
Abstract
The mounting evidence for anthropogenic changes in global climate raises many pressing questions about the potential effects on biological systems, and in particular the transmission of infectious diseases. Vector-borne diseases, such as dengue, may be particularly sensitive to both periodic fluctuations and sustained changes in global and local climates, because vector biology and viral replication are temperature- and moisture-dependent. This paper reviews the current state of knowledge on the associations between climate variability, climate change and dengue transmission, and the tools being used to quantify these associations. The underlying causes of dengue's recent global expansion are multifactorial and poorly understood, but climatic factors should be considered within the context of the sociodemographic, economic and immunological determinants that have contributed to dengue's spread. These factors may mediate the direct effects of climate on dengue and many may operate at a very local level. Translating theoretical models of dengue transmission based on historical data into predictive models that can inform public health interventions is a critical next step and efforts should be focused on developing and refining models at smaller spatial scales to characterize the relationships between both climatic and non-climatic factors and dengue risk.
Introduction
Dengue is the most common vector-borne viral disease worldwide, and is ranked among the most important infectious diseases by the World Health Organization (WHO). 1 Dengue poses a major challenge to international public health (World Health Assembly resolution, 2002). The disease burden and geographic range of dengue have expanded over the past 50 years, from approximately 15,000 cases reported annually to WHO from fewer than 10 countries during the 1960s to close to 1 million cases annually across more than 60 countries in 2000–2005. 2 Recent estimates suggest that transmission occurs in up to 124 countries with at least 35 million symptomatic cases per year and around 20,000 deaths, and that approximately 3.5 billion people, or 55% of the world's population, live in countries at risk for dengue. 3 In Vietnam, dengue was first reported in 1959 and since then the number of reported cases has increased steadily, with major outbreaks in 1987 and 1998 throughout all provinces. 4–7 Figure 1 shows the incidence of dengue and the case fatality rate in southern Vietnam since 1996. In endemic areas of southeast Asia, dengue is mainly a childhood disease and children experience an annual exposure risk of ∼10%. 8,9 An upwards shift in the median age of dengue cases has recently been reported from Thailand; 10 however, it is not yet clear whether this is replicated in other endemic settings.
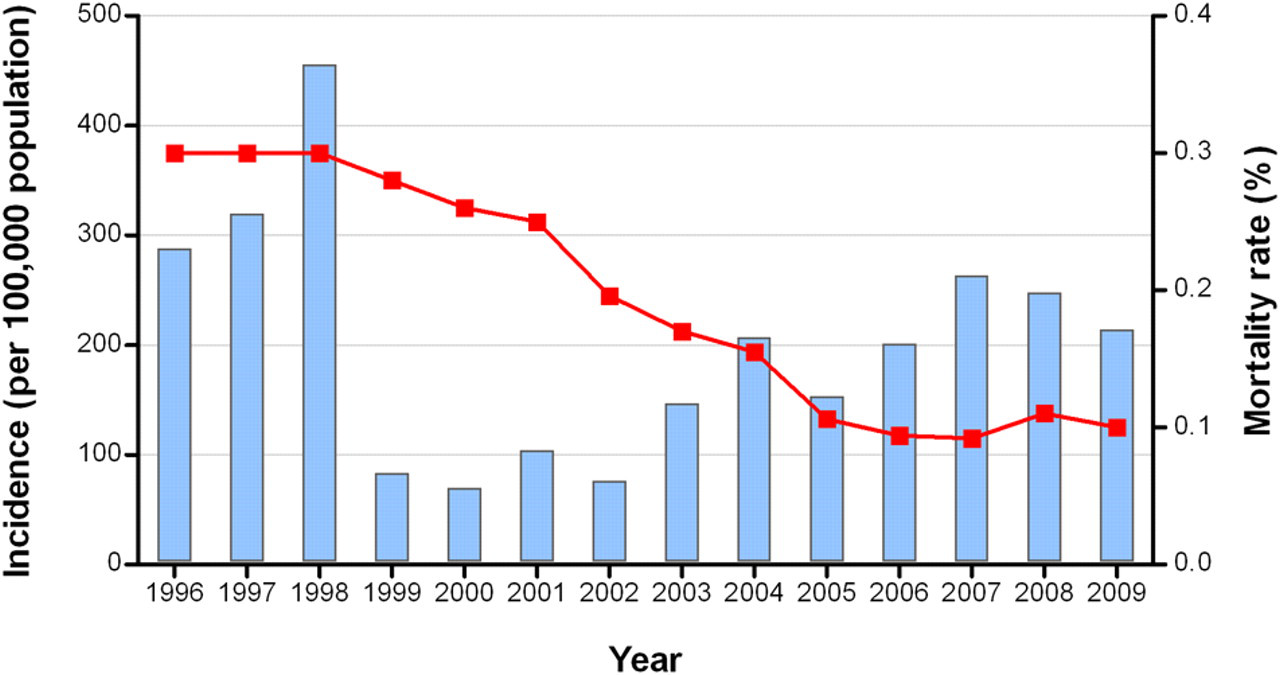
Dengue incidence and mortality in southern Vietnam, 1996–2009. Bars show the incidence of dengue (dengue fever and dengue hemorrhagic fever) per 100,000 population in the southern 20 provinces of Vietnam between 1996 and 2009. The line shows the mortality rate among reported dengue cases over the same period. Data represent cases reported to the national dengue surveillance control program and includes hospitalized cases only. These data are reproduced with the permission of the Pasteur Institute, Ho Chi Minh City
Humans are the primary host of dengue virus (DENV) and transmission of DENV takes place through the bite of the principal mosquito vector Aedes aegypti, and to a lesser degree, Aedes albopictus. Human infection by DENV can lead to a broad spectrum of outcomes. The majority of DENV infections are inapparent (50–90%) 11,12 ; clinical manifestations range from dengue fever (DF), a self-limiting syndrome characterized by fever, malaise, arthralgia and myalgia, to severe disease that has been classically classified into dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS) and is characterized by vascular permeability, coagulopathy and, in the case of DSS, hypovolemic shock. 13,14 Mortality rates vary from less than 1% to 10% in different settings, and depend critically on access to health-care facilities and the degree of clinical experience in hematological monitoring and management of vascular leakage. 15
The geographical distribution of dengue largely reflects the distribution of the principal vector A. aegypti. The expansion in the range and magnitude of the dengue disease burden over the past half-century has paralleled rapid population growth and urbanization, particularly in endemic areas of southeast Asia, and unprecedented increases in global human mobility and trade (reviewed in ref. 16 ). All of these factors are conducive to an intensification of transmission in early endemic settings and the export of DENVs and their vectors from these early foci in southeast Asia and parts of Central America into new areas, as occurred in the decades following the 1950s. In particular, many countries in the Americas experienced a re-emergence of dengue during the 1970s and 1980s after prior success in controlling A. aegypti through concerted campaigns to eliminate yellow fever, which shares the same primary vector. 17
The rapid and continued expansion of dengue represents an increasing challenge to national and regional health authorities, both in endemic settings and in currently unaffected or newly affected areas. The ability to accurately estimate the current disease burden and to predict future trends is key to the planning of effective prevention and control interventions.
Climate is an important determinant of the spatial and temporal distribution of dengue and other vector-borne diseases. 18–22 It seems logical therefore that long-term changes in global climate, for which there is considerable evidence, may have significant effects on the distribution of vector-borne diseases such as dengue. A substantial scientific literature has examined this question over the last two decades; however, there is still inconclusive evidence on what influence, if any, sustained global climate change will have on dengue. The aim of this paper is to review the current knowledge of the relationship between climate variability or climate change and dengue transmission and spread, and to discuss the tools that are being used to explore this relationship. In particular, we aim to highlight the distinction between models that explore climate variability with respect to dengue transmission, and those that aim to model the effects of climate change, as the required input parameters as well as intended outputs of these models are quite distinct. We consider the variable endpoints for models of dengue and climate, which tend to describe and predict either the geographic range or the intensity of dengue transmission, and the differences in how climate and environmental parameters are included to these ends. We further discuss the ways in which non-climatic determinants of dengue transmission may mediate or constrain the predicted effects of climate variability or change on dengue transmission, and the importance where possible of including these sociodemographic–economic factors into models, or at least giving due consideration to their potential influence on model outputs.
Effects of climate on dengue transmission
Climatic conditions play a key role in the biology and ecology of mosquito vectors and the viruses they transmit, and consequently also exert a strong influence on the risk of dengue transmission. 18,23–27 Higher temperatures increase the rate of larval development and therefore emergence of adult vectors, increase the vector biting rate and reduce the time required for virus replication within the vector, known as the extrinsic incubation period, 28,29 meaning vectors are infectious earlier and bite more frequently. Higher temperatures may reduce vector survival time, which may offset the positive effect on vector abundance to some degree. Numerous studies have linked temperature to A. aegypti abundance and dengue incidence rates. 30–33 These studies have used various statistical approaches considering different temperature parameters (e.g. mean, maximum and minimum temperatures).
Aedes vectors breed predominantly in clean water-holding containers in close proximity to human dwellings. 29,34,35 Variability in rainfall is likely to affect the availability of these vector breeding sites, and therefore influence vector abundance; 36 however, the magnitude and direction of this effect is uncertain and may differ between settings depending on the nature of local vector breeding sites, especially whether they are predominantly outdoor rain-filled objects or indoor containers that are filled manually. 37 Humidity, or vapor pressure, is governed by a combination of rainfall and temperature and influences the lifespan of the mosquito and therefore the potential for transmission of the virus. 29 Annual average vapor pressure has been suggested by some authors to be the most important climatic predictor of global dengue occurrence. 38
Temperature, rainfall and humidity are therefore important determinants of the geographic limits within which dengue transmission can be expected to be sustained, primarily through their effects on the survival and proliferation of the Aedes vector. Furthermore, within areas where minimum thresholds of these climate parameters are sufficient to sustain DENV transmission, seasonal fluctuations in these parameters will be important determinants of the duration and potentially the intensity of transmission.
Non-climate determinants of dengue transmission and disease severity
Climatic conditions favorable for Aedes vectors are a necessary but insufficient criterion for DENV transmission to occur and to spread. The availability of susceptible human hosts is determined by local population density and levels of pre-existing immunity, and the presence of the DENV itself is the necessary third component of the transmission cycle.
Infection with any one of the four DENV serotypes is believed to elicit lifelong immunity against that serotype, but confers only partial or transient immunity against the other three serotypes. 13,39 Secondary or subsequent infection with a heterologous virus is a well-established risk factor for severe dengue disease, 11,40–42 a phenomenon that is thought to be mediated by a process of antibody-dependent enhancement (ADE) of DENV infection by cross-reactive non-neutralizing antibodies, resulting in a higher viral burden and an increase in the resultant pathogenic processes. 43,44 Transient cross-protective immunity and ADE may also have implications for dengue transmission at a population level, as they may respectively reduce or increase the effective population of susceptible human hosts. 45–47 Despite the importance of cross-protective immunity for understanding the epidemiological dynamics of dengue, little is known about the duration of cross-protection against a heterologous serotype. It is generally assumed that a first clinical dengue episode elicits cross-protective immunity that lasts 2–9 months, 1,48 although a recent report estimates cross-protection to last as little as 1–2 weeks. 49
There is evidence that the infecting viral serotype, genotype and sequence of infection are also important determinants of disease severity, independent of infection parity. 50–55 This may also influence dengue transmission dynamics if increased inherent virulence results in higher viral titers and increased infectiousness to mosquitoes. Although there is limited direct evidence for this as yet, particular genotypes of DENV serotype 2 (DENV-2) are known to have displaced previously dominant strains in Vietnam, Thailand and Cambodia, suggestive of a difference in viral fitness. 56 Age, 11,15,57,58 host genetic background 59 and the time interval between sequential infections 57 are other factors associated with the risk of developing severe dengue disease.
Finally, factors that influence interactions between the virus, vector and host components of the dengue episystem will be critical in determining the overall effect on the establishment, persistence and intensity of dengue transmission in a given setting. This includes factors that determine the accessibility of vectors to human hosts, such as built environments that create vector breeding sites in close proximity to humans, increases in population density associated with urbanization or the use of window screens and air-conditioning that reduce vector access into human dwellings. As the Aedes vector has a restricted flight range, movement of dengue-infected humans is thought to play a major role in dengue transmission. 60,61 Rabaa et al. 62 have demonstrated substantial DENV viral exchange between the urban center of Ho Chi Minh City and other provinces of southern Vietnam, suggesting that human movement between urban and rural areas may play a central role in the rapid diffusion of DENV across southern Vietnam. Movement and transport of humans or vectors at a national, regional or international scale creates new opportunities for vectors to become established in permissive environments, and for virus transmission to be established where competent vectors exist, and inadequate or interrupted vector control activities determined by economic and political priorities will directly affect individuals' risk of exposure to infection in endemic settings. These social, demographic and economic drivers are thought to be responsible for much of dengue's expansion and intensified transmission over recent decades. 2,16,63
Dengue transmission dynamics and disease modeling
Transmission dynamics
Dengue transmission in endemic settings is characterized by non-linear dynamics, with strong seasonality, multiannual oscillations and non-stationary temporal variations (i.e. irregular temporal fluctuations in incidence). 64 Seasonal and multiannual cycles in dengue incidence vary over time and space. 65 Besides the seasonality of dengue transmission, periodic epidemics and more irregular intervals of outbreaks are commonly observed. Mathematical models of dengue transmission aim to quantify the relative contributions of viral, host, vector and ecological factors to these observed cyclic dynamics; however, this is complicated due to the presence of multiple inter-related environmental, biological and sociodemographic determinants, as discussed above. Alternatively, models may have as an endpoint the occurrence of disease as a qualitative (yes/no) measure, rather than a quantitative measure of incidence, with the aim of defining climatic, environmental or other ecological variables that correlate with the spatial distribution of disease. Mathematical modeling of infectious disease dynamics has two related main objectives: firstly to provide insights into the underlying biological and ecological mechanisms that give rise to the dynamics observed historically and currently, and secondly to make predictions about the future magnitude, timing and/or location of disease transmission.
Seasonal and interannual climate variability is thought to be an important determinant of dengue epidemic cycles. 38,66 Numerous studies have examined the wave-like behavior of dengue transmission in different areas and have demonstrated various associations between dengue incidence and climate variables (Table 1). 19,22,65,67–74 Table 1 summarizes published studies examining the relationship between extreme climatic events and dengue incidence time series. In particular, periodic dengue epidemics with multiannual cycles appear to be associated with extreme weather events, and the El Niño Southern Oscillation (ENSO) has been suggested as a major indicator. 66 The ENSO is a natural climate fluctuation and is probably the best understood systematic pattern of global climate variability. It affects rapid climatic changes in most countries bordering on or in the Pacific and Indian oceans. It is characterized by variations in the surface temperature of the tropical eastern Pacific Ocean, which consists of the warm El Niño event and the cold La Niña event. El Niño and La Niña events occur irregularly every 2–7 years and last for 12–18 months. 75 Other indices for the quantification of ENSO events are the Southern Oscillation index which compares the atmospheric pressure between Tahiti and Darwin, Australia, and the multivariate ENSO index which combines the six main observed variables over the tropical Pacific.
Summary of published studies examining the relationship between extreme climatic events and dengue incidence in time series
ARIMA, autoregressive integrated moving average; ENSO, El Niño Southern Oscillation; SOI, Southern Oscillation Index; SST, sea surface temperature
Tools for modeling dengue transmission dynamics
Traditionally, Fourier analysis has been used to analyze relationships between oscillating time series. This technique decomposes time series into their different periodic components that can then be compared between time series. Since Fourier analysis cannot take into account temporal changes in the periodic behavior of time series (i.e. their lack of stationarity), this method, and others such as generalized linear models, may be inadequate for investigating the determinants of dengue transmission dynamics. Wavelet analysis is suitable for investigating time series data from non-stationary systems and for inferring associations between such systems. 76 This approach reveals how the different scales (i.e. the periodic components) of the time series change over time. Wavelet analysis is able to measure associations (coherency) between two time series at any frequency (period) band and at every time-window period.
Wavelet coherency analyses have been used to compare time series of disease incidence across localities and countries for the characterization of the evolution of epidemic periodicity and the identification of synchrony. Wavelet analyses have been used in analyzing various human infectious disease dynamics such as measles, influenza, leishmaniasis and dengue. 65,71,77–80
Although annual periodic patterns are a common phenomenon in dengue endemic areas, the identification of a periodic multiannual (e.g. 2–3 years) cycle differs between countries and in analyses used. Cazelles et al. 65 used wavelet approaches to demonstrate a highly significant but discontinuous association between ENSO, precipitation and dengue epidemics in Thailand. Johansson et al. investigated the relationship between ENSO, local weather and dengue incidence in Puerto Rico, Thailand and Mexico since the mid-1980s with an annual scale and multiyear cycles. Temperature, rainfall and dengue incidence were strongly associated in all three countries for the annual cycle. The associations with ENSO varied between countries in the multiannual cycle. ENSO was associated with dengue incidence in Puerto Rico, but characterized with non-stationarity while there was no association in Mexico. In Thailand, ENSO was associated with climate and dengue incidence. 71 Thai et al. provided insights into dengue transmission dynamics in Binh Thuan province, southern Vietnam, between 1996 and 2009. A continuous annual mode of oscillation with a non-stationary 2–3-year multiannual cycle was observed (Figure 2a) with strong irregular associations between dengue incidence and ENSO indices and climate variables (Figure 2b). The dengue incidence time series for Phan Thiet City and eight neighboring districts within Binh Thuan province are shown in Figure 2c. Figure 2d shows the coherency between these two time series, which demonstrates high coherence in the annual periodic band and in the 2–3-year periodic band between 1996 and 2001. In addition, the spatio-temporal patterns seem to be different between the annual and multiannual cycle. 73
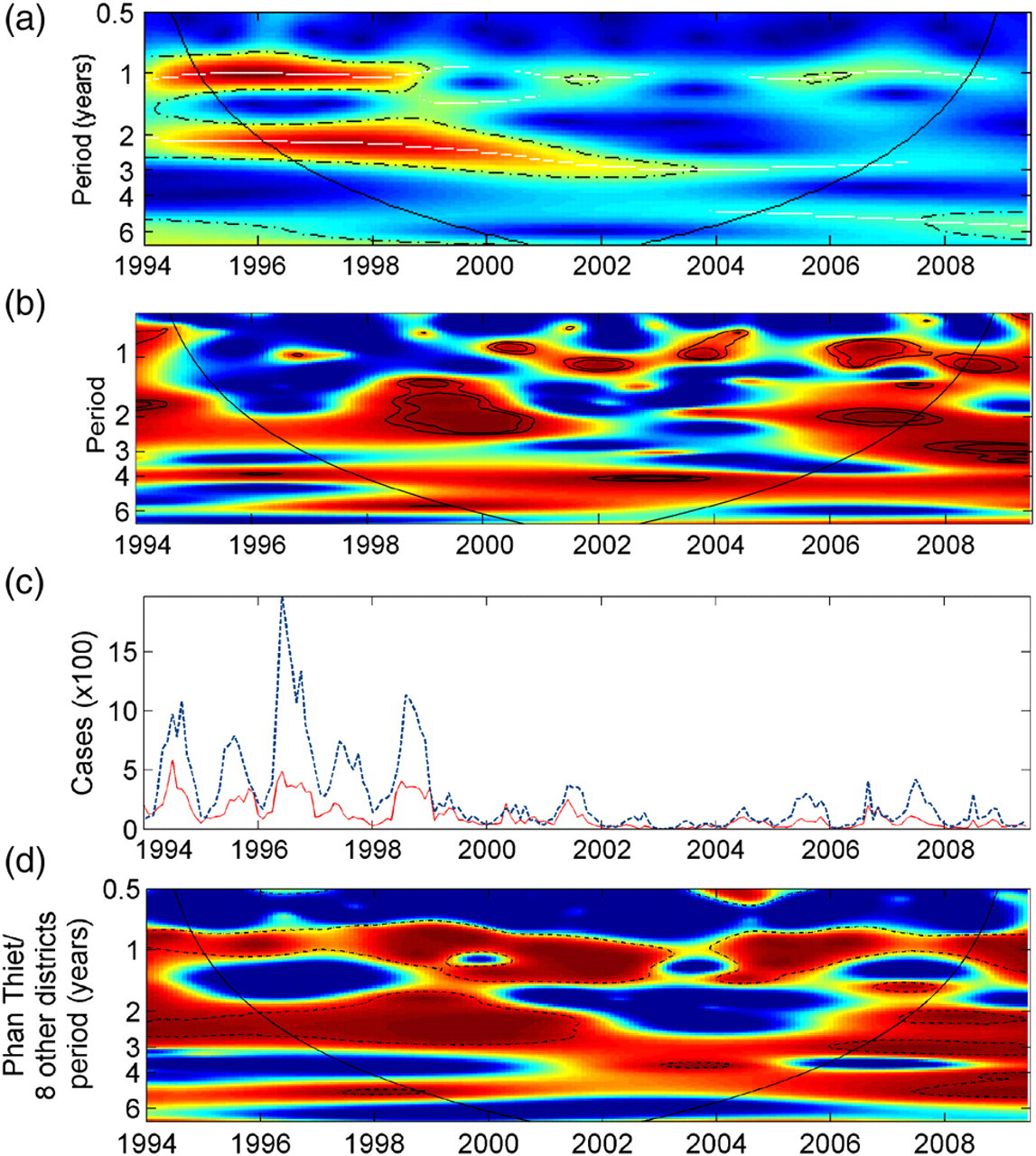
Wavelet analysis and wavelet coherency analysis with dengue incidence time series and with an El Niño Southern Oscillation (ENSO) index in Binh Thuan province, Southern Vietnam. (a) Wavelet analysis of the dengue incidence time series with monthly data. Color scheme shows increasing intensity, from blue to red; dotted lines show statistically significant area; the black curve delimits the cone of influence. (b) Wavelet coherence analysis of the dengue incidence time series with the ENSO index NIÑO 4. Dark blue and dark red indicates low coherence and high coherence, respectively. The dotted lines show α = 5% and 10% significance levels. The cone of influence (black curve) indicates the region not influenced by edge effects. (c) Time series of dengue incidence in Phan Thiet City (solid red line) and the eight neighboring districts combined (dotted blue line). (d) Wavelet coherence analysis of time series in panel (c) showing a continuous annual mode of oscillation with a non-stationary 2–3 year multiannual cycle. Dark blue indicates low coherence and dark red indicates high coherence. The dotted-dashed lines show α = 5% significance levels computed based on 1000 bootstrapped series. The cone of influence (black curve) indicates the region not influenced by edge effects. This figure has been published previously73 and is reproduced with the permission of the authors
Limitations and considerations in modeling dengue transmission
Although these wavelet analyses have provided important insights into the cyclical dynamics of dengue transmission, the associations found with ENSO have been irregular and transient, which reduces the potential for generating future predictions based on these climatic events. Furthermore, these analyses have tended to examine the association between climate variability and dengue incidence in isolation from other parameters likely to be relevant to the transmission dynamics of dengue, such as the host immune landscape and virus population dynamics. In contrast, others have modeled dengue incidence time series based on parameters related to host immune and viral factors, such as temporary cross-protective immunity, temporary ADE and variations in virus serotype virulence, 46 ADE alone, 45,81 or varying degrees of cross-protective immunity, 82 and have been able to reproduce the observed cyclical incidence trends and serotype oscillations based on assumptions around these parameters, in the absence of climate variability. Because climate, host immunity and viral factors are all likely to impact upon dengue transmission dynamics in a given setting, the interactions between, as well as independent effects of, these intrinsic (host and virus) and extrinsic (climate and environment) factors need further exploration in transmission models.
Aside from their contribution to a fundamental understanding of dengue cyclical dynamics, the public health relevance of transmission models lies in their potential to permit prediction of disease trends and therefore inform intervention. In Taiwan, the occurrence of local epidemics has been shown to be associated with imported dengue cases within a context of favorable meteorological conditions of higher temperature and lower rainfall and humidity, which may inform prospective assessments of the risk of local transmission following the identification of an imported dengue case. 83 To date, there are few publications on the development and application of predictive models for dengue; however, climate and environmental variables have been used to build risk assessment models for other vector-borne diseases such as Rift Valley fever, and to enact public health interventions on the basis of their predictions. 84
The spatial scale of analysis is important when modeling the impact of various factors on dengue transmission. This is because dengue may be sensitive to differences in climatic, environmental, societal and demographic characteristics that occur at a local level, and the relative contribution of these factors may differ between settings. Even when considering more macro-climatic events such as ENSO, the spatial resolution of the dengue incidence data is important. Cummings et al. 85 have demonstrated a spatiotemporal wave in the three-year dengue incidence cycle in Thailand, with each wave originating in Bangkok and radiating out to the provinces, which experience a lag in the peak incidence of up to 10 months. In contrast, our preliminary analysis of dengue surveillance data from southern Vietnam suggests that the annual peak incidence in Ho Chi Minh City occurs consistently at a two-month lag after the peak incidence in the other 19 southern provinces combined. Such spatiotemporal observations may prove useful in informing risk assessments used by local or national dengue control programs to prepare for and respond to annual dengue epidemics in endemic settings, if consistent patterns can be identified in the spatial and temporal relationships between incidence trends in neighboring geographic areas. This is particularly so if environmental or sociodemographic patterns to explain these relationships can be elucidated, providing potential targets for enhanced surveillance or interventions to prevent spread of the epidemic.
Climate change and dengue
Evidence for a changing climate
The world climate is in a warming phase that began in the 18th century. The average temperature in southeast Asia has increased between 0.1 and 0.3°C per decade between 1951 and 2000 86 and the average temperature will further increase by up to 2–4°C by 2100, according to projections of the Intergovermental Panel on Climate Change (IPCC). 87,88 In particular, minimum temperatures have been rising faster than maximum or average temperatures. Changes in rainfall patterns have been geographically inconsistent, with some areas becoming wetter and others drier. 89 Climate change represents these sustained changes in the mean state of the climate or in its variability, as compared with climate variability which encompasses seasonal and multiannual fluctuations in temperature, rainfall and humidity.
Modeling the effect of climate change on dengue
The innate sensitivity of vector-borne diseases, including dengue, to climatic conditions raises the question as to what effect, if any, we might expect sustained increases in temperature and variable changes in rainfall to have on the global disease burden. Again, two separate but related endpoints need to be considered: the geographic range of transmission and the intensity and/or seasonality of transmission. Hales et al. 38 modeled the global geographic range of dengue during the period 1975–1996 in relation to monthly averages of rainfall, vapor pressure (humidity) and maximum, minimum and mean temperatures, aggregated within each of 2000 cells that made up a grid covering the global land surface. Interestingly, annual average humidity was found to be the most important individual predictor of dengue distribution, and an estimated 30% of the global population (1.5 billion) were calculated to be at risk of dengue in 1990. On the basis of this finding and projected increases in population, the authors estimated that 34% of the world's population (3.2 billion) will be at risk of dengue in 2055 if humidity remains at baseline values, compared with 44% (4.1 billion) if changes in humidity occur as predicted by the IPCC. In contrast, more recent estimates of the current extent of dengue transmission, based on a review of published reports of dengue incidence, outbreaks, serosurveys and confirmed cases in travelers, suggest that up to 55% of the world's population are already living in areas at risk of dengue during the first decade of the 21st century. 3 Others have used a model based on a calculation of temperature-dependent vectorial capacity to estimate the effect of global temperature increases on dengue distribution and transmission intensity. 90 This analysis indicated an expansion in the geographic range of dengue, to wider latitudes and higher altitudes, as well as an increased duration of the transmission season and higher transmission intensity in already affected areas. The largest effect of climate change on dengue transmission was expected where A. aegypti populations are already established but where virus replication is currently limited by the temperature.
Mediating factors in the effect of climate change on disease
These models describe the geographic and seasonal range which can be expected to sustain dengue, but do not account for factors that will determine how disease potential relates to disease occurrence. They also consider only the direct effects of climate change, and not indirect effects of climate change on sociodemographics, land use, changes in mode of urbanization (e.g. town planning) or other factors that may mitigate or exacerbate the direct effects of climate on vector-borne disease. There is little published evidence indicating a direct effect of climate change on the increased distribution and magnitude of dengue transmission, and the Aedes vectors, seen over the past decades. Rather, this global resurgence has been attributed to rapid population growth and urban expansion in endemic areas of southeast Asia, coincident with unprecedented connectedness between these areas and the rest of the world through trade and human movement. In the Americas, the re-establishment of A. aegypti since the 1970s, following transnational efforts to eradicate the vector, can be attributed to declining political and financial commitment to resource-intensive control efforts rather than any change in ecological suitability. 63 Similarly, the introduction of the secondary vector A. albopictus to North America, with subsequent spread to Central and South America, is thought to have occurred through shipments of used tires from Japan. 91 More recently, the A. albopictus mosquitoes were introduced into the Netherlands through the import of the ornamental plant Lucky bamboo (Dracaena sanderiana). 92,93 To date, locally acquired DENV infections in non-endemic areas have been reported in Key West, FL, USA and Nice, France. 94,95 Although models have suggested that the vector can survive in the Netherlands, DENV transmission has not been demonstrated. 96 Given this central role for demographic, economic and political influences in dengue's recent resurgence, it seems reasonable to assume that these factors will continue to play a role in shaping the future burden and distribution of disease, and that any climate-related changes will not act independently of these factors.
Factors that will shape how changes in disease potential correspond to changes in actual disease occurrence include: the presence or introduction of the Aedes vector; availability of vector breeding sites; vector control activities; the circulation of one or more DENV serotypes; population demographics – in particular population density and movement; and the degree of contact between humans and vectors, which is influenced for example by housing design, availability of air-conditioning and the use of window and door screens. Many of these things may in fact be influenced by climate change indirectly. For example, changes in precipitation or rising inland water levels in endemic countries could potentially result in changed land use patterns, domestic or international migration and urbanization, all of which have implications for the risk of exposure of susceptible humans to infectious mosquitoes. Therefore, when evaluating the likely impact of climate changes on dengue transmission, both direct and indirect effects should be considered.
Again, the spatial scale of analysis is paramount. At a global scale, climate-based models may be useful in indicating the broad geographic areas in which Aedes vectors, and potentially dengue transmission, could conceivably be sustained at present or in the future. However, the relative effects of climate versus the range of non-climatic factors discussed above on the risk of dengue transmission are certain to depend on the local context. It has been demonstrated both in theoretical models at a global scale 97 and in analysis of empirical data at a national level 30 that local climate characteristics mediate the strength of association between climate variability and Aedes abundance or dengue incidence. These analyses showed a weaker association between monthly variations in temperature or precipitation and monthly variations in Aedes abundance or dengue cases in places with overall higher average temperatures or precipitation, respectively. This demonstrates that the rate-limiting factors determining vector abundance and dengue incidence are likely to be locally defined. In an endemic setting such as southern Vietnam where current climatic conditions are already supportive of near year-round vector development and survival and virus replication, how big an effect is a sustained increase in temperature likely to have in a context of high population immunity and considering a potential life-shortening effect of higher temperatures on mosquito survival? Conditions that may mediate climate-related changes to vector density and disease incidence are also likely to operate at a local level, such as vector-control activities, water storage practices and characteristics of the built environment that determine micro-climates and the availability of breeding sites.
Impact of changes in dengue transmission range and intensity on clinical outcomes
Changes in the geographic distribution or intensity of dengue transmission will have implications for the clinical manifestation of disease. Two key risk factors for both symptomatic and severe dengue disease are the age at infection and the acquisition of secondary infections. Children with DENV infections are less likely than adults to experience clinical disease, 98–100 but are also less able to compensate for the increased vascular permeability that is characteristic of dengue pathogenesis, so are at higher risk than adults of severe outcomes including severe vascular leakage and hypovolemic shock (DSS). 58,100,101 In sporadic dengue epidemics in Cuba and Taiwan, clinical cases were more common in adults than children, 57,102–104 and in Singapore, where successful vector control has greatly reduced the force of infection and therefore the population immunity, adult cases of DF represent the majority of clinical disease. 105,106 In contrast, in the dengue endemic countries of southeast Asia and Central America, dengue is primarily a disease of children and young adults, and by adulthood most individuals have partial or full immunity from multiple DENV exposures. 8,11,107,108 Repeated introductions of DENV to a non-endemic area have the potential to lead to sequential epidemics with heterologous DENV strains, with the associated increase in the risk of DHF. An increased force of infection in endemic settings where multiple serotypes circulate could be expected to reduce the time between sequential infections, leading to a shift in the age distribution of disease towards younger age groups and potentially increasing the incidence of DHF/DSS in very young children. A recent analysis of hospitalized dengue patients in Ho Chi Minh City from 1996–2009 demonstrated that the highest risk of DSS was in pediatric dengue patients aged 6–10 years, but the youngest children (≤5 years) were at significantly higher risk of mortality than older children. 109 Efforts to model the epidemiology of dengue based on trends in climate, environmental and other factors should therefore consider also the implications of alterations in force of infection and the likelihood of sequential or co-circulation of heterologous serotypes on the age distribution of disease and therefore the clinical spectrum of dengue.
Further issues
Evaluating the effect of climate or other factors on the current or future dengue disease burden requires defined indicators of disease or infection. The most obvious indicator is clinical disease; however, for dengue, perhaps more so than for many other infectious diseases of global importance, this is complicated in a number of ways. Firstly, national and international surveillance efforts for dengue generally rely on passively reported notifications of hospitalized cases, and therefore do not capture the full disease burden, with the ascertainment gap subject to considerable variation between settings and in time. Hospital-based data also carries inherent issues with determining the appropriate denominator for calculating burden of disease. Furthermore, dengue encompasses a spectrum of severities that may be variably included in the case definition for reporting. At the same time, surveillance in most endemic settings is based only on a clinical diagnosis with only a small proportion of cases undergoing laboratory diagnostic testing; therefore, over-reporting is an issue of variable magnitude within and between countries and over time. Furthermore, the quantitative relationship between clinical cases and total infections will vary substantially between epidemiological settings, depending on the intensity of transmission, age distribution of cases, population immunity and identity of circulating viruses. Indicators of vector abundance (i.e. house index, container index and Breteau index of pupae and larvae) have often been used as proxy measures for dengue risk, but their correlation with human disease is often poor 110,111 and is likely to depend on local ecological and demographic characteristics. The lack of a robust and standardized indicator for dengue disease burden complicates efforts to predict and monitor future trends in dengue range and endemicity, which will rely on comparisons with a baseline, as well as models examining spatial patterns in dengue transmission, which may be confounded by geographic differences in clinical case ascertainment. Extensive work has been done to describe the geographic range and endemicity of malaria worldwide, using Plasmodium parasite prevalence as the index of endemicity. 112,113 The existence of numerous published and unpublished parasite prevalence surveys from many locations and over a substantial time period made spatial and temporal comparisons of malaria endemicity valid and logistically feasible. An equivalent population-based virological marker for dengue burden is less obvious. Standard serological surveys give an indication of lifetime exposure risk, but must include a large age-stratified sample in order to be informative about historic and current transmission intensity. Serological markers of acute or recent DENV infection represent a more promising candidate for population-based assessments of dengue transmission risk.
We have discussed the limitations of transmission models or risk assessments that consider the climatic or immunological influences on dengue transmission in isolation from the multifactorial environmental, social and demographic determinants that are accepted to have contributed to dengue's recent resurgence. However, one explanation for the absence of these variables from models may be the difficulty in obtaining time series for sociodemographic and environmental factors that are comparable in time and geography to the case burden and climatic time series. Greater interdisciplinary collaboration between the ecology, social science and biomedical science fields would facilitate the incorporation of longitudinal data on relevant covariates as far as those data are available, or would at least allow for model findings to be considered within a broader environmental, social and demographic context.
Conclusions
Dengue, like all vector-borne diseases, is sensitive to climatic conditions that shape virus replication, vector development and survival, and therefore help define the geographical and seasonal limits that can support DENV transmission. Climatic factors do not, however, act in isolation, and non-climatic variables including population growth, human movement and environmental changes may have had far more to do with the global resurgence in dengue witnessed over recent decades than any direct effects of climate. The influences of climatic and non-climatic determinants on current and future dengue transmission are difficult to disentangle and therefore to quantitate independently. The challenge in refining models of dengue transmission to maximize their utility in predicting the location, magnitude and timing of future dengue epidemics or multiannual peaks in endemic cycles is to use data at appropriate spatial scales so that relevant ecological, social and demographic variables that operate at a local or regional scale can be incorporated into the model.
Footnotes
ACKNOWLEDGEMENTS
We are grateful to Jeremy Farrar, Cameron P Simmons, Maciej F Boni and H Rogier van Doorn for critically reading the manuscript. This work was supported by the Wellcome Trust. KTDT is supported by a ‘Mosaic’ fellowship from the Netherlands Organization for Scientific Research (NWO). The sponsors of the study had no role in this report.