
Abstract
Genetic factors are important in the pathogenesis of diabetic retinopathy (DR); there is a clear association of increased expression of vascular endothelial growth factor (VEGF) with DR as well as numerous VEGF polymorphisms that are linked to increased VEGF levels and DR. In this study, the relationships between the VEGF promoter polymorphism −634C/G, plasma VEGF levels and DR were examined in the Han Chinese. Ninety-six healthy subjects and 285 subjects with type 2 diabetes were enrolled in this study. The diabetic subjects were divided into three groups depending on the degree of DR as determined by fundus photography and fluorescent angiography. Along with standard clinical characteristics, the −634C/G polymorphism was examined using TaqMan allelic discrimination, and plasma VEGF levels were analyzed by enzyme-linked immunosorbent assay. The distribution of the polymorphism differed significantly between patients with and without retinopathy; this was most pronounced between the no DR and proliferative DR groups. Significantly greater plasma VEGF levels were present in those with the −634CC genotype, and only the proliferative DR group had elevated plasma VEGF levels. Logistic regression revealed that the −634C/G polymorphism is strongly associated with DR. This study suggests that diabetic Han Chinese carrying the −634CC VEGF promoter polymorphism have a genetic risk of DR, and this polymorphism may be a major factor influencing plasma VEGF levels. Therefore, this polymorphism may be used as a biomarker at the onset of diabetes in the Han Chinese to predict the risk of DR, allowing for clinicians to treat these patients more aggressively.
Keywords
Introduction
Diabetic retinopathy (DR) is the most common microvascular complication of diabetes and a leading cause of blindness in the world, affecting approximately three-fourths of diabetic patients 15 years after the onset of the disease. 1 There is already strong evidence that longer duration of diabetes, poorer control of blood glucose and elevated blood pressure are the major factors responsible for the onset and progression of DR. 2–4 However, DR occurs even with optimal glucose and blood pressure control. 2,5,6 Consequently, the pathogenesis of DR is thought to be determined by environmental and genetic factors. Ethnic differences in the prevalence of DR may provide insights into the relative importance of genetic or environmental risk factors; 7,8 therefore, we examined type 2 diabetes mellitus (T2DM) in the Han Chinese, who are a single large ethnic group that has not been studied in respect to DR.
In DR, vascular endothelial growth factor (VEGF) plays a role in the neovascularization of proliferative retinopathy and in the breakdown of the blood–retinal barrier that is characterized by hyperpermeability of retinal vessels. 9,10 Markedly elevated serum and vitreous levels of VEGF have also been reported in eyes of patients with proliferative DR. 11 The promoter region of VEGF has several polymorphisms, 12 some of which have been examined in the context of DR. However, the data obtained in these reports are not consistent, especially regarding the involvement of the −634C/G polymorphism with retinopathy. 13–18 In the Japanese, the −634C/G polymorphism has been reported to be both associated 13 and not associated 15 with DR. Similarly, studies in ethnically more varied societies produced similar contradictory reports; 16–19 however, the majority of reports indicate that polymorphisms within the VEGF promoter are associated with DR. Consequently, it has been suggested that the VEGF −634C/G polymorphism might serve as a predictive factor for the development of DR 19 ; thus, this polymorphism is the focus of our study.
Importantly, this study represents the first examination of a VEGF polymorphism in type 2 diabetic Han Chinese. The Han are the largest ethnic group within China, 20,21 numbering approximately one billion, which also makes this group the largest ethnic group in the world. Since genetic polymorphisms often vary between ethnic groups, all of the major ethnic groups should be examined to clarify the association between VEGF polymorphisms with DR. In addition, since VEGF polymorphisms in DR have not been examined in the Han Chinese, which unlike many previous studies is a single ethnic group, we evaluated the association of the −634C/G VEGF promoter polymorphism with DR in type 2 diabetic Han Chinese. In addition, we examined the relationship among standard clinical characteristics, the VEGF −634C/G polymorphism, plasma levels of VEGF and DR. The data indicate that the VEGF −634C/G polymorphism is associated with DR, and thus can be used as an early biomarker of retinopathy in the Han Chinese.
Materials and methods
Subjects
A total of 285 subjects with type 2 diabetes and 96 healthy control subjects from rural and urban areas within Yunnan Province were recruited from individuals admitted to the Yunnan Province 2nd Hospital (Kunming, China). In China all citizens have an identity card that indicates their ethnicity; all subjects were ethnic Han Chinese. Diagnosis and classification of diabetes was based on clinical features, laboratory data and the guidelines of the Expert Committee Report of the American Diabetes Association. We specifically excluded patients with a history of myocardial infarction (MI), or presenting MI. Each patient was examined via 12-lead electrocardiogram; the exclusion criteria of MI in our study were made according to the MI diagnosis criteria by the World Health Organization. 22 Body mass index (BMI) was calculated as weight/height 2 (kg/m2) and waist–hip ratio (WHR) was calculated. Blood pressure was measured by mercury sphygmomanometer. Fasting glycated hemoglobin (HbA1c), cholesterol (TC) and triglyceride (TG) levels were measured using conventional clinical methods. The normal control (NC) group consisted of unrelated healthy individuals with no family history of type 2 diabetes or other conditions and no abnormal laboratory findings. Informed consent was obtained from each individual; all procedures were conducted in accordance with the principles of the Declaration of Helsinki.
Ophthalmological evaluation
All patients underwent a complete ophthalmological examination, including corrected slit-lamp microscopic examination (with and without preset lens), funduscopic examination and fundus photography. They were classified as non-retinopathy (non-DR), non-proliferative DR (non-PDR) and proliferative DR (PDR). The classification used is as described before. 13 The DR group includes both the non-PDR and PDR groups. If diagnosis of DR was found by fundus photography, it was confirmed by fluorescent angiography.
Genotyping of VEGF gene polymorphism
The VEGF gene promoter polymorphism −634C/G (rs2010963) was detected by TaqMan allelic discrimination (Applied Biosystems, Foster City, CA, USA). The genotyping was confirmed by sending the PCR products to Shanghai Sangon Biological Engineering Technology & Services Co, Ltd (Shanghai, China) for sequencing.
Measurement of serum VEGF concentrations
Venous blood samples were taken from 96 healthy subjects and 285 type 2 diabetic patients fasting over night. Plasma was separated by centrifuge and then stored at −20°C until analysis. VEGF serum levels were measured using an enzyme-linked immunosorbent assay (human VEGF Quantikine; R&D Systems, Minneapolis, MN, USA) according to the manufacturer's instructions.
Statistical analysis
Statistical analyses were performed using SPSS 10.0 (SPSS Inc, Chicago, IL, USA) and Prism 5 (GraphPad Software, Inc, La Jolla, CA, USA). Distribution of genotypes and alleles was compared by chi-square test or Fisher's exact test depending on sample size. Clinical data were compared by one-way analysis of variance (ANOVA) and multivariate analysis of variance (MANOVA) with Tukey–Kramer's post hoc test, and categorical clinical data were compared by Fisher's exact test. Logistic regression was used to calculate the odds ratios (ORs) and 95% confidence intervals (CIs) for incident retinopathy in diabetic patients. Statistical significance was defined as P < 0.05.
Results
Subjects and ophthalmology
Based on ophthalmological evaluation, individuals with T2DM were divided into three groups: 109 patients did not present any signs of retinopathy (non-DR group), 110 patients presented with non-proliferative DR (non-PDR group) and 66 patients presented with proliferative DR (PDR group) (Table 1). We examined clinical characteristics in each category of DR. With one-way ANOVA the comparison of groups enrolled in the present study revealed a significant difference in age (F = 7.767, P = 0.01), systolic blood pressure (SBP) (F = 4.249, P = 0.015) and diastolic blood pressure (DBP) (F = 5.202, P = 0.010) but no statistically significant differences in the duration of diabetes, BMI, WHR, fasting blood glucose (FBG), HbA1c, TC and TG. Post hoc analyses indicated that the age of the non-PDR group was greater than the non-DR or PDR groups (P < 0.05), and SBP as well as DBP were decreased in the non-DR group compared with the non-PDR and PDR groups (P < 0.05).
Clinical characteristics of type 2 diabetic patients divided into three groups based on the severity of their diabetic retinopathy
DR, diabetic retinopathy; PDR, proliferative diabetic retinopathy; BMI, body mass index; WHR, waist–hip ratio; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, fasting blood glucose; HbA1c, glycated haemoglobin; TC, cholesterol; TG, triglyceride; ANOVA, analysis of variance
Data are presented as means ± SE. Statistical differences were examined via one-way ANOVA with Tukey–Kramer's post hoc tests and for the duration a logarithmic transformation was conducted prior to the ANOVA. Data were determined to be significant when P < 0.05; this is denoted by Greek letters; values with different Greek letters are significantly different, and no notation indicates that there are no significant differences between the groups
Association of VEGF polymorphism with DR
Each subject's genotype was analyzed by TaqMan probe allelic discrimination, and the products were confirmed by DNA sequencing (Figure 1). The frequency of the −634C/G polymorphism (Table 2) did not deviate from the Hardy–Weinberg equilibrium for any of the groups. However, there were significant differences in the frequency of the polymorphism at −634 of the VEGF promoter between non-DR and DR groups (P = 0.0253), and non-DR and PDR groups (P = 0.0265) (Table 3). Although no significant differences were observed between the other groups, there is a trend for the non-DR group to have fewer individuals with the VEGF −634CC genotype compared with the NC and non-PDR groups, suggesting that the VEGF −634CC genotype may be detrimental in T2DM. Additionally, there is no difference in the distribution of alleles between the NC and T2DM groups, indicating that the −634C/G polymorphism is not associated with diabetes. Taken together these data indicate that 11.5% of the Han Chinese carry the −634CC genotype, and that in diabetes this genotype may be detrimental.

Representative sequence of the −634C/G vascular endothelial growth factor polymorphism. The three possible genotypes –634GG (top), CC (middle) and CG (bottom). The polymorphism is easily identifiable by both the TaqMan probes and sequencing
Genotype and allele distribution of VEGF polymorphisms
VEGF, vascular endothelial growth factor; NC, normal control; T2DM, type 2 diabetes mellitus; DR, diabetic retinopathy; PDR, proliferative diabetic retinopathy
Data are presented as numbers and in parentheses percentages. The 634C/G polymorphism is in complete Hardy–Weinberg equilibrium in all subjects. The statistical analysis is shown in Table 3
Comparison of the −634C/G polymorphism across all groups of patients
NC, normal control; T2DM, type 2 diabetes mellitus; DR, diabetic retinopathy; PDR, proliferative diabetic retinopathy
The raw data are presented in Table 2; P values are shown from chi-square test. An asterisk (*) indicates the traditional acceptance of significance (P < 0.05), and an (x) indicates that no test was run either because it is a duplicate or one component is a subgroup of the other component in the test
To determine whether the −634CC VEGF promoter genotype alone is detrimental, two-tailed Fisher's exact test was used to determine whether the frequency of the CC genotype is associated with the severity of DR. As shown in Table 2 the CC frequency is similar in the NC, T2DM and the T2DM subgroup DR; thus, it is not surprising that there is no difference in the frequency of the CC versus CG and GG genotypes in these groups. However, the non-DR group has significantly fewer individuals with the CC genotype compared with all other groups (Table 4). Thus, the data indicate that −634 VEGF CC genotype is associated with DR; moreover, the lack of difference between the frequencies of this polymorphism in the normal and T2DM groups indicates that this polymorphism likely synergizes with the diabetic condition to cause retinopathy.
Examination of the numbers of individuals in a group with the CC genotype in relation to the GC and GG genotype
NC, normal control; DR, diabetic retinopathy; PDR, proliferative diabetic retinopathy
Fisher's exact test (CC versus GC + GG), P values are shown. An asterisk (*) indicates the traditional acceptance of significance (P < 0.05)
Association of VEGF polymorphism with plasma levels of VEGF
To assess the functional relevance of the −634C/G VEGF promoter polymorphism on plasma VEGF levels, 96 NC and 285 T2DM patients' plasma VEGF concentrations were examined. As shown in Figure 2, fasting plasma VEGF levels were significantly greater in subjects with the −634CC genotype than either those with the CG or GG genotypes. Although there is a tendency for patients with the GC genotype to have increased plasma VEGF concentrations compared with the GG genotype, this increase is not statistically significant (P = 0.75). Therefore, the C allele appears to increase plasma VEGF concentrations. Additionally, plasma VEGF levels in the diabetic patients were grouped by the clinical presentation of retinopathy; individuals within the PDR group have greater plasma VEGF levels than either the non-DR or non-PDR group (P < 0.05) (Figure 3), and there is no difference between the non-DR and non-PDR groups. Because DR is associated with the duration of diabetes 21,23 and our subjects represent a wide variation in their duration of diabetes (Table 1), we conducted two tests to examine the role of duration of diabetes in our previous analyses. We examined the effect of duration of diabetes (Supplementary Table 1) on the association of the −634C/G polymorphism and presentation of retinopathy via chi-square analysis. We found little to no differences between the three duration groups (0–10, 11–20, and 21+ years) and distribution of the −634C/G polymorphism within each group. To further determine the role of duration of diabetes on plasma VEGF levels, we utilized a MANOVA with the −634C/G polymorphism, duration of diabetes and presentation of retinopathy as the factors. Only genotype (P = 0.000032) and the degree of retinopathy (P = 0.000001) were found to have significant effects on the plasma VEGF levels (Figures 2 and 3, respectively); duration of diabetes was not found to be a significant factor. Moreover, when examining the interaction between factors, no significant differences were observed when duration was included as a factor. Thus, the data indicate that increased plasma VEGF levels are found in patients carrying the −634CC VFGF promoter genotype and those patients with the most aggressive form of retinopathy (PDR) have the greatest plasma VEGF levels, both of which are independent of the duration of diabetes.
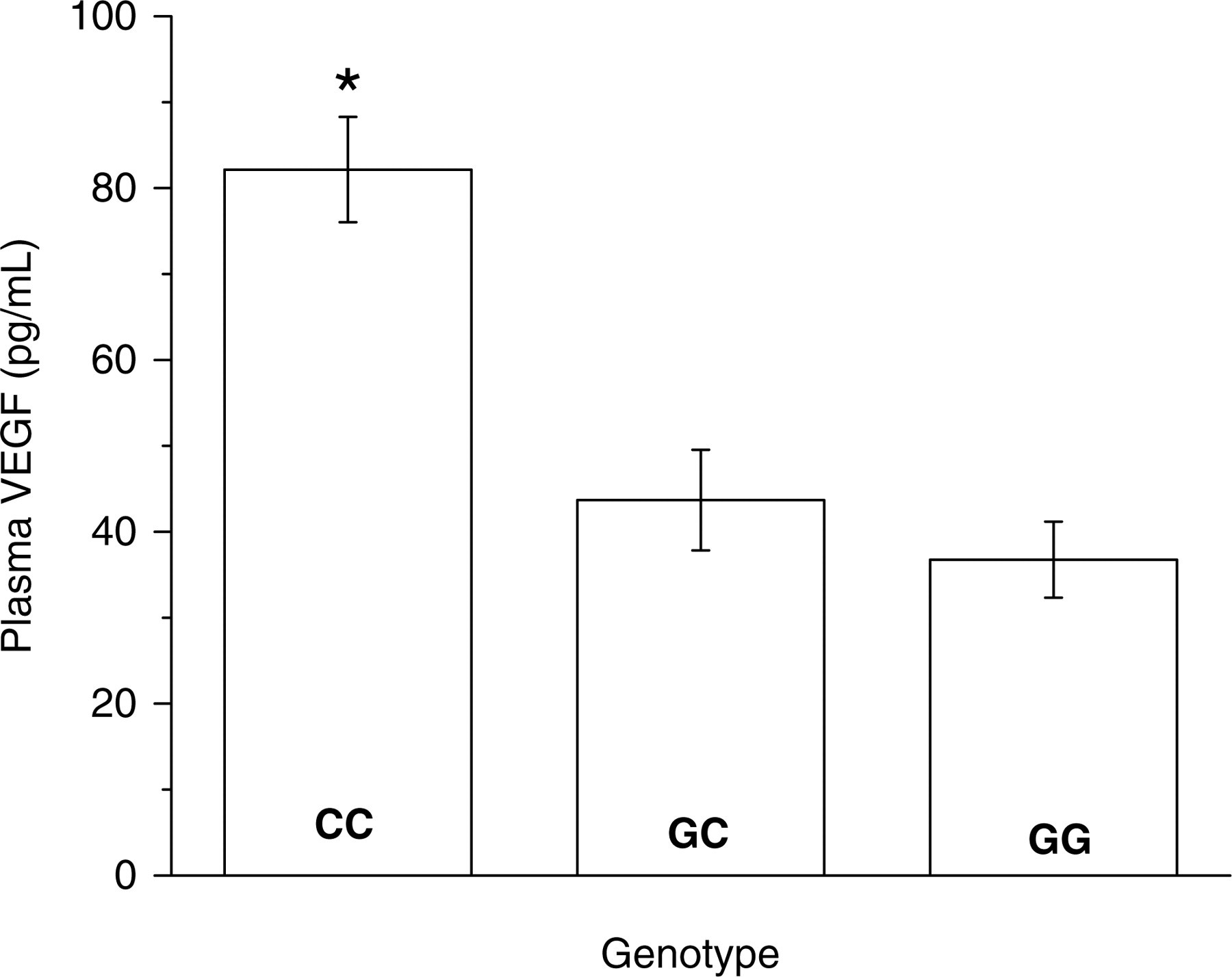
Comparison of plasma VEGF levels in Han Chinese carrying the −634CC, GC and GG VEGF promoter variants. The histogram depicts plasma VEGF levels (means ± SE) in subjects with CC (n = 47), GC (n = 170) and GG (n = 123) genotypes at –634 of the VEGF promoter. Bar with an asterisk (*) is significantly different (P < 0.01) from the other bars as determined by one-way ANOVA with Tukey–Kramer's post hoc test. VEGF, vascular endothelial growth factor; ANOVA, analysis of variance

Comparison of plasma VEGF levels in Han Chinese diabetic patients classified via the degree of retinopathy. The histogram depicts plasma VEGF levels (means ± SE) in subjects within the three subcategories of type 2 diabetes: non-DR (n = 109), non-PDR (n = 110) and PDR (n = 66). Bar with an asterisk (*) is significantly different (P < 0.01) from the other bars as determined by one-way ANOVA with Tukey–Kramer's post hoc test. VEGF, vascular endothelial growth factor; ANOVA, analysis of variance; DR, diabetic retinopathy; PDR, proliferative diabetic retinopathy
Association of VEGF polymorphism with clinical characteristics
Since there are significant differences in age, SBP and DBP in the population examined, based on the clinical presentation of retinopathy, the clinical characteristics of the population were also grouped based on the patient's genotype. When arranged by genotype, age, duration of T2DM, SBP, DBP, BMI, WHR, FBG, HbA1c, TC and TG did not vary significantly between the genotypes (Table 5). Therefore, the −634C/G VEGF promoter polymorphism is not related to any of the measured clinical characteristics. To further assess the relationship of the −634C/G polymorphism with DR, multivariate logistic regression analysis of the polymorphism and clinical features was performed (Table 6). Coverage estimates are presented with a 95% CI; statistical significance of the effect of determinants on coverage rates was tested for each factor independently by univariate and multiple logistic regressions. Final models were selected via backward selection (the P value for elimination was >0.1). DBP, plasma VEGF and CC genotype were the factors included in this analysis. It was revealed that the −634C/G VEGF promoter genotype denotes a significantly increased risk of DR (OR = 2.6, P < 0.001), and that the polymorphism is the most predictive −634C/G polymorphism for DR. Additional predictors of DR include plasma VEGF levels and DBP. Therefore, in the Han Chinese with T2DM the −634C/G VEGF polymorphism is associated with DR, and can be used as a predictive biomarker for DR in the clinic.
Clinical and biochemical characteristics of study group classified according to VEGF genotype
VEGF, vascular endothelial growth factor; BMI, body mass index; WHR, waist–hip ratio; SBP, systolic blood pressure; DBP, diastolic blood pressure; FBG, fasting blood glucose; HbA1c, glycated haemoglobin; TC, cholesterol; TG, triglyceride; ANOVA, analysis of variance
Data are presented as means ± SE. Statistical differences were examined via one-way ANOVA with Tukey–Kramer's post hoc tests and determined to be significant when P < 0.05; there is no significant difference among the genotypes
Odds ratios adjusted by logistic regression analysis for the association with DR among type 2 diabetes patients
DR, diabetic retinopathy; VEGF, vascular endothelial growth factor; BMI, body mass index; SBP, systolic blood pressure; DBP, diastolic blood pressure; OR, odds ratio; CI, confidence interval
OR is presented with its 95% CI, and the P value is given. P < 0.05 is considered significant and is denoted by an asterisk. An asterisk (*) indicates the traditional acceptance of significance (P < 0.05)
Discussion
VEGF is involved with retinal vascularization, as it participates in the formation of new vessels that appear after retinal ischemia 24,25 and several clinical trials are currently investigating the efficacy of anti-VEGF agents in the treatment of DR. 26,27 In this study, only the −634C/G polymorphism in the 5′-untranslated region of the VEGF gene was examined, because this polymorphism has been found to be common in multiple populations with DR. 13–19 In the retina, VEGF is produced in the pigmented epithelium, the neurosensory retina, the pericytes and the vascular smooth muscle layer. 28,29 Plasma VEGF levels are influenced by multiple factors, and are not equal to the levels of vitreous and aqueous fluids within the eyes; however, plasma VEGF is recognized as an indirect measure of these fluids' VEGF levels. 30,31 In different populations including Caucasian, Japanese and Indian, the association of VEGF −634C/G polymorphism and DR is contradictive. 13–19 These differences could possibly be due to differences in the genetic background or environment of each population under examination. Therefore, we focused on a single ethnic group, the Han Chinese, in a defined geographical area, Yunnan Province.
In our patient population, Han Chinese presenting PDR have greater plasma VEGF levels than patients presenting non-DR or non-PDR (Figure 3). VEGF plasma levels may be one of the predictors for DR in type 2 diabetic patients. 32 Our study indicates that Han Chinese carrying the VEGF −634CC genotype have greater plasma VEGF levels, and the VEGF gene −634C/G polymorphism is a risk factor for DR in the Han Chinese, which is similar to what has been reported in the Japanese. 13 In our study the −634C/G polymorphism is not only related to DR, but is also associated with a severe stage of retinopathy (PDR), that is with neovascularization. This is reasonable, because VEGF-induced vascular permeability as well as angiogenesis should be an important factor in development of PDR.
The VEGF −634C/G polymorphism is also a potential marker for MI in type 2 diabetic Caucasians. 33,34 This is likely due to the increased levels of VEGF due to this polymorphism (see below for further discussion); increased VEGF levels are associated with more sever MI and poor prognoses. 35 This has yet to be tested in the Han Chinese; however, it is likely that the increased plasma VEGF observed in the PDR group would predict further diabetic pathologies. This also explains the low sample size of this group as patients with cardiovascular pathologies were excluded from the study. Further studies are required to determine if the VEGF −634C/G polymorphism leads to additional vascular pathologies in the Han Chinese.
Diabetes duration has been shown to be an independent risk factor for retinopathy in many studies. 21,23 The patients in this study represent a wide range of duration of diabetes and age; yet there are no differences between distribution of the −634C/G polymorphism within each duration of diabetes group (0–10, 11–20 and 21+ years) (Supplementary Table 1). Moreover, duration of diabetes is not associated with plasma VEGF levels. Therefore, in the Han Chinese it appears that the duration of diabetes is not associated with DR. However, further studies should be conducted to examine other polymorphisms, and retrospective and prospective studies should be conducted to determine if VEGF polymorphisms, especially the −634CC, accelerate the progression of DR in the Han Chinese as can be hypothesized based on this study.
Our findings suggest that the VEGF −634CC genotype increases the risk of DR development in Han Chinese with type 2 diabetes. Plasma VEGF concentration is enhanced in Han Chinese with the VEGF −634CC genotype, and is associated with DR. The most likely mechanism is that the −634CC genotype results in increased activity of the VEGF promoter. The 5′ UTR of VEGF has two internal ribosomal entry sites (IRES) that control translation of VEGF mRNA, and the second IRES is affected by the −634C/G polymorphism. 36 The VEGF gene expression is increased by the −634C allele, but not by the −634G allele. In vitro studies indicate that this increase is due to alternations of the second IRES activity; −634GG genotype has significantly lower activity compared with −634CC genotype, 37 which likely explains the higher plasma VEGF levels found in Han Chinese with the VEGF −634 CC genotype (Figure 2). However, there is also the possibility that there are other confounding factors besides the −634C/G polymorphism in our analysis, such as environmental and genetical factors (i.e. hypoxia, hyperglycemia, oxidative stress, ischemia and other VEGF gene polymorphisms) that influence plasma VEGF levels. 38 Further studies will have to be conducted to determine whether the −634GG genotype is sufficient to induce DR.
Not only is there an increase in the prevalence of type 2 diabetes in China, DR is also on the rise. 39 Thus, it is necessary to investigate genetic factors in the pathogenesis of DR in the Han Chinese because the Han Chinese represent the majority of the Chinese. 20,40 The present study is the first time that a relationship among VEGF gene −634C/G polymorphism, plasma levels of VEGF and DR in type 2 diabetic patients has been examined specially in the Han Chinese. The data indicate that the VEGF −634CC genotype is associated with increased plasma levels of VEGF in the Han Chinese and DR; moreover, type 2 diabetic patients who do not present with retinopathy have a reduced frequency of the −634CC genotype compared with the normal population and patients with DR. Consequently, the −634CC genotype is a negative factor contributing to increased VEGF levels that synergize with the diabetic condition resulting in increased retinopathy.
Therefore, this gene polymorphism can be used as a clinical marker in diabetic Han Chinese prior to the observance of retinopathy. A result of a −634CC genotype would indicate that the patient should be monitored more frequently and may also suggest the use of an anti-VEGF therapy such as ranibizumab or bevacizumab. 41 Such an approach will allow for personalized medicine. However, a larger multicenter study is needed to test the hypotheses that VEGF gene polymorphisms are causative of the observed increased VEGF levels and subsequently DR in the Han Chinese before such preventive therapy is wanted. The data presented here can be used as a predictive clinical marker of future DR, which can be used to alter the treatment regimen of the patient.
Footnotes
Acknowledgements
This project was supported by grants from the National Natural Science Foundation of China (No. 30960148), the Science Foundation of Education Department of Yunnan Province (No. 2007Z40625) and a grant from the Red Cross hospital of Yunnan Province (No. 2008yk009). The authors would like to thank the staff of the Department of Endocrinology and Metabolism, Department of Ophthalmology and Department of Healthy Check-up Center in Yunnan Province 2nd Hospital China who conducted the clinical examinations. The authors would also like to thank Dr L Feng, M Qiong and F Zhengdong for aiding in collection of the clinical data and logistic regression analysis, as well as acknowledge the China Scholarship Council for its support of YY's travels to the United States of America. Additionally, we would also like to acknowledge Dr James R Sowers for his support of YY while training in the USA.