molecule. These results indicated that the experimental basis of the study was robust.
TFPI-2 transfection efficiency using different methods was analyzed. Whether the TFPI-2 gene could be transfected into HUVECs or the arterial endothelium was critical. By comparing the two transfection methods (SonoVue and adenovirus), the transfection efficiency of SonoVue and adenovirus groups was found to be higher than the liposome and control methods in vitro, and there was no significant difference between the SonoVue and adenovirus groups in vitro. The in vivo transfection efficiency of SonoVue was higher than that of adenovirus. The most reasonable explanation is that the ultrasound contrast agent enhanced vascular permeability. 22 Conversely, the adenovirus method was detrimental to arterial tissue. Data supporting the theory that SonoVue and ultrasound waves transferred TFPI-2 were convincing (Figures 1 –3a and b). Preceding the experiments, rabbit common carotid artery of damage mode was set as the positive control. Through the analysis of different transfection methods, we found that the SonoVue transfection method could be a target-specific, safe, and effective procedure for delivering a gene into the arterial endothelium. However, thrombosis and arterial re-stenosis could not be completely inhibited. We postulated that other contributing factors may affect the artery. In some cases where inflammation was not controlled at the wounded site of artery, inhibition of TFPI-2 effect was found to result in recurrent damages of the artery. This notion requires further exploration.
In conclusion, these results suggest that transferring the TFPI-2 gene directly into the artery in vivo by SonoVue is feasible and has great potential. The adenovirus is widely used as a transfection vector in gene therapy, but has two major obstacles: (i) the intrinsic potential insecurity of the adenovirus vector, and (ii) the extensive nonspecificity of the adenovirus on host cells which leads to non-targeted gene transfection. Moreover, due to the special anatomical location and rapid blood flow, traditional gene therapy strategies are hard to apply in atherosclerosis.
Conclusion
The present study showed that the SonoVue transfection technique is a more targeted, safe, convenient and efficient method for transfecting genes into arterial walls than that of adenvorius. The ability to regulate the amount of gene expression could become a promising step towards gene therapy.
Footnotes
ACKNOWLEDGEMENTS
This work was supported by grants from the National Natural Science Foundation of China (grant number 30570554 and 30770446), Health Department Fund Project in Hubei Province (grant number JX3B01), Science and Technology Department Fund Project in Hubei Province (grant number 200950431178) and University Special Basic Research Fund Project in China. We thank Associate Professor Yilong Zhang for technical assistance, and Dr Ping Yuan for providing the adenovirus.