
Abstract
Preclinical results with various gene therapy strategies indicate significant potential for new cancer treatments. However, many therapeutics fail at clinical trial, often due to differences in tissue physiology between animal models and humans, and tumor phenotype variation. Clinical data relevant to treatment strategies may be generated prior to clinical trial through experimentation using intact patient tissue ex vivo. We developed a novel tumor slice model culture system that is universally applicable to gene delivery methods, using a realtime luminescence detection method to assess gene delivery. Methods investigated include viruses (adenovirus [Ad] and adeno-associated virus), lipofection, ultrasound (US), electroporation and naked DNA. Viability and tumor populations within the slices were well maintained for seven days, and gene delivery was qualitatively and quantitatively examinable for all vectors. Ad was the most efficient gene delivery vector with transduction efficiency >50%. US proved the optimal non-viral gene delivery method in human tumor slices. The nature of the ex vivo culture system permitted examination of specific elements. Parameters shown to diminish Ad gene delivery included blood, regions of low viability and secondary disease. US gene delivery was significantly reduced by blood and skin, while tissue hyperthermia improved gene delivery. US achieved improved efficacy for secondary disease. The ex vivo model was also suitable for examination of tissue-specific effects on vector expression, with Ad expression mediated by the CXCR4 promoter shown to provide a tumor selective advantage over the ubiquitously active cytomegalovirus promoter. In conclusion, this is the first study incorporating patient tissue models in comparing gene delivery from various vectors, providing knowledge on cell-type specificity and examining the crucial biological factors determining successful gene delivery. The results highlight the importance of in-depth preclinical assessment of novel therapeutics and may serve as a platform for further testing of current, novel gene delivery approaches.
Introduction
Breast cancer is estimated to account for nearly 27% of predicted new cancer cases in the USA and Europe this year. 1,2 Despite early detection methods and advanced conventional treatments, loco-regional recurrence rates can be as high as 13%. 3 Nearly half of these patients will develop treatment-resistant loco-regional disease, which is an independent prognostic factor associated with poor outcome. 4 These figures clearly indicate the urgent need for novel therapies in the treatment of this disease and gene therapy is believed to offer exciting therapeutic approaches, 5 and thus may prove suitable in altering the course of recurrent loco-regional disease.
Various gene therapy strategies may be applicable for the targeted treatment of loco-regional disease. Clinical application, however, depends on the ability to deliver sufficient genes to the target site. Six methods of gene delivery were examined in this study. While the use of other potentially more efficient and less immunogenic vectors, such as other viral vectors, nanoparticles, bacteria 6–9 and more, is increasing, there are currently numerous ongoing human clinical trials utilizing the methods described in this paper. The adenovirus (Ad) vector, due to its exceptional gene delivery capability, has been the most widely used in preclinical and clinical trials. 10 The concurrent success of non-viral gene delivery systems, including electroporation (EP) and ultrasound (US), has also encouraged significant work in this field. 11–13 Recent failure of promising gene therapy strategies in the clinical setting has highlighted the importance of testing strategies on the most stringent model available prior to entering clinical trials. 14–16 The factors that are thought to play a major role in treatment failure are the unpredictable variation in tissue physiology between rodent and man, tumor heterogeneity and complex tumor phenotypes. This research quagmire has led to the demand for alternative models and has prompted the emergence of ex vivo model systems utilizing intact human tissue. The tissue slice model system was first introduced by Krumdieck et al. 17 several decades ago; however, its relevance and potential in cancer research has only been realized of late. It involves the use of fresh human tumor tissue, cut into thin slices and maintained ex vivo, and represents a more clinically relevant primary model as it allows strategies to be tested on intact tissue. Several reports have utilized the tissue slice model of human tumors to study Ad-mediated gene delivery; 18–21 however, little is known about the effects of other gene delivery systems on human tumors and none of the current models offer the opportunity to investigate other gene delivery methods. Furthermore, previous reports on ex vivo models used analysis techniques requiring sacrifice of the tissue for quantification of gene expression. We introduce a novel ex vivo system with the capability of examining all delivery methods and offering realtime analysis of gene delivery. The universal application is achieved by utilizing a slice thickness that does not limit nutrient and oxygen diffusion throughout the slice and allows for the physical delivery of genes by direct injection or the use of devices for EP and sonoporation. Furthermore, a thicker slice, which maintains all cellular components and diffusion gradients, would more closely represent the true intratumoral conditions of solid tumors.
For measurements of ex vivo gene expression, we introduce a novel bioluminescence imaging technique based on the expression of luciferase, the light-emitting enzyme of the firefly Photinus pyralis. 22 This non-toxic detection system enables the sequential quantification of gene expression without sacrifice of tissue, allowing for the measurement of duration of expression and thereby enabling assessment of vectors requiring longer incubation periods for maximum expression such as adeno-associated virus (AAV). 23 For the investigation of vector efficacy, toxicity and target cell specificity, we have optimized a dissociation technique, which provides representative cells from the entire slice for the accurate assessment of viability using automated cell counting and for identification of cell types by flow cytometric analysis. Using this model system we evaluate the efficacy of various gene delivery methods and the factors that limit or enhance gene expression in patient tumor samples. We also investigate the potential of tumor-specific promoters to enhance tumor selectivity over normal tissue. This model will broaden our understanding of the biological factors that promote and hinder successful gene delivery to tumors and provide valuable insight for identifying novel gene delivery systems for the treatment of loco-regional breast cancer. This will permit further assessment of the clinical relevance of new treatment strategies prior to entering clinical trial.
Materials and methods
Human tissue samples
This study was approved by the Clinical Research Ethics Committee of the Cork Teaching Hospitals and informed consent was obtained from the patients the day before surgery. Breast tumor samples were obtained from 80 patients undergoing wide local excision or mastectomy because of breast cancer, their age ranging between 35 and 75 years. The tissue was obtained from tumors greater than 2 cm in diameter as surgical waste from patients at the South Infirmary Victoria Hospital and Mercy University Hospital immediately after surgical resection. Liver tissue was obtained from three patients undergoing partial hepatectomy for metastatic liver disease. Colon tissue was obtained from three patients undergoing bowel resection for malignancy.
Tissue slice culture
Fresh tumor material upon collection was placed in collection media (Dulbecco's modified Eagle's medium [DMEM] supplemented with penicillin [200 IU/L], streptomycin [200 μg/L] and fungizone [250 μg/mL]) at 4°C. Prior to slicing, tissue was washed with wash buffer (phosphate-buffered saline [PBS] supplemented with penicillin, streptomycin and fungizone). Slicing was performed aseptically using a Leica Vibrotome (Laboratory Instruments and Supplies, Meath, Ireland). Tissue was held using Dermabond (Johnson & Johnson Medical, Berkshire, UK) and the base discarded as waste. Slice thickness was set at 2000 μg and cut using a reciprocating blade at 22–26 rpm depending on the consistency of the tissue. Slices were incubated in six-well plates (1 slice/well) containing culture media at 37°C with 5% CO2 in a humidified environment.
DNA constructs
pCMV-luc plasmid, which expresses firefly luciferase under the transcriptional control of the cytomegalovirus (CMV) promoter, was purchased from Plasmid Factory (Bielefeld, Germany). Replication incompetent recombinant Ad5 particles under the transcriptional control of the CMV promoter and CXC chemokine receptor 4 (CXCR4) promoter were kind gifts from Professor Andrew Baker (University of Glasgow) and Professor David Curiel (University of Alabama), respectively, and generated as described previously. 18,24 Infectious particle concentration was determined by plaque assay using the ViraPower Adenoviral Expression Kit (Invitrogen, Dublin, Ireland), according to the manufacturer's instructions. An AAV plasmid expressing firefly luciferase under the transcriptional control of the CMV promoter was constructed and purified as described previously. 23
Plasmid/viral delivery
Cell number for slice thickness was estimated at 8 × 106 cells per slice based on an 80-cell-thick slice (2000 μm) and 8-mm slice diameter. Fifty micrograms of plasmid DNA in a volume of 50 μL (Buffer TE) were used for all non-viral methods. This was to ensure that plasmid DNA was not a limiting factor for gene expression, based on standard in vitro recommendations (1 μg per 1.9 × 105 cells). DNA was injected directly into the breast tumor slices. After treatment, slices were incubated at 37°C with 5% CO2 in a humidified environment. Media was supplemented with serum after two hours.
Viral vectors
The titer employed for different particles was based on optimum particle concentration. For Ad, 2.1 × 107 infectious particles per slice (average of 2.6 infectious particles per cell) were administered. However, in AdCMVLuc, this viral load saturated the Xenogen IVIS-bioluminescent detection system, and therefore 1 × 107 infectious particles (1.25 viral particles per cell) per slice were used for all subsequent trials with this vector. AAV titer employed was 1.1 × 108 infectious particles per slice (13.75 infectious viral particles per cell), which was based on experience with AAV used in murine therapeutic trials in our laboratory. 23 Fifty microliters of viral particles Ad5.CMVluc (1 × 107), Ad5.CXCR4luc (2.1 × 107) and AAVCMVLuc (1.1 × 108) were injected directly into the center of the tumor slice.
Electroporation
Plasmid DNA was injected into the center of the slice. After 90 s, pulses were delivered using a needle pair electrode. The tip of the electrode was carefully placed near the center of the slice, by controlling the depth of insertion relative to slice thickness. Pulses were generated using the Cliniporator (IGEA, Carpi, Italy) at one high-voltage pulse of 360 V followed by eight low-voltage pulses at 36 V. 25
Sonoporation
Plasmid DNA was injected into the center of the tumor slice. After 90 s, low-intensity US was delivered for five minutes using a 1-MHz US transducer (Sonitron 2000, Rich-Mar Corp, Inola, OK, USA) with a surface area of 5 cm2. The probe was held against the tumor throughout the duration of treatment. The parameters 1.0 W/cm2, 20% duty cycle was used. 26
Lipofection
Fifty micrograms of plasmid DNA were combined with 25 μL Lipofectamine 2000 (Invitrogen, Biosciences, Dublin, Ireland) (2:1) and incubated at room temperature for five minutes. The mixture was injected directly into the center of the tumor slice.
Tissue viability assessment
Viabilities of individual tissue samples were determined using propidium iodide (PI) by a Nucleocounter (ChemoMetec, BioImages Ltd, Cavan, Ireland) or fluorescence-activated cell sorting (FACS). Tissue samples are dissociated into a single-cell suspension using a combination of physical dissociation and enzymatic digestion. Briefly, the tumor slice is cut with a scalpel and incubated in culture media supplemented with Collagenase IV (1500 U per slice), Dispase (4.8 mg per slice) and DNAse (0.01 MU per slice) for 45 min at 37°C. Dissociated cells were removed at 15-min intervals and passed through a BD Falcon 70 μm nylon cell strainer (BD, Dublin, Ireland). Both systems are based on the uptake of PI by non-viable cells.
Histology and immunohistochemical detection of Ki-67-positive cells
For histological examination, tumor slices were fixed in 10% formaldehyde solution and embedded in paraffin. Sections (4 μm) were prepared and for conventional histology were stained with hematoxylin and eosin (H&E). In parallel sections, Ki-67-positive cells were immunohistochemically highlighted using the monoclonal antibody MIB1 (MIB1, Dianova, DEA 505) as described by Gerdes et al.
Ex vivo and in vivo comparison of gene delivery
All animal experiments were approved by the Ethics Committee of University College Cork. Female MF1 nu/nu mice were obtained from Harlan Laboratories (Oxfordshire, UK). For MCF-7 tumor induction, 1 × 106 tumor cells, suspended in 200 μL of serum-free DMEM, were injected subcutaneously into the flank. When tumors reached 1 cm diameter, mice were anesthetized using 100 μL intraperitoneal injection of PBS containing 1.5 mg ketamine hydrochloride (Veroquinol, Galway, Ireland) and 300 μg xylazine (Chanelle, Galway, Ireland) and tumors were removed. Tumors were sliced, treated and analyzed for gene expression at 24 h as described above. For in vivo experiments, mice were anesthetized before viral, lipofectamine and plasmid vectors were slowly injected into the center of the tumor. After 90 s, this was followed by either US or EP treatment. In US treatment, high viscosity coupling gel (Aquasonic 100) was used to improve skin contact.
Xenogen IVIS imaging
Tissue slices were maintained in six-well plates for analysis. Hundred microliters of 30 mg/mL firefly luciferin (Biosynth, Staad, Switzerland) were injected into the slices and 100 μL was added into media. After 10 min of incubation, slices were imaged for five minutes using the IVIS Imaging System (Caliper Life Sciences, Cheshire, UK). For whole body imaging of mice, 100 μL of luciferin was injected intratumorally and 100 μL intraperitoneally. At 10 min post-luciferin injection, mice were anesthetized and imaged for three minutes. All measurements were obtained using Living Image 2.6 application. 27
Epithelial cell analysis of tumor slices
Tumor slices were dissociated into a single-cell suspension fixed using 70% ethanol and permeabilized using IFA-tx buffer (2% FCS, 10 mmol/L HEPES, 0.1% Triton X-100, 0.1% sodium azide and 150 mmol/L NaCl) buffer. Cells were incubated for one hour with pan-cytokeratin (3 μg) antibody tagged with phycoerythrin (PE) (clone C-11) (Abcam, Cambridge, UK).
Cell-type-specific expression
Slices were dissociated, fixed and permeabilized as above. Cells were dual-stained sequentially for one hour on ice with pan-cytokeratin antibody tagged with PE (3 μg), and primary luciferase antibody (10 μg) (clone Luci17) (Abcam) and a secondary cyanine 5 (Cy5) antibody (1:500) (Abcam).
Statistics
Calculation of means, standard deviation and standard error of the mean was performed using GraphPad Prism (V 3.0, San Diego, CA, USA). Statistical significances of the differences between the individual groups were determined by using the two-tailed Student's t-test for paired values. Differences with a P value <0.05 were considered significant.
Results
Optimization of tissue slice model system
The optimum temperature for collection and storage of tissue was determined to be 4°C (data not shown). At this temperature, viability was unaffected over a 12-h period and it prevented the occurrence of microbial infections before processing. The minimum thickness for accurate intratumoral gene delivery by direct injection and for the application of EP and sonoporation devices was 2 mm. The greatest transfection efficiency was found to occur in the absence of serum (data not shown) and consequently this was employed in all treatments. Serum was subsequently added two hours after treatment for all methods.
Cell viability and characterization of cultured tumor slices
To mimic in vivo conditions, efforts were aimed at maintaining slices in their constituent cellular components. In order to avoid stimulation of particular cellular populations, slices were maintained in standard culture medium. PI viability assays were employed to assess total cell viability at various time points after surgical resection prior to cultivation. The optimum harvesting time after surgical resection for breast tumors was within 30 min, with viability dropping by 80.2% after 90 min (Figure 1a). All samples used for subsequent analyses were harvested within 30 min of resection from patients.
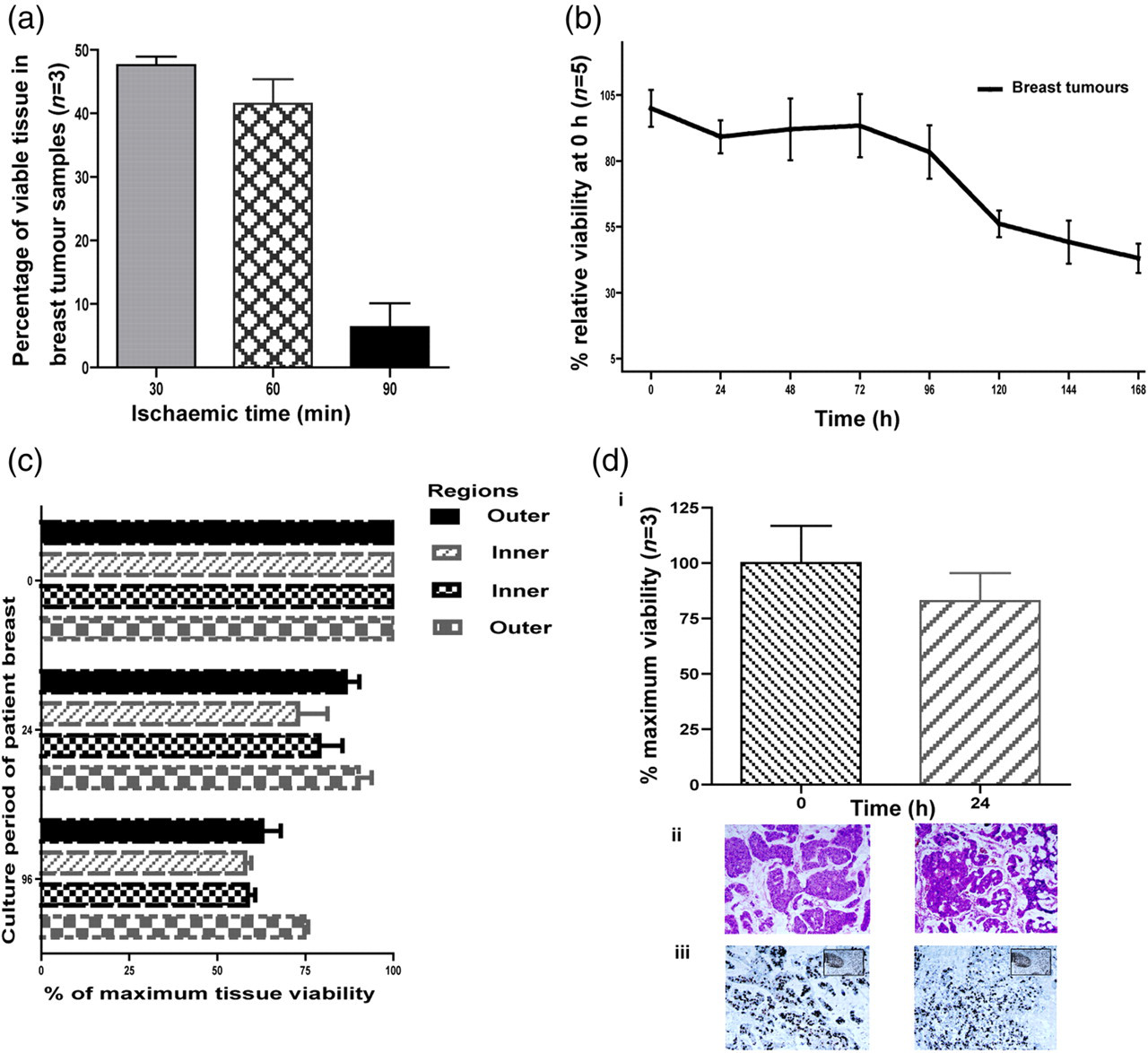
Cell viability and characterization in cultured tumor tissue. (a) Influence of time on sample recovery. A propidium iodide assay was used to assess cell viability at various time points (30, 60, 90 min) after surgical resection prior to cultivation. (b) Viability of cells in culture over time. Slices were cultured and viability at various time points assessed over a period of seven days. (c) Intratissue variability in viability. Intraslice viability was assessed by further dividing cultured slices into 500 μm regions at either 24 or 96 h and viability was assessed. (d) Cell type characterization and histological analysis. Epithelial cell component of slices was examined by flow cytometry before cultivation and 24 h after using pancytokeratin marker (i). Histological assessment by hematoxylin and eosin (ii) and anti-Ki67 (iii) staining was carried out at 0 and 24 h. Proliferating Ki67-positive cells stain black. Inset demonstrates positive control (A color version of this figure is available in the online journal)
The efficiency of the culture method in retaining tissue viability over time was examined (Figure 1b). An initial decrease in viability observed at 24 h may be attributed to an adaptability period to culture conditions and therefore prior to all treatments, slices were incubated in culture medium for two hours at 37°C to ensure slice adaptation prior to treatment. Viability assays showed that slices were able to maintain 80% of original viability for up to 96 h (Figure 1b). The decrease in slice viability after 96 h is most likely due to a negative cell turnover (cell death > cell proliferation). Previously reported studies have only maintained ex vivo tissue viability for a shorter period of four days. 19 In order to examine the uniformity of viability throughout the tissue section, intraslice viability was assessed. No marked difference was observed between regions within the slice and there was a proportionate decrease in viability in all regions over time (Figure 1c). Flow cytometric analysis of epithelial cells indicated that a significant proportion of tumor cells (82.3 ± 12.3%) was still present after 24 h of culture when compared with precultured tissue (Figure 1d). Histological analysis at 0 and 24 h revealed no significant change in morphology or apoptosis as detected by H&E (Figure 1d [ii]). Proliferative cells were present at 0 and 24 h detected by anti-Ki 67 staining (Figure 1d [iii]). Thus, this culture system was capable of maintaining the desired viability and tumor component required for the application and assessment of gene delivery methods.
Realtime luminescence imaging of ex vivo tissue permits assessment of gene delivery and expression over time.
The optimized culture model was employed to assess and compare gene delivery systems. Breast tumor slices were administered CMV-firefly luciferase DNA cassette according to Materials and methods using various gene delivery methods and expression analyzed at various time points post-treatment. Parameters for various gene delivery methods were optimized in various cell lines and MCF-7 tumors in vivo. A method for realtime IVIS imaging of ex vivo tissue slices transfected with luciferase was developed. Luminescence per gene copy administered was determined and results are displayed in Figure 2a, which represents maximum gene expression for various methods at their optimum time point. Ad has highest gene expression at 48 h, while AAV peaked at 120 h. The highest expression for lipofectamine was found at 72 h, while no further increase in gene expression was found after 24 h for both US and EP unlike all other delivery methods. The results obtained with AAV, which requires the longest time for optimum expression (5 d) correlates with various published in vivo time course studies. Ad proved to be the most efficient vector overall with US providing highest reporter gene expression among the non-viral methods in breast tumor tissue.

Assessment of gene delivery in breast tumor tissue. (a) Gene delivery in patient breast tumor samples. Breast tumor slices were treated ex vivo with various gene delivery methods. Luciferase activity at optimum time points for each delivery method (EP [electroporation] and US [ultrasound] – 24 h, Ad [adenovirus] – 48 h, Lipo [lipofection] – 72 h, plasmid – 24 h, AAV [adeno-associated virus] – 120 h) was detected by an IVIS-luminescence system following addition of substrate to culture medium. Luminescence units are displayed per gene copy administered. Representative images of luminescence readings are displayed below. (b) Comparison of gene delivery methods in ex vivo and in vivo models. MCF-7 tumor xenografts were treated ex vivo (squares, z-axis) or in vivo (bars, y-axis) with the various methods as above. The pattern of relative efficiencies of methods in vivo (Ad > AAV > Lipo > EP > US > Plasmid) was generally reflected ex vivo except in the case of Ad and US, which provided higher relative efficiency ex vivo (A color version of this figure is available in the online journal)
Comparison of ex vivo and in vivo analyses
To assess consistency with the in vivo setting, we performed in vivo and ex vivo MCF-7 xenograft gene transfections using all methods. For practicality purposes, a xenograft model was used instead of spontaneous or induced models because of the relative ease in obtaining tumors of similar volumes. Spontaneous or induced models would more closely represent the tumor state in patients in relation to organ-specific physiology and immunogenicity. They, however, have slow and unpredictable growth rates and therefore require large numbers to obtain sufficient homogenous tumor experimental groups. The time point for maximum expression in vivo for each method was used to measure luminescence. The pattern of relative efficiencies of methods in vivo (Ad > AAV > Lipo > EP > US > plasmid) was reflected ex vivo except in the case of US which provided higher relative efficiency ex vivo. Both EP and Lipo performed better in the in vivo setting. However, there was a marked reduction in the efficiency of Ad and US as delivery methods in vivo. This suggests the activity of in vivo factors adversely affecting gene delivery and/or expression, which are absent in the ex vivo model for these methods (Figure 2b).
Examination of biological barriers to US gene delivery
Among the non-viral methods examined here, US provided the greatest gene expression ex vivo in patient tumor tissue. In murine trials, the high level of US transfected gene expression was only seen ex vivo with significant reduction in vivo. To investigate the reasons for the dramatic differences between US results ex vivo and in vivo (Figure 2b), we examined the involvement of physical factors that are not present ex vivo, as potential biological barriers to US gene delivery in vivo. We investigated the following physical factors: presence of blood, skin and temperature and tumor variables of tumor type, tumor stage (primary versus metastatic tumor) and tumor US wave penetration.
The presence of whole patient blood acted as a barrier to all gene delivery methods, with the most significant effect on US as shown in Figure 3a. Separation of blood into cellular and serum components showed that US was only adversely affected by the cellular component of blood (data not shown). US may enhance gene delivery by either thermal or non-thermal effects. The thermal effect caused by US is due to the absorption of US waves. US application results in a 0.5–1.0°C rise in tissue temperature; yet increasing tissue temperature to 39°C only moderately increased gene expression by plasmid delivery, which was still significantly lower than US (data not shown). However, combining hyperthermia (39°C) with US improved transfection by 200%, without affecting viability (Figure 3b). Increasing temperature beyond 39°C resulted in dramatic reduction in viability and gene expression per viable cell (data not shown).
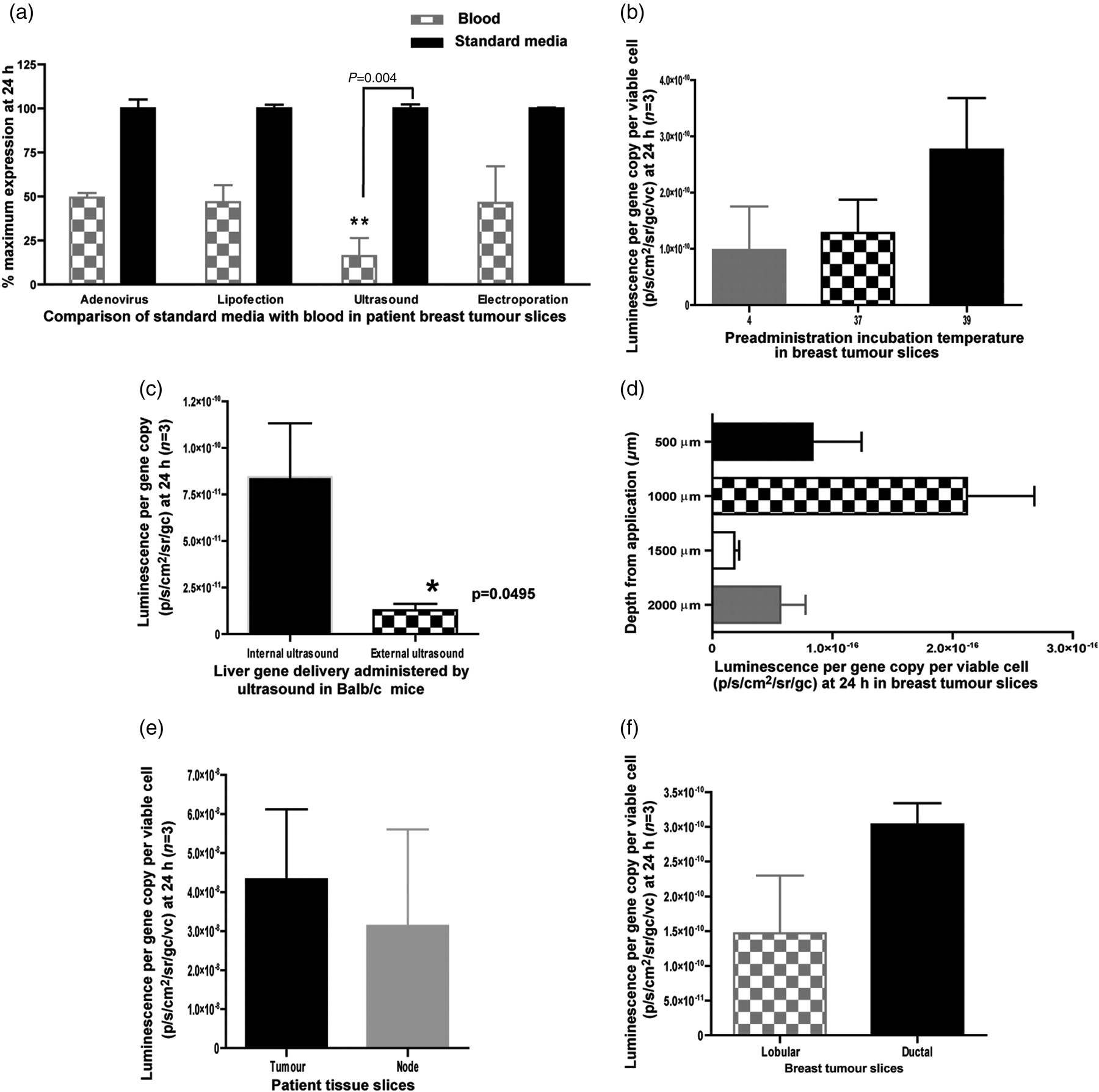
Biological barriers to ultrasound (US)-related reporter gene expression. (a) Breast tumor slices were treated with various gene delivery methods in the presence of the patient's own blood. After treatment, slices were removed from blood, washed, cultured and assessed for gene expression and viability. (b) Tumor slices were incubated at various temperatures for two hours prior to gene delivery and culture as normal. Resulting expression and viability was analyzed at 24 h. (c) The effects of the presence of skin between the US probe and target tissue were assessed in a Balb/C murine model, where treatment was performed on the liver either under the skin or over it and in vivo luminescence was assessed using IVIS imaging. (d) Tumor slices were examined for maximum reporter gene expression and viability with respect to distance from US probe. (e, f) US treatment was examined in ductal, metastatic nodal and lobular tissue
As evidenced by in vivo US-mediated delivery to mouse liver, overlying skin reduced transfection by 40% when compared with direct contact (Figure 3c). The optimal distance from the US probe for highest transgene expression (Figure 3d) was also investigated. Maximal luminescence was seen in the tissue area 500–1000 μm from the US probe. The layer closest to the probe did not show significantly reduced viability following US application (data not shown) indicating that the observed luminescence was due to maximum efficiency of gene delivery sonic waves 500–1000 μm from the US probe, rather than a high rate of cell killing outweighing DNA delivery in the tissue closest to the probe. US gene delivery was as effective in secondary nodal tumors compared with primary ductal tumors from the same patients (Figure 3e). However, gene expression was reduced in tissue slices originating from lobular tumors when compared with ductal tumors from three different patients (Figure 3f).
Examination of biological barriers to Ad gene delivery
Ad vectors are extremely efficient gene delivery agents and target a wide host tissue range. However, various physical factors can limit gene expression. As previously mentioned, in Figure 3a, blood is a barrier to all methods, reducing Ad gene expression by 50%. Ad demonstrated good penetration of solid tumors, with comparable expression in all regions of the slice (Figure 4a) However, gene expression was significantly reduced (P = 0.045) in nodal metastatic disease (Figure 4b), suggesting reduced transduction in metastatic tissue unlike observations with US (Figure 3b).
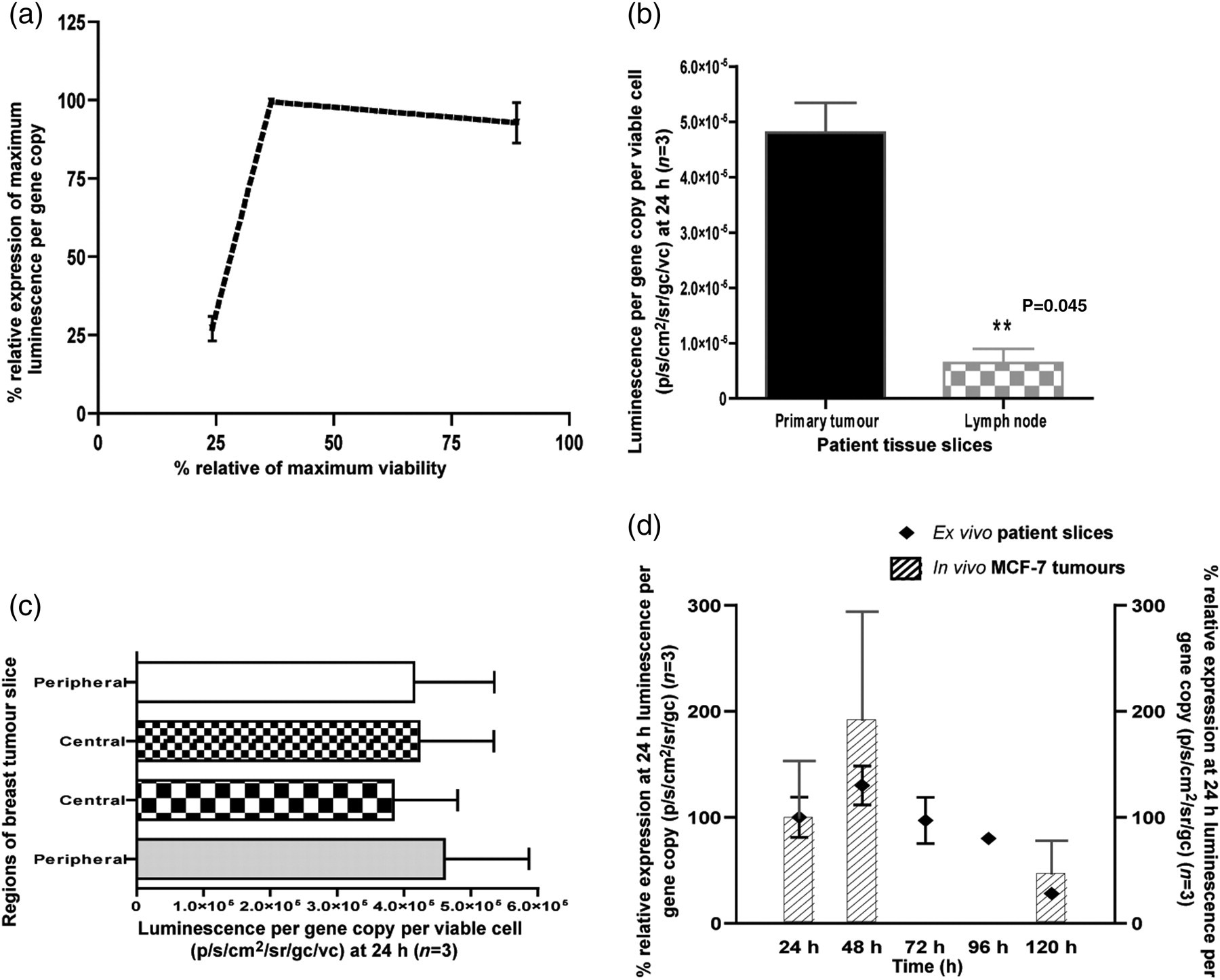
Biological barriers to adenovirus-related reporter gene expression. (a) Breast tumor slices were administered Ad5CMVluc and incubated at 37°C for 24 h. Slices were further sliced into 500 μm regions and luciferase expression and viability were assessed at 24 h. Viability for each region was analyzed by creating a single-cell suspension and performing propidium iodide assay (n = 3). (b) Breast tumor slices from the primary tumor and metastatic nodes were assessed for Ad5CMVLuc gene expression and viability at 24 h (n = 3). (c) Breast tumor slices at 24 h after central Ad5CMVluc administration were sliced into four equal regions and assessed for gene expression and viability. (d) Gene expression for Ad5CMVluc-administered slices was assessed every 24 h for five days compared with corresponding in vivo MCF-7 tumors (n = 3)
Solid tumors are associated with regions of reduced viability due to hypoxic conditions. Regional tissue viability can affect treatment in two ways: by reducing gene delivery and/or by its effect on gene expression. In our studies, viability was observed to have a linear relationship with naked plasmid-mediated transgene expression (data not shown). With Ad, reporter gene expression was unchanged at viability rates above 40% of maximum viability, with significant reduction at viabilities below this threshold, suggesting saturation in luminescence readings or gene delivery above this limit (Figure 4c). Measurement of gene expression over time showed maximum expression at 48 h, correlating with in vivo data, with 70% reduction in gene expression at day 5 (Figure 4d).
Validation of system using malignant and non-malignant tissues
In order to further examine the culture and imaging system in a setting aimed at qualifying as well as quantifying reporter gene expression, we compared the tissue/cell selectivity of luciferase expression under the control of gene promoters with disparate expression profiles in malignant and normal tissues. While CMV is ubiquitously expressed, CXCR4 is considered to be differentially expressed in tumor cells. 28–30 Ad vectors featuring the firefly luciferase gene under the control of either the CMV or CXCR4 promoter were examined in breast tumor, normal colon and normal liver tissues. Normal liver and colon was used rather than normal breast due to the fatty consistency of normal breast tissue making slicing impractical. When examined by bioluminescent imaging, Ad5CXCR4Luc demonstrated tumor tissue selectivity, with significantly improved normal to tumor ratio when compared with Ad5CMVLuc (Figure 5a). To quantify transduction efficiency within tumor and normal tissue with both Ad vectors, we optimized a method of gentle tissue dissociation using both chemical and physical means to isolate a representative population of cells. Ad-mediated luciferase expression was examined by flow cytometry in cell suspensions derived from slices 48 h after treatment. We demonstrated transduction efficiency (% luciferase positive cells) of Ad5CMVLuc (30.9 ± 7.7%) and Ad5CXCR4Luc (11.3 ± 0.9%) in breast tumor slices (Figures 5c and d, respectively). This specificity was confirmed in analysis of liver samples, with 10.6% (±3.4) liver epithelial cells luc+ in Ad5CMVLuc-administered samples, compared with 0.6% (±0.4) in the case of Ad5CXCR4Luc (Figures 5e and f, respectively) and in colon samples, with 20.3% (±8.4) colon cells luc+ in Ad5CMVLuc compared with 0.77% (±0.15) in Ad5CXCR4Luc (Figure 5g and h, respectively). Graphical representation of transduction efficiency ratios in tumor, colon and liver is shown in Figure 5b. However, human tumors are composed of a variety of cells, of which only ∼30% represent the tumor population. Hence, to assess cell type selectivity within the slices we co-localized transfected populations with an epithelial tumor cell marker, pancytokeratin. Analysis of tumor cell populations revealed that Ad5CXCR4Luc had a higher selectivity for expression in epithelial tumor cells (93.7% [±6.2] epithelial cells luc +; 6.25% [±3.46] non-epithelial cells luc+) when compared with Ad5CMVLuc (75% [±8] epithelial cells luc +; 25% [±8] non-epithelial cells luc+) as shown in Figures 5e and f, respectively. Figure 5i demonstrates graphical representation of epithelial cell transduction in tumors with both Ad vectors confirming selectivity of AdCXCR4Luc expression in tumor epithelial cells.

Comparative analyses of cytomegalovirus (CMV) and CXC chemokine receptor 4 (CXCR4) promoter activity in tumor, liver and colon patient samples. Breast and liver patient samples were administered Ad5CMVLuc or Ad5CXCR4Luc and incubated at 37°C for 24 h. (a) Bioluminescent imaging at 48 h demonstrates a greater tumor specificity of AdCXCR4Luc when compared with Ad5CMVLuc. Percentage luminescence in liver and colon is expressed relative to tumor. Slices were dissociated into single-cell suspensions and fixed with 70% ethanol. To establish transduction efficiency (% luc + cells), cells were stained with anti-luciferase antibody (detected as cyanine 5-labeled cells [red 2A]) and to identify epithelial tumor cells, populations were stained with a pan-cytokeratin antibody (detected as phycoerythrin labeled cells [PE-A]). (b) Comparison of transduction efficiency of Ad5CMVLuc and Ad5CXCR4Luc in tumor, colon and liver samples. Percentage luciferase expression in liver and colon is expressed relative to tumor. (c, d) Representative flow cytometric analysis of tumor cells with Ad5CMVLuc (c) and Ad5CXCR4Luc (d) stained with luciferase antibodies (right panels) and corresponding non-specific IgG (left panels). Percentage of cells in Q4 represent those cells expressing luciferase in Ad5CMVLuc (30.9 ± 7.7%) and Ad5CXCR4Luc (11.3 ± 0.9%). (e, f) Representative flow cytometric analysis of liver patient samples with Ad5CMVLuc (e) and Ad5CXCR4Luc (f) stained with luciferase antibody (right panels) and corresponding IgG (left panels). Percentage of cells in Q2 represents those cells expressing luciferase in Ad5CMVLuc-Liver (10.6 ± 3.4%) and Ad5CXCR4-Liver (0.6 ± 0.4%). (g, h) Representative flow cytometric analysis of colon patient samples with Ad5CMVLuc (g) and Ad4CXCR4Luc (h) stained with luciferase antibody (right panels) and corresponding IgG (left panels). Percentage of cells in Q1–Q2 represent those cells expressing luciferase in Ad5CMVLuc (20.3 ± 8.4%) and Ad5CXCR4Luc (0.77 ± 0.15%). Tumor samples transduced with Ad5CMVLuc and Ad5CXCR4Luc were counterstained with pancytokeratin. Percentage luc+ epithelial tumor cells in Ad5CMVLuc-tumors (75 ± 8%) and Ad5CXCR4Luc-tumors (93.7 ± 6.2%) are presented in Q2 (right panels) and corresponding IgG (left panels). (i–k) Quantification of epithelial and non-epithelial fractions of luc+ tumor cells from Ad5CMVLuc (75% [±8] epithelial cells luc + ; 25% [±8] non-epithelial cells luc+) and Ad5CXCR4Luc (93.7% [±6.2] epithelial cells luc + ; 6.25% [±3.46] non-epithelial cells luc+). Percentages shown are averages of three independent experiments
Discussion
The major focus of this study was to determine whether ex vivo tumor slices could be used to compare various gene delivery methods using a realtime bioluminescence detection system for quantitative assessment of gene expression in patient samples. This ex vivo model enables the assessment of gene delivery methods on the complex three-dimensional (3D) architecture, tumor heterogeneity and phenotypic variation that is present in vivo. The maintenance of significant viability is crucial for ex vivo cultivation. 31 In order to evaluate the suitability of this novel system, we studied the effects of culture conditions on tumor cell viability and variations in tumor cell populations over time. The tissue slices were maintained for up to seven days with sustained viability, ensuring appropriate response to various gene delivery experiments and allowing the use of methods requiring longer incubation periods for maximum expression such as AAV. There have been a number of publications over the last 10 years on the use of ex vivo tumor slices with specific individual viral vectors. 18,19 However, only single methods were applicable using these models; valuable insights on tumor biology ex vivo and their effects on gene delivery were not fully explored. Our model uses a comparatively thicker slice of tumor tissue when compared with other model systems. Through optimization, we achieved an important balance between ensuring adequate diffusion of nutrients and oxygen to the inner regions of the slice and facilitating the physical delivery of genes by direct injection, the application of EP and sonoporation devices and enabling in-depth intraslice analysis. Our approach of tumor dissociation for the analysis of PI uptake, cell markers and transduction efficiency allows for the examination of a representative, viable cell population in the relative proportions found in the intact tumors. This, we believe, gives a more detailed and accurate representation of the cells in the slices that may be unavailable in the intact tissue. 32 Access to high-quality screening in developed countries has resulted in the detection of breast cancer at an earlier stage, leading to a decrease in the incidence of large tumors and thus less patient tissue available for research purposes. Even though our model uses a large slice of tumor, the bioluminescence detection system we have developed allows the accurate analysis of gene expression over time without sequential sacrifice of tissue, as with previous models, minimizing wastage of valuable patient material. To allow for differences in tissue composition and variation in transfectability between patient samples, it was important to compare all methods on tissue from the same patient. Despite marked heterogeneity between patient samples, we found Ad to be the most effective vector overall, correlating with existing evidence in the field. 33 The finding that US provided the optimal transgene expression for ex vivo human breast tumor slices among non-viral methods was surprising. When we repeated these experiments in MCF-7 xenografts, we found a similar trend in the ex vivo setting; however, both methods had a significantly lower transfection efficiency in the in vivo setting. This suggested to us that physical conditions were inhibiting both methods from demonstrating their maximum transfection ability in vivo.
The nature of the ex vivo system permitted the examination of specific physical factors individually, which can account for this reduction in gene delivery. Furthermore, comparing delivery to distinct histological types and stages of disease in breast cancer can be studied. The physical factors investigated were blood, regional viability, tumor penetration, skin, tumor type and temperature. Large bulky tumors, fluctuations in body temperature and the skin barrier are frequently encountered in the clinical setting. Solid tumors are known to possess a tortuous and leaky vasculature and can have significant variations in regional viability 34 while regional lymph nodes are the commonest site for metastatic spread in breast cancer. Our experiments show that blood, reduced viability and nodal tissue are factors that adversely affect Ad gene delivery. The reduction of gene expression in nodal tissue is likely to be due to physical properties of nodal tissue rather than phenotypic variation in nodal tumor cells. Lymph nodes are composed of a fibrous capsule and a supporting meshwork of connective tissue and extracellular matrix (ECM) components have previously been shown to reduce adenoviral gene delivery. 35 The use of degradation enzymes of ECM components, such as hyaluronidases, may improve Ad gene delivery to involved lymph nodes. In primary tumors, Ad demonstrated a transduction efficiency of up to 50%, and was potent at penetrating all regions of the slice. However, this efficiency was not accompanied by long-term gene expression with >70% reduction in expression within five days. Reduction in gene expression may be attributed to either cell turnover or cell death in the ex vivo tissue. In MCF-7 tumors, when comparing ex vivo with in vivo gene expression, there was significant reduction (50% and 74% respectively) in gene expression in vivo which may be linked to the presence of a systemic immune response in vivo which is absent in an ex vivo model. US gene delivery offers good penetration of nodal tissue and a temperature rise of 2°C greatly enhanced gene delivery. Expression is significantly reduced by the presence of overlying skin and blood, and it offers a reduced penetration of tumor slices. These findings indicate that Ad may be a better candidate vector for the targeting of large solid tumors. US offer a better safety profile albeit a less efficient alternative to Ad. Its greatest benefit may be in the treatment of superficial, small and relatively avascular involved nodes of the chest wall or axilla. The targeting of viable regions and a temporary blood-free field would improve transfection ability for all methods. The use of imaging modalities such as color flow Doppler to identify neo-vascularity, 36 and hence target viable regions, and the application of vasoconstrictor agents to reduce blood exposure prior to treatment will improve gene delivery. In addition, heat delivery systems may improve US-mediated treatment delivery.
The model is not confined to tumor studies and allows for intertissue variations to be assessed. The chief safety concern with Ad use is activation of the inflammatory response syndrome. 37 Slow intratumoral delivery of Ad and the use of polymeric delivery systems 38 reduce systemic dissemination. Yet, there can be significant viral loads systemically disseminated due to a delivery-induced convective transport into leaky vessels which leads primarily to accumulation in the liver. 39 The predilection for liver accumulation in vivo may be due to the detoxifying activity of the liver, making it inherently prone to ‘capture’ foreign particles. This unwanted effect from dissemination may be limited by the integration of unique promoters in viral vectors, which are highly expressed in tumor cells, with little or no expression in normal cells. Ad-expressing luciferase under CXCR4 control was found to improve tumor cell targeting with relative sparing of non-tumor cells in patient tumor slices, and moreover reduced gene expression in non-target tissue (liver slices). Comparison of tumor selectivity of the CXCR4 promoter evaluated by bioluminescence and FACS revealed good correlation with previous publications with regard to both tissue type and cell population. The tumor-cell selective transgene expression would suggest that Ad utilizing the CXCR4 promoter would also support the systemic targeting of disseminated disease with minimal non-target effects and moreover allow early postsurgical treatment.
Conclusions
Our study demonstrates for the first time that bioluminescence imaging of luciferase-transfected patient tumor slices can be used for the assessment of gene delivery methods and to study physical barriers to gene delivery. Bioluminescent imaging provides a rapid, economical and simple method for monitoring gene expression. Furthermore, it offers an attractive alternative to animal trials and may provide a more accurate representation of patient response. A range of commonly employed gene delivery methods with potential for breast tumor therapy were examined with this strategy. We did not examine other vector types such as nanoparticles 40–42 or bacterial vectors, 43 but it is likely that the model system developed here is applicable to all vector types. Furthermore, the model is not confined to gene delivery assessment. The extended duration of culture period and 3D architecture of this model makes it applicable to the studies of novel gene therapeutic strategies where the interplay between tumor cells and the microenvironment is important. The findings from this study and potential relevance in the clinical setting highlight the importance of meticulous evaluation prior to entering clinical trials.
Footnotes
Acknowledgements
The authors thank Dr Martina Scallan, Microbiology Department UCC, for use of AAV facilities and the Pathology Department, Mercy University Hospital and Surgical Department, South Infirmary Victoria University Hospital, for aiding collection of patient samples. This work was funded through the Cork South Infirmary Victoria University Hospital Breast Fund, the Irish Cancer Society (CRI07TAN) and the Cork Cancer Research Centre.