
Abstract
Different routes for the administration of bone marrow-derived cells (BMDC) have been proposed to treat the progression of chronic renal failure (CRF). We investigated whether (1) the use of bovine pericardium (BP) as a scaffold for cell therapy would retard the progression of CRF and (2) the efficacy of cell therapy differently impacts distinct degrees of CRF. We used 2/3 and 5/6 models of renal mass reduction to simulate different stages of chronicity. Treatments consisted of BP seeded with either mesenchymal or mononuclear cells implanted in the parenchyma of remnant kidney. Renal function and proteinuria were measured at days 45 and 90 after cell implantation. BMDC treatment reduced glomerulosclerosis, interstitial fibrosis and lymphocytic infiltration. Immunohistochemistry showed decreased macrophage accumulation, proliferative activity and the expression of fibronectin and α-smooth muscle-actin. Our results demonstrate: (1) biomaterial combined with BMDC did retard the progression of experimental CRF; (2) cellular therapy stabilized serum creatinine (sCr), improved creatinine clearance and 1/sCr slope when administered during the less severe stages of CRF; (3) treatment with combined therapy decreased glomerulosclerosis, fibrosis and the expression of fibrogenic molecules; and (4) biomaterials seeded with BMDC can be an alternative route of cellular therapy.
Introduction
The progressive deterioration observed in chronic renal disease is caused by a series of inflammatory events leading to glomerulosclerosis, interstitial cell infiltration, tubular atrophy, activation of fibroblasts, scar formation or fibrosis. 1
Since the process of renal repair depends on the severity and extent of kidney injury and the number of resident stem cells, the recent development in cell-based therapies aiming to restore or replace chronically injured tissues may bring hope for the treatment of many chronic diseases. 2,3
However, there is a paucity of reports using bone marrow-derived cells (BMDC) as a regenerative therapy for chronic renal failure (CRF). Comparisons among the results are therefore jeopardized by study differences such as the use of different models of renal damage, the amount of administered cells and differences in the routes of cell administration. 4–9
Generally, 5/6 nephrectomized rats are used as a model to mimic human CRF in the majority of published papers because the procedure causes a significant reduction in nephron number, resulting in severe CRF. 10,11 We reasoned that with the reduction of a large amount of renal mass, the regenerative capacity of the organ could be compromised; this fact would impact the result of cell therapy. 12 To address this issue, we investigated the effect of treatment with BMDC on a 2/3 nephrectomized rat (CRF2/3) with less renal damage and a lesser degree of CRF, in addition to the usual 5/6 model (CRF5/6).
In this study, we also introduced a basic concept of tissue engineering that includes the use of a scaffold to provide an architecture upon which seeded cells can organize and develop to promote tissue repair. 13 Using this combination as opposed to traditional methods of cell administration, we could evaluate whether a biomaterial seeded with BMDC could be an alternative route for cell therapy.
Considering that in both models of renal mass reduction, chronic deterioration of the remnant kidney is due to the participation of cellular and inflammatory mechanisms that lead to fibrosis, we hypothesized that BMDC treatment would reduce the inflammatory activity and expression of profibrotic molecules and fibrosis.
In the present report, we sought to evaluate whether (1) biomaterial seeded with mesenchymal stem cells (BPMSC) or mononuclear cells (BPMO) could retard the progression of experimental CRF; (2) the amount of remnant renal mass would impact the efficacy of cell therapy; (3) the expression of profibrotic molecules would be affected by BMDC treatment; and (4) biomaterial combined with BMDC could be an alternative route of cellular therapy.
Materials and methods
Animal models
Animal procedures were performed in accordance with protocols approved by the Institutional Animal Care and Use Committee (No. 3310/2008). Female Wistar rats weighing 250–350 g that underwent a reduction of 5/6 or 2/3 renal mass reduction were used for this study. All animals were provided standard rat chow and water ad libitum.
CRF models
The 5/6 renal mass reduction procedure was performed as previously described to experimentally induce severe CRF. 14 To create a less severe CRF model, we reduced the renal mass by only 2/3. Briefly, female rats were administered anesthesia in the form of ketamine hydrochloride (50 mg/kg) and xylazine (10 mg/kg). Infarction of approximately one-third of the left kidney was performed by microsurgical ligation of one branch of the left renal artery, followed by right nephrectomy.
Experimental groups
Animals (n = 45) were divided into groups according to the amount of renal mass reduction and the severity of CRF (2/3 and 5/6 models). They were further subdivided according to treatment received: (1) sham (S, n = 5); (2) animals with 2/3 or 5/6 mass reduction alone (CRF2/3, n = 5 or CRF5/6, n = 5); (3) animals implanted with bovine pericardium (BP) alone (CRF2/3 + BP, n = 5 or CRF5/6 + BP, n = 5); (4) animals treated with BP seeded with mesenchymal stem cells (BPMSC2/3, n = 5 or BPMSC5/6, n= 5); and (5) animals treated with BP seeded with mononuclear cells (BPMO2/3, n = 5 or BPMO5/6, n = 5). Renal function was assessed by measurements of serum creatinine (sCr), creatinine clearance (Clcr), and 24-h proteinuria (PT-24 h) at the baseline, at 45 and 90 d after surgery. Progression of CRF was measured by the 1/sCr slopes and decline in the Clcr rate (mL/min/d). At the end of 90 d, the animals were weighed and sacrificed.
Isolation and characterization of BMDC
BMDC were isolated from the femur and tibia of male Wistar rats. Mononuclear cells (MO) were separated by Ficoll-Hypaque (d = 1.077) density gradient centrifugation and cultured in Dulbecco's modified Eagle's medium (Gibco, Invitrogen Co, New York, NY, USA), 20% fetal bovine serum (Cultilab, Campinas, Brazil) and penicillin/streptomycin (Invitrogen, Carlsbad, CA, USA) for 14 d. Mesenchymal stem cells (MSC) were recovered using their tendency to adhere to plastic; non-adherent cells were removed by washing. Flow cytometry analyses (FACSCanto, Becton Dickinson, San Jose, CA, USA) were performed with antibodies for the cell-surface markers CD31, CD44, CD90, CD45 and CD34 (Caltag Laboratories, Carlsbad, CA, USA) kindly provided by Dr Irene Noronha. Cell differentiation potential was tested by adipogenic and osteogenic differentiation as previously described. 15
Preparation of acellular BP
BP was prepared by the Biomaterials Group of the Chemical Institute of Sao Carlos – University of Sao Paulo. Briefly, fresh BP to be used as a collagen source was treated at 20°C for periods of 0–48 h with an alkaline solution (3 mL/g of tissue) containing 6 vol% of dimethyl sulfoxide, salts (chlorides and sulfate) and bases of alkaline (K+, 1.19 mol/L, and Na+, 1.74 mol/L), and alkaline earth metals (Ca2+, 0.86 mol/L). The resulting materials were equilibrated with a solution containing Na2SO4, NaCl, KCl and CaSO4 (6 mL of solution/g of tissue) for a period of 12 h, and the excess salts were removed by washes with the following solutions: 3% w/w of boric acid solution (3 × 2 h, 250 mL), deionized water (3 × 6 h, 250 mL), 0.3% w/w ethylenediamine tetraacetic acid (EDTA) solution (3 × 2 h, 150 mL), pH 11.0 and (6 × 2 h, 250 mL) washes with deionized water.
The resulting material is basically acellular polyanionic collagen matrices associated with an elastin content and triple helical structure. Previous studies showed that the biomaterial used is biocompatible, causing only mild and progressive chronic inflammation. 16,17
MSC and MO seeding in BP
After rehydration in phosphate-buffered saline (PBS), 0.5 × 0.5 cm segments of BP were placed in six-well Petri dishes and MSC resuspended at a concentration of 2.5 × 106 cells/mL were seeded onto the BP. The plates were kept in a humidified 5% CO2 incubator at 37°C during 14 d of culture. After this period, the segments of BPMSC were fixed in 10% phosphate-buffered formalin and samples were subjected to histological evaluation after embedding in paraffin and stained with hematoxylin and eosin (H&E) and Giemsa (Gibco, Invitrogen Co., New York, NY, USA) (Figures 1a and b). BP was seeded with MO at a concentration of 5 × 106 cells/mL 3 h before implantation.
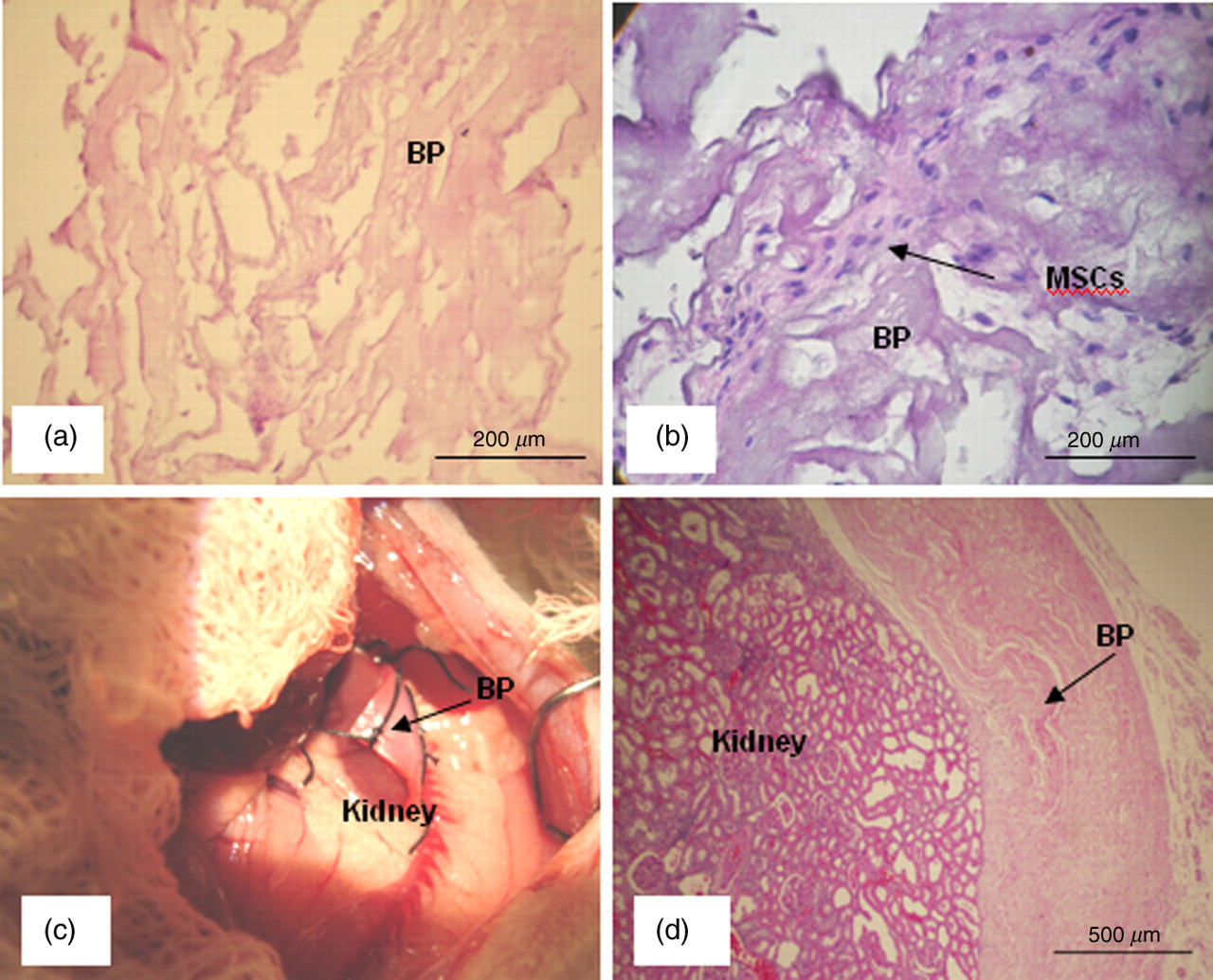
(a and b) Hematoxylin/eosin staining of unseeded or MSC-seeded collagen scaffolds cultured for 14 d in culture medium. (c) Photograph of biomaterial adhered to renal parenchyma after renal mass reduction surgery. (d) Histological appearance of the biomaterial attached to renal parenchyma at 90 d postsurgery. Bars = 100 μm. BP, bovine pericardium; MSC, mesenchymal stem cells (A color version of this figure is available in the online journal)
Implantation of BP in renal tissue
Immediately after renal mass reduction surgery, the renal capsule was removed from the interface region of renal infarction/healthy and segments of biomaterial alone (BP) or seeded with BPMSC or BPMO were sutured with 8.0 mononylon adjacent to the renal surface (Figures 1c and d).
Histological and immunohistochemical analysis
Sections (3-μm) of renal tissue were stained with H&E and methenamine silver (PAMS) for histological analysis. A semi-quantitative evaluation based on percentages was performed by two blinded renal pathologists (+1 = <25% damage, +2 = 25–50% damage, +3 = 51–75% damage, +4 = >75%).
The criteria for the semi-quantitative analysis were used for the following histopathological indicators: glomerulosclerosis (GS), tubular atrophy (TA), interstitial fibrosis (IF) and interstitial lymphocytic infiltration (IL). 18
Immunohistochemical analysis was performed as previously described. 19 Briefly, the sections were incubated with the anti-α-smooth muscle (SM)-actin (Dako, Glostrup, Denmark), antifibronectin (Chemicon International, Temecula, CA, USA) or anti-Jun-N-terminal kinase (p-JNK; Santa Cruz Biotechnology, Santa Cruz, CA, USA) antibody at 4°C, or the anti-proliferating cell nuclear antigen (PCNA) (Sigma, St Louis, MO, USA) or anti-ED1 antibody at room temperature for 30 min. The reaction product was detected with an avidin–biotin–peroxidase complex (Vector Laboratories, Burlingame, CA, USA). The material was counterstained with methyl green, dehydrated and mounted. Counterstaining of the p-JNK slides was performed with Harris hematoxylin. Non-specific protein binding was blocked by incubation with 20% goat serum in PBS for 20 min. Negative controls consisted of replacement of the primary antibody with normal rabbit IgG and mouse IgG for the polyclonal and monoclonal antibodies, respectively, at equivalent concentrations.
Each grid field was semi-quantitatively graded, and the mean score per kidney was calculated to evaluate the immunoperoxidase staining of fibronectin and α-SM-actin. Each score mainly reflected changes in the extent rather than the intensity of staining and depended on the percentage of the grid field showing positive staining: 0 = absent or less than 5%; I = 5–25%; II = 25–50%; III = 50–75%; IV > 75%.
The number of ED1-positive (macrophage cells) and PCNA-positive cells in each section was calculated by counting the number of positive cells in 30 sequential (0.245 mm2) grid fields from the renal cortex. 19
Statistical analysis
Data were expressed as mean ± standard deviation. Analyses were performed using GraphPad Prism software (San Diego, CA, USA), with the critical level set at P < 0.05. Comparisons among multiple groups were made using analyses of variance (ANOVA). When F values were significant, differences between the groups were specified with Tukey's multiple comparison post-tests. When comparing data, a two-sided Student's t-test and Mann-Whitney U test were performed.
Results
Functional studies
Comparing severity of the CRF2/3 and 5/6 models
As expected, the 2/3 nephrectomized rats presented a pattern of less severe CRF when compared with the 5/6 mass reduction model. This result was demonstrated by the significantly lower increase in sCr level observed at day 90 in CRF2/3 animals compared with CRF5/6 rats (CRF2/3 = 48.2% versus CRF5/6 = 128%; P = 0.006). Interestingly, the 5/6 but not 2/3 nephrectomized rats treated with unseeded BP showed the greatest increases in sCr after 90 d, suggesting a worsening of chronic inflammation. In addition, progression of disease as measured by the slope of 1/sCr was significantly slower in the CRF2/3 model (CRF2/3 = −0.24 ± 0.03 versus CRF5/6 = −0.49 ± 0.04; P = 0.008), demonstrating a lesser degree of chronic deterioration in these animals.
Effects of treatment in the CRF2/3 model
After 90 d, the increase in sCr level in CRF2/3 rats treated with BPMSC was blocked in a way similar to that of rats in the Sham group (S = 5.2% versus BPMSC = 7.6%; P = NS), while sCr in untreated CRF2/3 animals continued to rise (CRF2/3 = 48.2% versus BPMSC = 7.6%; P < 0.05) (Figure 2a). In this model, the greatest effect of treatment was evident after day 45, when the use of BPMSC and BPMO stabilized the increase in sCr (CRF2/3 versus BPMSC and BPMO, P < 0.05; BP versus BPMSC and BPMO, P < 0.001) (Figure 2a).
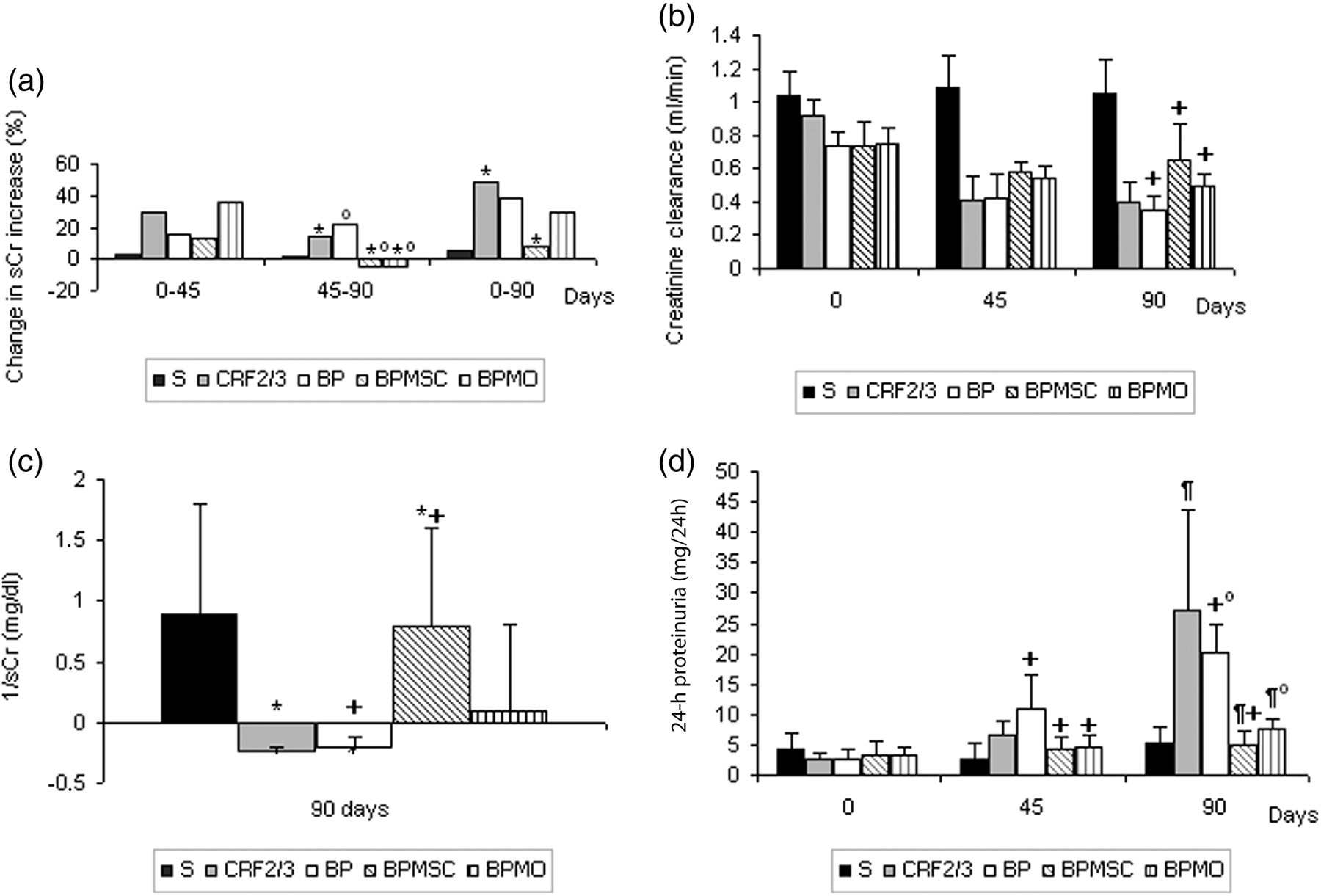
Renal function studies at days 0, 45 and 90 in the 2/3 renal mass reduction model. (a) Percentage increase in sCr, (b) creatinine clearance, (c) slopes of the reciprocal serum creatinine plot (1/sCr), (d) 24-h proteinuria (PT-24 h). Values are expressed as means ± SD in b, c and d (*P < 0.05, °P < 0.05, + P < 0.01, ¶ P < 0.01). sCr, serum creatinine; S, sham; CRF, chronic renal failure; BP, bovine pericardium; BPMSC, BP seeded with mesenchymal stem cells; BPMO, BP seeded with mononuclear cells
Treatment with BPMSC and BPMO also resulted in improved Clcr (S = 1.05 ± 0.2 mL/min versus CRF2/3 = 0.4 ± 0.12 versus BP = 0.34 ± 0.09 versus BPMSC = 0.65 ± 0.22 versus BPMO = 0.5 ± 0.07; P < 0.0001) (Figure 2b). Chronic deterioration of renal function in the CRF2/3 model as measured by 1/sCr slope significantly slowed with BPMSC treatment (S = 0.88 ± 0.91 versus CRF2/3 = −0.24 ± 0.03 versus BP = −0.20 ± 0.09 versus BPMSC = 0.78 ± 0.81 versus BPMO = 0.09 ± 0.71; P = 0.034 (Figure 2c). The excretion of PT-24 h was very similar to that of sham animals when the rats were treated with BPMSC or BPMO (S = 5.4 ± 1.1 mg/24 h versus BPMSC = 4.9 ± 2.4 versus BPMO = 7.6 ± 1.6; P = NS), while the untreated groups retained elevated rates of PT-24 h excretion (CRF2/3 = 27 ± 16.8 mg/24 h and BP = 20.2 ± 4.7; P < 0.01) (Figure 2d).
Effects of treatment in the CRF5/6 model
In contrast to the CRF2/3 model, 5/6 nephrectomized rats demonstrated a better response to treatment during the initial 45-day period. During this period of time, both types of cells significantly reduced sCr (Figure 3a). At the end of the 90-day period, the treatment effectively prevented increases in sCr in the CRF5/6 model (S = 5.2% versus CRF5/6 = 128% versus BP = 168% versus BPMSC = 78.6% versus BPMO = 72.4%; P < 0.01) (Figure 3a). Profound decreases in Clcr were observed in the untreated groups, while groups treated with BPMSC and BPMO demonstrated a lower reduction after 90 days (S = 1.05 ± 0.18 mL/min versus CRF5/6 = 0.25 ± 0.17 versus BP = 0.22 ± 0.09 versus BPMSC = 0.46 ± 0.10 versus BPMO = 0.53 ± 0.15; P < 0.01) (Figure 3b). The progression of disease in the CRF5/6 model was significantly retarded using both treatments (S = 0.88 ± 0.9 versus CRF5/6 = −0.49 ± 0.04 versus BP = −0.53 ± 0.10 versus BPMSC = −0.35 ± 0.12 versus BPMO = −0.32 ± 0.13; P < 0.01) (Figure 3c), although to a lesser degree than observed for the CRF2/3 model.
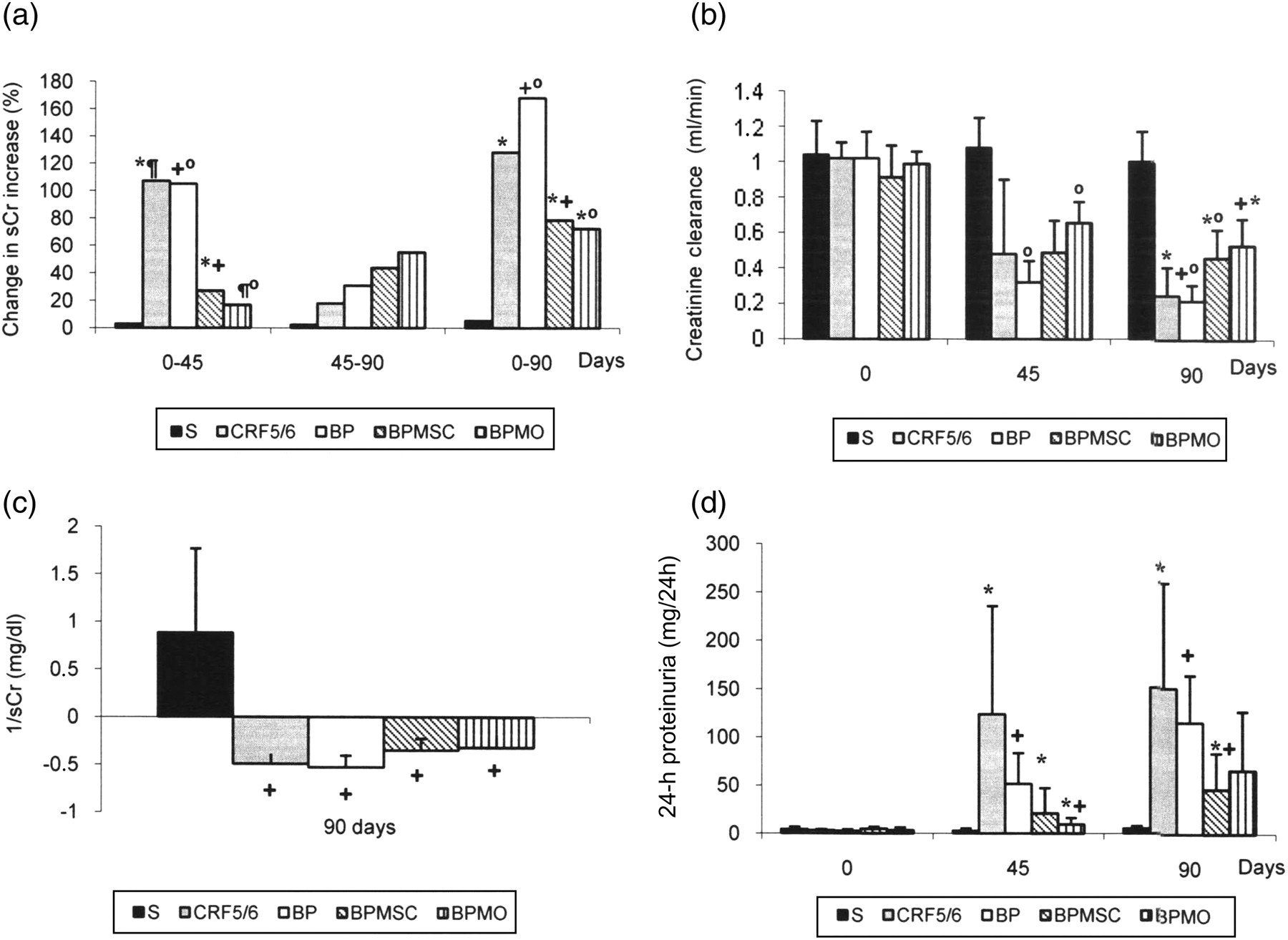
Renal function studies at days 0, 45 and 90 in the 5/6 renal mass reduction model. (a) Percentage increase in sCr, (b) creatinine clearance, (c) slopes of the reciprocal serum creatinine plot (1/sCr), (d) 24-hour proteinuria (PT-24 h). Values are expressed as means ± SD in b, c and d (*P < 0.05, °P < 0.05, + P < 0.01, ¶ P < 0.01). sCr, serum creatinine; S, sham; CRF, chronic renal failure; BP, bovine pericardium; BPMSC, BP seeded with mesenchymal stem cells; BPMO, BP seeded with mononuclear cells
PT-24 h decreased significantly in treated groups after the 45-day period (S = 2.8 ± 1.64 mg/24 h versus CRF5/6 = 124 ± 112 versus BP = 51.6 ± 32 versus BPMSC = 20.8 ± 26.4 versus BPMO = 9.6 ± 6.6; P = 0.012); this effect persisted until day 90 (Figure 3d).
Renal histology
GS, TA, IF and IL were significantly less severe in CRF2/3 rats. In spite of the significantly less severe morphological chronic injury observed in the CRF2/3 model, treatment with BPMSC and BPMO effectively reduced the amount of GS and IF. A trend toward less injury was noted for all other evaluated histological parameters (Table 1).
Histological changes and the effect of treatment with BMDC on the remnant kidneys of 2/3 and 5/6 nephrectomized animals
CRF, untreated chronic renal failure; BP, chronic renal failure with unseeded biomaterial alone; BPMSC, CRF rats treated with BP seeded with mesenchymal stem cells; BPMO, CRF rats treated with BP seeded with mononuclear cells; GS, glomerular sclerosis; TA, tubular atrophy; IF, interstitial fibrosis; IL, interstitial lymphocytic infiltration
Data are expressed as means ± SD (*P<0.05)
The effect of treatment with BPMSC or BPMO in the CRF2/3 animals was more striking and significantly reduced GS, TA, IF and IL (P < 0.05) by at least two-fold. At the end of the study, the treated CRF5/6 animals presented significantly less renal damage when compared with untreated rats.
Immunohistochemical analysis
Monocytes/macrophages and PCNA
The accumulation of macrophages (ED-1-positive cells) was significantly reduced in rats with less severe chronic kidney disease (CRF2/3 = 9.1 ± 3 versus CRF5/6 = 37 ± 10.5 ED-1-positive cells; P = 0.0012); the same as observed with the proliferative activity as expressed by the number of PCNA-positive cells (CRF2/3 = 2.36 ± 1 versus CRF5/6 = 8.33 ± 1.1 PCNA-positive cells; P = 0.0002) (Figures 4a and c).

Immunohistochemistry of renal tissue from 2/3 and 5/6 nephrectomized rats. (a) Immunolocalization of ED-1-positive cells; (b) staining for fibronectin; (c) immunolocalization of PCNA; (d) immunostaining of interstitial α-SM-actin; and (e) p-JNK in the renal cortex. Data are expressed as means ± SD (*P < 0.05, °P < 0.05, + P < 0.01, ¶ P < 0.01). S, sham; CRF, chronic renal failure; BP, bovine pericardium; BPMSC, BP seeded with mesenchymal stem cells; BPMO, BP seeded with mononuclear cells; PCNA, proliferating cell nuclear antigen; SM, smooth muscle; JNK, Jun-N-terminal kinase
Treatment with BPMSC or BPMO decreased the number of ED-1-positive cells in the CRF2/3 model (S = 2.28 ± 0.78 versus CRF2/3 = 9.1 ± 3 versus BP = 9.6 ± 2.8 versus BPMSC = 6.09 ± 1.5 versus BPMO = 5.06 ± 2.4; P = 0.0024) but had no effect on PCNA expression (Figure 4c).
In contrast, a significant decrease in the number of ED-1-positive cells and in the expression of PCNA were observed following BPMSC or BPMO treatment in 5/6 nephrectomized rats (P < 0.001) (Figures 4a, c and 5).
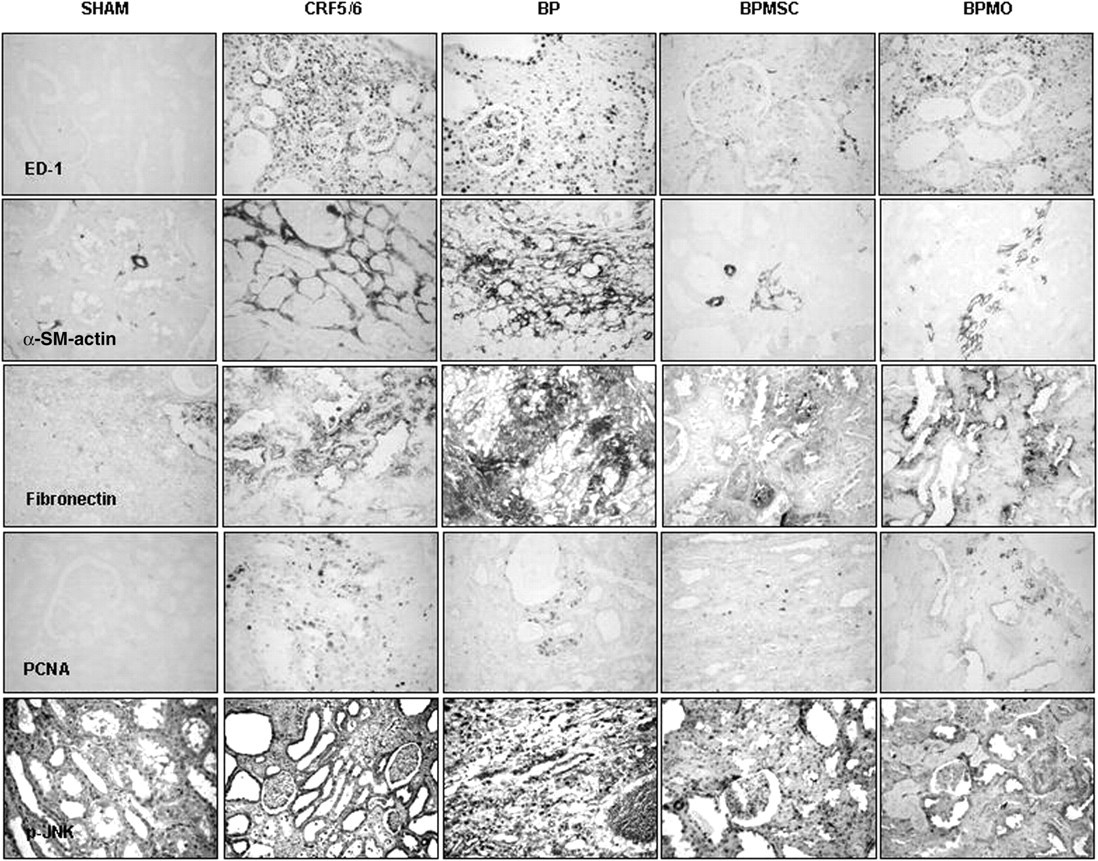
Representative images of immunolocalization of ED-1 cells (macrophages/monocytes), α-SM-actin, fibronectin, PCNA and p-JNK in the renal cortices of the sham, CRF5/6, BP, BPMSC and BPMO groups (CRF5/6 model) on postoperative day 90 (×40). CRF, chronic renal failure; BP, bovine pericardium; BPMSC, BP seeded with mesenchymal stem cells; BPMO, BP seeded with mononuclear cells; PCNA, proliferating cell nuclear antigen; SM, smooth muscle; JNK, Jun-N-terminal kinase
Fibronectin and α-SM-actin
Staining for both markers matched the degree of severity of CRF. Much lower expression of both molecules occurred in the CRF2/3 model compared with the 5/6 model. Treatments with BPMSC and BPMO were equally effective at reducing fibronectin and α-SM-actin expression in both CRF2/3 and CRF5/6 animals (P < 0.05).
Efficacy of treatment was observed in CRF2/3 rats in spite of the low expression of these proteins in this model (Figures 4b, d and 5).
Jun-N-terminal kinase
In contrast to the results with CRF2/3 rats, JNK activity markedly increased after 5/6 nephrectomy (Figure 4e; P < 0.01). As observed with the increase in sCr, unseeded BP groups showed the highest expression of JNK activity. Comparisons between the two models showed differences according to the degree of tissue injury. Only BPMSC reduced the expression of JNK in the 2/3 model, while the same effect was observed with both treatments in the 5/6 nephrectomized rats (Figures 4e and 5).
Discussion
We and other groups have previously shown that the administration of BMDC into a chronically damaged kidney improves renal function and retards the progression of chronic kidney disease in 5/6 nephrectomized rats. 5–9
In the present study, our main goals were to elucidate whether scaffolds seeded with BMDC could be an effective alternative to deliver BMDC in rats with CRF and whether the amount of remnant renal mass would impact the efficacy of cellular therapy.
Major considerations that led us to use this approach were the ability of decellularized scaffolds made from biological tissues to retain the properties necessary to interact with the host and the capacity of the scaffolds to favor the process of proliferation and differentiation of precursor cells. 20 Moreover, the inflammatory reaction elicited after scaffold implantation and associated with the plasticity of BMDC would generate a local microenvironment that favors tissue remodeling and repair. 21
As we hypothesized that cell therapy could be more effective if administered during less severe stages of the disease, we evaluated the effectiveness of treatment in rats sustained by a remnant renal mass two-fold greater than that of the traditional 5/6 model using the 2/3 reduction of renal mass model.
Our study revealed two main findings. First, the approach of using seeded scaffolds was effective in retarding the progression of disease in both models of CRF. Significantly lower increases in sCr and PT-24 h improved CLcr and reduced slopes of the progression of CRF were seen only in animals treated with BPMSC and BPMO (Figures 2a and b). Second, we provide evidence that the amount of remnant renal mass positively did impact the efficacy of cell therapy. After 90 d, renal functional studies showed that in the 2/3 model, treatment with BPMSC and BPMO fully reversed the decline in the 1/sCr slopes and kept the rate of PT-24 h excretion similar to that of the sham animals. Despite the statistically significant results, the progression of CRF was only attenuated in rats with a 5/6 nephrectomy (Figures 3 and 4).
The kinetics of sCr elevation after surgery also differed between the two models. Treatment of CRF2/3 rats with BPMSC or BPMO did not significantly alter the progressive increase in sCr during the initial 45 d after surgery, but the increase in sCr leveled off thereafter. In contrast, both treatments prevented the increase in sCr during the same period in the 5/6-nephrectomized animals, but after 45 d, neither treatment could effectively avoid the increase in sCr (Figures 2a and 3a). These results could be due to differences in the amount of damaged tissue, the capacity of BMDC to promote repair in response to inflammatory cues within the local microenvironment or to the reduced number of host stem cell niches consequent to renal mass reduction. 21,22 Interestingly, the implantation of unseeded BP seems to accelerate the progression of CRF in animals with the 5/6 reduction in renal mass, suggesting additional inflammatory stimuli elicited by the biomaterial in the already severely injured kidney tissue. 23
It has been suggested that BMDC can reduce renal injury and facilitate tissue repair by upregulating the expression of anti-inflammatory cytokines and chemokines by the host infiltrating macrophages, which results in reduced glomerulosclerosis and fibrosis. 21,24–26 In fact, comparisons of the morphological findings between the two models of CRF showed more glomerulosclerosis, tubular atrophy and fibrosis in the CRF5/6 group than in the CRF2/3 group (Table 1). The amelioration of renal function following treatment with BMDC was also associated with a significant improvement in the histological features of both groups of CRF animals. Taking into account the extent of renal damage, the greatest ‘renoprotective’ effect occurred in the 5/6 nephrectomized animals, with much less GS, IF and LI observed in these remnant kidneys after treatment with BPMSC and BPMO when compared with untreated animals (Table 1). Even more interesting is the observation that even in the presence of smaller amounts of histological lesions, a significant reduction in IF could still be detected in the treated CRF2/3 groups (Table 1).
The accumulation of macrophages in the renal interstitium plays an important role in the process of renal inflammation that occurs during the initiation and progression of chronic kidney injury. This proinflammatory response is mediated in part by activation of the JNK signaling pathway and has been associated with chronic inflammation and tubular apoptosis. 27 Ma et al. 28 demonstrated that the inhibition of JNK signaling prevents the development of a proinflammatory response and provides protection against the progression of crescentic glomerulonephritis. Therefore, we assessed the effect of treatment with BMDC on the accumulation of macrophages and the expression of fibrogenic molecules and JNK signaling components in the remnant renal tissue of 2/3 and 5/6 nephrectomized animals. As expected, the number of macrophages/monocytes and the proliferative activity was three- to four-fold higher in CRF5/6 animals than in CRF2/3. Accordingly, the extent of the fibrogenic response was also greater in CRF5/6 animals, which expressed significantly more fibronectin and α-SM-actin. In the same way, JNK staining increased after renal mass reduction and was slightly greater in CRF5/6 rats, suggesting a direct correlation between the activation of this pathway and the amount of tissue damage.
Treatment with BPMSC and BPMO significantly reduced the number of macrophages and the expression of fibronectin, α-SM-actin and JNK in both models. Treatments reduced the proliferative activity only in animals with severe CRF5/6, which was probably a consequence of more inflammation and tissue damage in this model. Interestingly, the reduction of JNK expression in the CRF2/3 model after BPMSC treatment was observed only in rats with unseeded BP. This result corroborates the idea that the biomaterial alone could elicit additional inflammatory stimuli throughout the signaling pathway.
Subcapsular, intraparenchymal or intravenous injection of BMDC and lineage-negative cells reduces renal injury and the infiltration of macrophages and lymphocytes in the 5/6 nephrectomy model, but the mechanisms by which the stem cells induce kidney repair remain controversial. 5–8 Differentiation into different types of renal cells, direct replacement of damaged structures and the release of growth factors and cytokines are some of the mechanisms proposed to promote functional and structural repair. 29
Despite limited information on the relationship of hyperfiltration and inflammation in this model, it is likely that lymphocyte and macrophage infiltration play a significant role in the development of fibrosis. 30
Biomaterials could exert their effects in two ways, by serving to deliver cells to the remnant renal parenchyma and by acting as a template for tissue regenerate. In addition, scaffolds could favor cell adhesion and differentiation and enhance stimulatory growth factors; in this way, they could contribute to amplify the regenerative capacity of BMDC. Moreover, it is important to consider the capacity of biomaterials to promote regeneration throughout a series of mechanisms that, when combined with seeded and resident stem cells, provide stimuli favoring regeneration instead of fibrosis. 31
For the first time, our experiments have shown that biomaterial seeded with BMDC was effective at preventing the progressive deterioration of chronic kidney disease. This effect was associated with a significant reduction in glomerulosclerosis and interstitial fibrosis, probably due to attenuation of macrophage accumulation and reduction of the proliferative activity and expression of myofibroblasts and fibronectin. Moreover, we demonstrated that the amount of remnant renal mass does impact on the efficacy of treatment, which suggests that cellular therapy should be started in less advanced stages of CRF.
Using the approach of combining the biomaterial and BMDC, we have provided a novel and efficient route for cellular therapy of CRF. We speculate that seeded scaffolds could have the same beneficial effect when implanted in other sites beyond renal tissue.
Footnotes
ACKNOWLEDGEMENTS
We thank Rita Cavaglieri for her skilled technical assistance. This work received partial financial support from FAPESP, CNPq and FAMERP/FUNFARME and was partially supported by grants from the FAMERP-BAP.