
Abstract
Glutathione S-transferase M1 (GSTM1) might be involved in inactivation of procarcinogens that contribute to the genesis and progression of cancers. GSTM1 null status has been extensively studied as a risk factor in bladder cancer susceptibility. The aim of this study is to evaluate the role of GSTM1 null genotype in bladder cancer risk. All available studies were considered in this meta-analysis, including 7301 cases and 9405 controls from 33 studies. Significantly increased risk was detected between GSTM1 deletion and bladder cancer susceptibility in all subjects (odds ratio [OR] = 1.409 [1.267–1.568], P < 0.001). The same patterns were observed in Caucasians (OR = 1.434 [1.212–1.697], P < 0.001) and Asians (OR = 1.485 [1.295–1.704], P < 0.001). When stratified with study design, a positive association was also found in hospital-based studies (OR = 1.552 [1.382–1.744], P < 0.001), but no association in population-based ones (OR = 1.088 [0.970–1.221], P = 0.151). In summary, our meta-analysis suggested that GSTM1 null status is associated with a high increase in the risk of bladder cancer, and further studies based on population design are necessary to confirm our conclusion.
Introduction
Bladder cancer is one of the most common cancers of the urinary tract, and it is caused by a complex combination of genetic and environmental factors. Risk factors for bladder cancer include cigarette smoking, exposure to industrially related aromatic amines and intake of carcinogenic drugs such as phenacetine, chlornaphrazine and cyclophosphamide. 1,2 Procarcinogens are mainly metabolized by various metabolizing enzymes, and a considerable number of studies have focused on the association of genes for metabolizing enzymes of carcinogens and cancers.
Mammalian glutathione transferases (GSTs) are dimeric enzymes with subunits of 199–244 amino acids in length that catalyze conjugation of electrophilic substrates with glutathione, usually resulting in detoxification of reactive intermediates. 3,4 The glutathione S-transferase M1 (GSTM1) gene belongs to the GST gene family and catalyzes the detoxification of polycyclic aromatic hydrocarbons (PAHs) that consists of many well-recognized mutagenic or carcinogenic agents.
GSTM1 plays a protective role against the development of cancers. The deficiency of this enzyme activity is caused by the inherited homozygous absence of the GSTM1 gene, the ‘null’ genotype (GSTM, 0/0). 5 Bell et al. 6 first reported the association between GSTM1 deficiency and increased bladder cancer risk, and subsequent studies have appeared with supporting findings. 7 However, many researchers have not found such a relationship. 5,8 Inconsistent results might be due to the relatively small sample sizes and differences in study populations. To strengthen the evidence, we performed a meta-analysis to examine the association between GSTM1 polymorphism and bladder cancer risk.
Materials and methods
Identification and eligibility of relevant studies
To identify all articles that examined the association of GSTM1 polymorphism with bladder cancer, we conducted a literature search of the PubMed database and the ISI Web of Knowledge database up to August 2010 using the following MeSH terms and keywords: ‘Glutathione S-transferase M1 or GSTM1’, ‘bladder neoplasm or bladder cancer’ and ‘polymorphism’. Eligible studies included in the meta-analysis had to meet the following criteria: (a) a case-control bladder cancer study; (b) the diagnosis of bladder cancer patients was confirmed pathologically; and (c) written in English.
Data extraction
Two investigators independently extracted data and reached a consensus on all of the items. The following information was extracted from each study: first author, years of publication, ethnicity of study population, the source of controls and the number of cases and controls. The multiplex-polymerase chain reaction method was performed in all included studies. Different ethnicities were categorized as Caucasian, Asian, African and mixed individuals. Concerning the source of controls, studies were also categorized as either population-based or hospital-based (Table 1).
Main characteristics of all studies included in the meta-analysis
HB: hospital-based study; PB: population-based study
Statistical analysis
The effect of association was indicated as odds ratios (OR) with the corresponding 95% confidence interval (CI), and the OR was calculated according to the method of Woolf. 42 A chi-square-based Q-statistic test 43 and an I 2 test 44 were performed to assess the heterogeneity between studies (I 2 < 25% no heterogeneity; I 2 = 25–50% moderate heterogeneity; I 2 > 50% large or extreme heterogeneity). The heterogeneity was considered statistically significant with P < 0.10. For a P value greater than 0.10 for the Q-test, the pooled OR estimate of each study was calculated using the fixed effects (Mantel–Haenszel) model. Otherwise, the random effects (RE) (DerSimonian and Laird) model was used. 43 The significance of the pooled OR was determined by the Z-test; a P value of <0.05 was considered significant. Publication bias was investigated by funnel plot, and an asymmetric plot suggested possible publication bias. The funnel plot asymmetry was assessed by Egger's linear regression test. 45 The t-test was performed to determine the significance of the asymmetry, and a P value of <0.05 was considered a significant publication bias. Meta-analysis and meta-regression analysis were carried out using Stata version 8.0 (Stata Corporation, College Station, TX, USA).
Results
Eligibility
Through a literature search and selection based on the inclusion criteria, 33 studies were identified. 9–41 Table 1 lists the identified studies and their main characteristics. The data for this analysis included 7301 cases and 9405 controls for GSTM1 polymorphism. The studies were published between 1996 and 2010. All studies were conducted in various populations of different ethnicities: 17 were conducted in populations of Caucasian ethnicity, 9,13–15,17–19,21,23,27,31,34,35,37–39,41 10 involved Asians, 12,16,24–26,29,30,32,33,36 four mixed 10,20,22,28 and two Africans. 11,40 We also stratified all studies considering the source of controls: 20 were hospital-based studies 9,12,14–21,24,27,29–32,34,36,38,41 and 13 were population-based ones. 10,11,13,22,23,25,26,28,33,35,37,39,40
Meta-analysis results
Extreme heterogeneity was found among the 33 eligible studies (I 2 = 72.6; P < 0.10). The overall data showed that the individuals who carried the GSTM1 null genotype had a significantly increased bladder cancer risk compared with those who carried the GSTM1 present genotype in all subjects (OR = 1.409 [1.267–1.568], P < 0.001) (Figure 1a). In subgroup analyses, the same significant associations were found in Caucasians (OR = 1.434 [1.212–1.697], P < 0.001) and Asians (OR = 1.485 [1.295–1.704], P < 0.001) (Table 2).
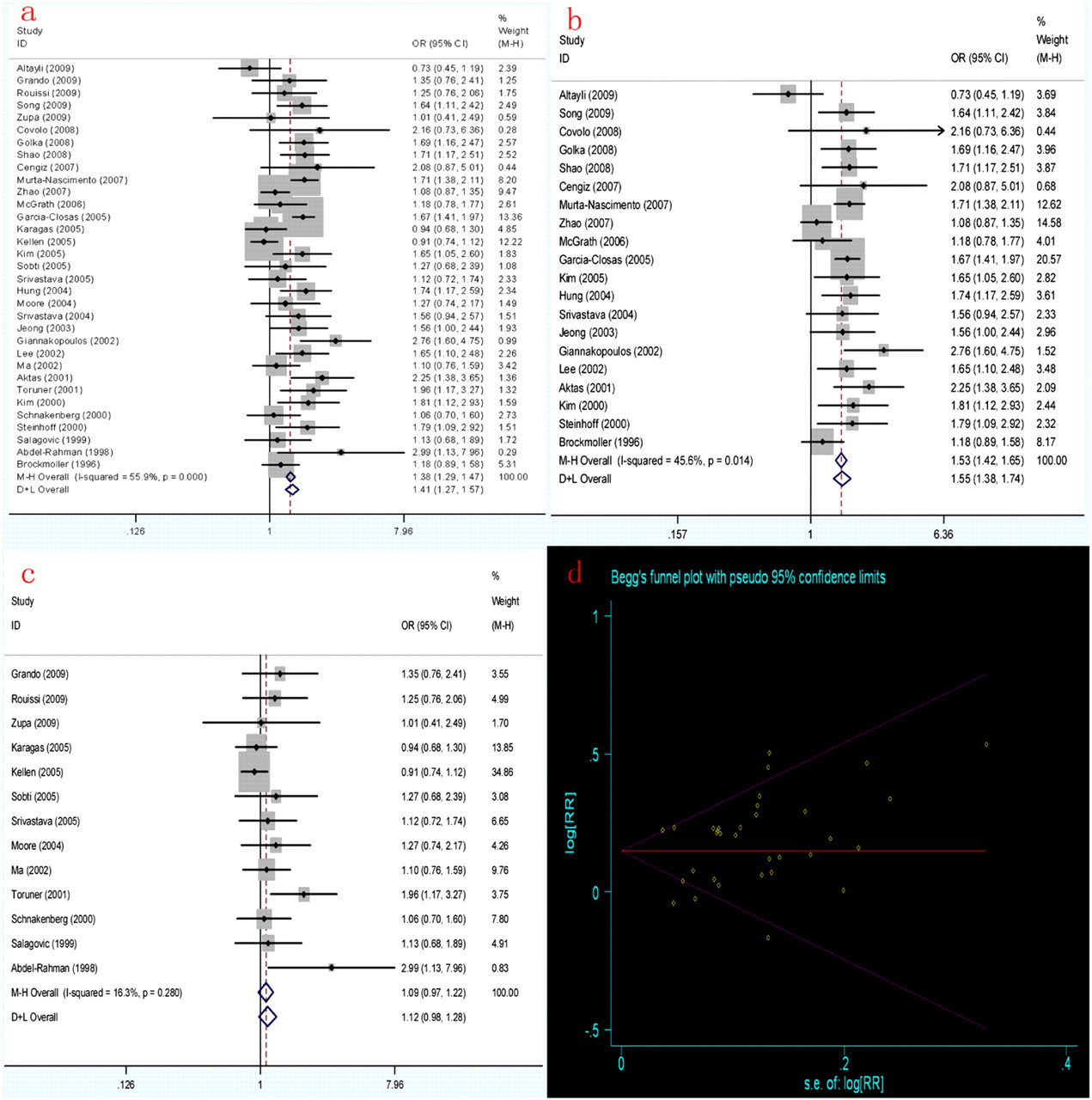
Meta-analysis of GSTM1 polymorphism in bladder cancer. The study is shown by a point estimate of the OR and accompanying 95% CI: (a) overall analysis for contrasts under FE (M-H) and RE (D + L) models; (b) overall analysis for contrasts under FE and RE models in hospital-based studies; (c) overall analysis for contrasts under FE and RE models in population-based studies; (d) Begg's funnel plot of the Egger's test of the comparison for publication bias. FE, fixed effects; M-H, Mantel–Haenszel; RE, random effects; D + L, DerSimonian and Laird. (A color version of this figure is available in the online journal)
Summary of ORs for GSTM1 polymorphism and bladder cancer risk
Ph: P value of Q test for heterogeneity test; OR, odds ratio; CI, confidence interval
*Number of comparisons
In stratified analysis according to the source of controls, the GSTM1 null genotype showed a significant association with increasing bladder cancer susceptibility in hospital-based studies (OR = 1.552 [1.382–1.744], P < 0.001) (Figure 1b). However, no association was found in population-based studies (OR = 1.088 [0.970–1.221], P = 0.151) (Figure 1c).
Sensitivity analysis
Sensitivity analysis was performed both by sequential removal of individual study and cumulative statistics of all subjects and subgroups. The pooled ORs of GSTM1 null genotype were not influenced by the result of any individual study in all subjects, subgroups and hospital-based studies. However, the pooled OR in population-based studies turned out to be subtly significant (OR = 1.181 [1.126–1.358], P = 0.020) when one study 23 was excluded. The same result was also produced using cumulative statistics.
Publication bias
Funnel plots and Egger's test were performed to assess publication bias. The data suggested that there was no evidence of publication bias in GSTM1 polymorphism (t = 1.41, P = 0.168) (Figure 1d).
Discussion
GSTM1 detoxifies hydrophobic electrophiles derived from the metabolism of xenobiotics, including PAH-derived epoxides. Previous studies have indicated that the GSTM1-null genotype is associated with increased risk for tobacco-related cancer due to a decreased ability to detoxify PAH. 46–48 In the present study, 33 studies on the GSTM1 genotype (16,706 subjects) were critically reviewed. Meta-analysis showed significant associations between GSTM1 null genotype and bladder cancer risk in all subjects, Caucasians and Asians. However, no association was found in population-based studies (OR = 1.088 [0.970–1.221], P = 0.151).
Our meta-analysis showed that the GSTM1 null genotype has a strikingly increased risk in bladder cancer susceptibility, suggesting that carriers of homozygous deletions in GSTM1 lack enzyme activity. Deficiency of the enzyme blocks effective metabolism of compounds involved in carcinogenesis, which may result in an increased risk of somatic mutations, contributing to tumor formation. A statistically significant increase was observed in hospital-based studies, while on the contrary no significance was observed in population-based ones. The data on hospital controls could provide relatively lower risk estimates if the diseases of the controls were associated with the gene variant being studied. Therefore, further studies based on population-design are necessary to confirm the association.
Although several meta-analyses have investigated GSTM1 polymorphism and bladder cancer risk, 49 our study was more stringent and comprehensive. First, more up-to-date studies (33 studies) were recruited to provide statistically significant results. Second, stratified analyses have been performed in detail to investigate the association between the GSTM1 null genotype and bladder cancer risk with different control designs. We suggested that the role of the GSTM1 null genotype on bladder cancer susceptibility was mainly influenced by study design based on different control individuals in this meta-analysis. More importantly, we have explored the biological significance that is valuable for further epidemiological studies.
There are some limitations in this meta-analysis. First, heterogeneity for GSTM1 polymorphism among the studies was extreme. Meta-regression analyses have been conducted used Stata 8.0 to examine the association of methodological and substantive factors with potential sources of heterogeneity, and found that 1.8%, 4.9% and 51.7% variability can be accounted for by publication year, ethnicity and study design, respectively. Therefore, one main reason for heterogeneity is the study design based on different controls in this meta-analysis. We had subgrouped the studies based on study design, but the moderate heterogeneity still existed in hospital-based studies. The one possible reason for heterogeneity may be relatively wide variation in various hospital controls. Second, although the data showed that there was no evidence of publication bias in population-based studies, we found that the impact of a specific study 23 on the result was enormous. Finally, the overall outcomes were based on individual unadjusted OR, while a more precise evaluation should be adjusted by other potentially suspected factors.
In conclusion, our meta-analysis suggested that GSTM1 null status is associated with a high increase in the risk of bladder cancer. Further studies based on population design are necessary to confirm the conclusion on the role of GSTM1 in bladder cancer risk.
Footnotes
ACKNOWLEDGEMENTS
This study was supported by the National Natural Science Foundation of China (No. 30872375).