
Abstract
Bone marrow mesenchymal stem cells (BMMSCs) have shown promise in repairing injured myocardium. However, few studies have explored the potential of BMMSC transplantation for dilated cardiomyopathy (DCM). In this study we aimed to examine whether BMMSC transplantation improves the cardiac function of dilated cardiomyopathy and investigate the underlying mechanism. We established a DCM model in rabbit, then transplanted BMMSCs induced by 5-azacytidine into the rabbit, and determined the left ventricular pressure and the expression of vascular endothelial growth factor (VEGF) and its receptors. Immunohistochemisty, ultrastructural and reverse transcription polymerase chain reaction (RT-PCR) analysis proved that 5-azacytidine induced the differentiation of BMMSCs into cardiomyocyte-like cells. Upon transplantation of the induced BMMSCs into a DCM model, significantly higher maximum rates of rise and decline (±dp/dt) of left ventricular pressure and left ventricular systolic pressure, as well as much lower left ventricular diastolic pressure, were observed compared with the control group (P < 0.05). After four weeks, deposition of collagen fibers in the myocardium of transplantation group was reduced, accompanied by increased expression of VEGF and its receptors as detected by RT-PCR. Taken together, our results suggest that BMMSC transplantation could alleviate DCM through angiogenesis via the upregulation of VEGF and its receptors.
Keywords
Introduction
Dilated cardiomyopathy (DCM) is a kind of heart disease characterized by unilateral or bilateral enlargement of the cardiac chamber, myocardial fibrosis and myocardial systolic dysfunction. Besides being ischemic heart disease, DCM may also cause congestive heart failure (CHF).
Because neither traditional medicine nor interventional therapy can regenerate myocardial cells, cases of heart failure show poor prognosis. 1 Myocardial cells in adults are a kind of terminally differentiated cell, and are considered to have very limited replication capability. 2 Therefore, they can not undergo regeneration and repair, but instead they form fibrotic scar and gradually generate ventricular remodeling, which would lead finally to heart failure. 3 Supplementing muscle-derived cells to the injured myocardium through cellular cardiomyoplasty, 4 and re-building functional myocardial cells can improve the recipient's cardiac function. Thus, it has become a promising treatment to cure heart failure resulting from DCM.
In recent years, bone marrow mesenchymal stem cells (BMMSCs) originating from the mesoderm have gained broad application prospects in repairing injured myocardium because they are prone to isolation and culture, can self-replicate and have great potential for proliferation, and can differentiate into various kinds of cells under certain induction conditions. 5–8 As donor cells, they can be transplanted into the recipient's heart to promote the restoration of cardiac function of the heart suffering from heart failure caused by ischemic myocardial infarction and non-ischemic cardiomyopathy. 9,10 Therefore, it has become an important source of donor cells for cellular cardiomyoplasty.
It has been proposed that the mechanism by which BMMSC transplantation improves ischemic heart function is related to angiogenesis and its relevant receptors. 11,12 At present, however, there are few reports on whether, in a DCM setting, BMMSC transplantation affects the expression of vascular endothelial growth factor (VEGF) and its receptor. Therefore, in this study we aimed to examine whether BMMSC transplantation improves the cardiac function of DCM and explore the underlying mechanism. Based on in vivo expansion and directed induction of BMMSCs into cardiac-like cells, we transplanted these cells into a rabbit model of heart failure resulting from DCM, and observed the influence of induced BMMSC transplantation on cardiac function. We further investigated the deposition of myocardial collagen fibers and the expression of VEGF and its receptor to elucidate the possible mechanism.
Material and methods
DCM animal model
The New Zealand white rabbits used in the experiment were provided by the Department of Laboratory Animals, Xinjiang Medical University. Twenty-five male New Zealand rabbits (weight between 2.1 and 2.3 kg) were chosen as a source of BMMSC donor cells. One hundred and twenty female rabbits (weight between 2.2 and 2.5 kg) were randomly divided into three groups: the normal group, the transplant group and the control group (n = 40). Intraperitoneal injection of 2 mg/kg adriamycin (Shenzhen Wanle Pharmaceutical Company, Shenzhen, China) was performed for the transplant group and the control group every week for six consecutive weeks, while the normal group was injected with the same volume of saline. 13 After six weeks, the general behavior and the mortality rate of rabbits were observed, and the ejection fraction and left ventricular end-diastolic dimension (LVEDD) of rabbits was checked by ultrasonic apparatus to see whether the model was successful. All animals received humane care in compliance with the Principles of Laboratory Animal Care formulated by the National Society of Medical Research and the Guide for the Care and Use of Laboratory Animals, published by the US National Institutes of Health. The protocol was approved by the Ethics Committee of the First Affiliated Hospital of Xinjiang Medical University.
BMMSC isolation and culture
Male rabbits were subjected to intraperitoneal anesthesia (with chloral hydrate), and the BMMSCs were isolated from hind limbs and cultured as described previously. 14 Briefly, under sterile conditions, tibia and femur bone marrow cells screened with a 200 molybdenum screen (BD Company, Shanghai, China) were centrifuged for eight minutes at 1500 rev/min. The pellet was washed twice with phosphate-buffered saline (PBS) and re-suspended in Dulbecco's modified Eagle's medium (DMEM) supplemented with 10% fetal bovine serum (FBS) complete culture medium. The cells were inoculated into culture bottles at 5 × 108/mL and cultured in a CO2 incubator at 37°C. The medium was changed after 24 h, and then changed every three or four days to remove the hematopoietic stem cells not adhering to the wall. When the cells were 80–90% confluent, they were passaged 1:2 by trypsinase. For induction, BMMSCs of passage 1 were cultured in DMEM complete media for three days, and the media was changed to 10 μmol/L 5-azacytidine complete culture medium. The cells were incubated in CO2 incubators at 37°C for 24 h, after which the media was changed to DMEM complete media and cultured for another four weeks.
Primary culture of myocardial cells
The hearts were taken from fetal rabbits born within eight days and the myocardium was cut into fragments of 0.2 cm3 with an ophthalmic scissor. Then the fragments were subjected to trypsinase digestion with shaking at 37°C until the myocardial cells were fully digested. The cells were collected and re-suspended in DMEM supplemented with 15% FBS complete culture medium. The cells were inoculated into culture bottles and cultured in a CO2 incubator at 37°C for 150 min. Then, purified myocardial cells were obtained by differential adhesion method and cultured in DMEM complete media.
Reverse transcription polymerase chain reaction
Total RNA was extracted from BMMSCs of passage 1, BMMSCs induced for four weeks, and primarily cultured myocardial cells, or from the myocardium isolated from the rabbits by Trizol one-step method using a TAKARA RT-PCR kit (Takara/Invitrogen, Shanghai, China) following the manufacturer's instructions. cDNA was synthesized from total RNA at the cycle of 30°C for 10 min, 42°C for 30 min and 99°C for 5 min. For polymerase chain reaction (PCR), after 2 min denaturation at 94°C, cDNA was amplified for 35 cycles (94°C 40 s, 58°C 40 s and 72°C 1 min) followed by final extension at 72°C for 10 min. Primer sequences (synthesized by Takara Biotechnology, Dalian, China) were: ANP, 5′ GAGTGAGCCGAGACAGCA 3′/5′ TGAGACGGGTTGACTTCC 3′; BNP, 5′ TCTCAAAGGACCAAGGC 3′/5′ GTGCTGGAAGATAAGAAACA 3′; α-MHC, 5′ GGCACCGTGGACTACAAC 3′/5′ CCCTTTCCCGCTATCAA 3′; β-MHC, 5′ GGACGTTTATTGACTTCGG 3′/5′ CTTTGCTTTGCCTTTGC 3′; VEGF, 5′ GCAACACCAAGTCCGAATG 3′/5′ GCCTACAGAATGGAGCAAAT 3′; Flt-1, 5′ CGTGTATGGCATCCCTC 3′/5′ GTGCTAACCGTCTTATTGG 3′; Flk-1, 5′ CACGGTTGGGCTACTGC 3′/5′ ACCTTCTGCCATCACG 3′; and β-actin, 5′ GCCAACCGTGAAAAGATG 3′/5′ CCAGGATAGAGCCACCAAT 3′. The sizes of the products were as follows: ANP, 318 bp; BNP, 348 bp; α-MHC, 477 bp; β-MHC, 395 bp; VEGF, 463 bp; Flk-1, 415 bp; Flt-1, 198 bp; and β-actin, 701 bp. The products were separated by electrophoresis and subjected to semiquantitative analysis with β-actin as internal control.
Transplantation of induced BMMSCs
The induced BMMSCs were incubated with 1/10 volume of 10 μg/mL 4′,6 diacetyl 2 phenylindole (DAPI) in DMEM complete media at 37°C for 30 min. Then the cells were washed twice with PBS to get rid of unconjugated DAPI, and re-suspended in serum-free DMEM media at 5 × 106/200 μL, and kept on the ice for less than one hour before the injection. Rabbits were anesthetized by intraperitoneal injection of 10% chloral hydrate at 3 mL/kg. After tracheal intubation, a rodent ventilator was used to perform aerobic positive pressure ventilation. Next, thoracotomy was performed layer by layer on the fourth intercostals in the left. Then the pericardium was opened to make the heart exposed outside the chest. Induced BMMSCs marked by DAPI as above were injected into the left ventricular free wall in five spots at 5 × 106/200 μL, with 40 μL in every spot. For the control group, the same volume of serum-free DMEM was injected. After the injection, the heart was put back to its normal place instantaneously and the chest was sutured layer by layer. The air was eliminated in the pleural with negative pressure, and the pipes were plugged when rabbits resumed spontaneous respiration. Intraperitoneal injection of penicillin was performed to prevent the infection.
Determination of cardiac function with hemodynamics
The rabbits were measured for the weight at the end of the first, second, third and fourth week after the transplantation operation. Then the rabbits were anesthetized and subjected to tracheal intubation as described above. The right carotid artery was connected to 8-channel polyFig (AD Company, Australia) and the maximum rate of rise and decline of left ventricular pressure (±dp/dt), and left ventricular systolic pressure (LVSP) and left ventricular diastolic pressure (LVDP) were determined with a pressure converter.
Statistics analysis
The data were represented as mean number ± standard deviation (
Results
Characterization of induced BMMSCs
To characterize the induced BMMSCs we first performed immunofluorescence analysis. The results showed that BMMSCs of passage 1 were negative for CD34 and positive for CD44 and CDw90, indicating that they are BMMSCs but not the hematopoietic stem cells. Although some BMMSCs were positive for α-sarcomeric actin (indicated by the black arrow in Figure 1a), most of them were negative for troponin T. After induction, most cells were positive for α-sarcomeric actin (Figure 1b), and also positive for troponin T (shown by the green signal in the cytoplasm, Figure 1c), indicating that induced cells expressed myocardial specific protein. The proportion of α-sarcomeric actin positive cells was 22.1% before induction and 47.3% after induction. The proportion of troponin T-positive cells was 31.5% after induction. As a positive control, more than 95% of primary cultured myocardial cells were positive for both α-sarcomeric actin and troponin T.
Immunohistochemical analysis of bone marrow mesenchymal stem cells (BMMSCs) before and after the induction by 5-azacytidine. (a) Positive staining for α-sarcometric actin in BMMSCs before the induction; (b) positive staining for α-sarcometric actin in BMMSCs after the induction for four weeks; (c) positive staining for troponin T in BMMSCs after the induction for four weeks. Magnification: ×400 (A color version of this figure is available in the online journal)
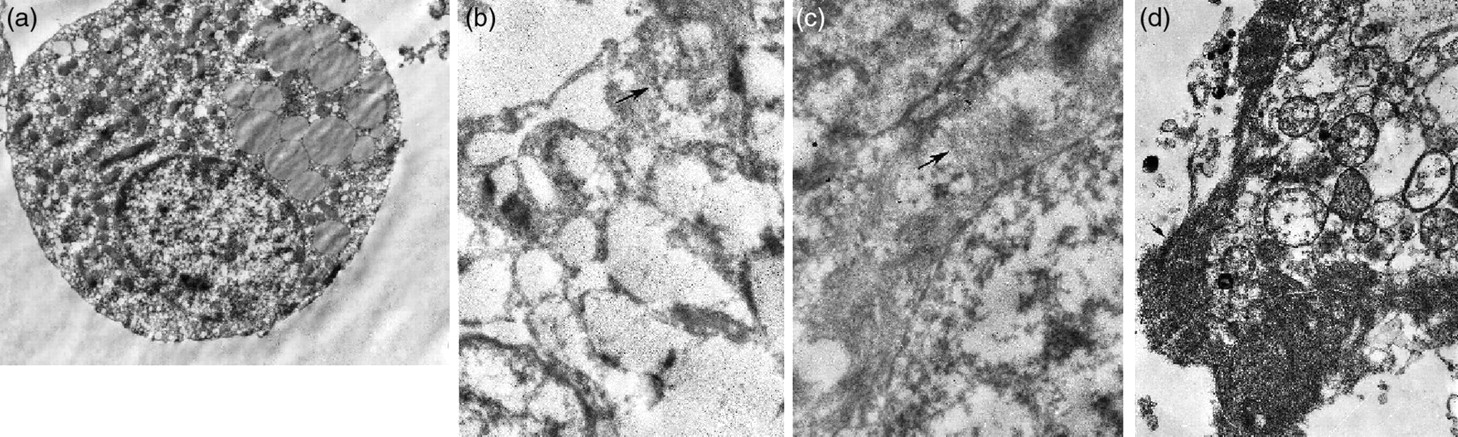
Next we examined the ultrastructure of induced BMMSCs. Under an electron microscope, most BMMSCs were round or round-like, with relatively big nuclei and clear nucleoli before induction. The chromatin was loose, and the nuclear cytoplasmic ratio was high. Within the cytoplasm, the number of organelles was small and the organelles were not developed (Figure 2a). In contrast, induced BMMSCs demonstrated glycogen granules (indicated by the arrow in Figure 2b) and a typical arrangement of the myofibril (Figure 2c) and myocardial structure (Figure 2d).

Electron microscopy analysis of bone marrow mesenchymal stem cells (BMMSCs) before and after the induction by 5-azacytidine. (a) BMMSCs before the induction; (b) BMMSCs after the induction for four weeks, glycogenosome in the plasma was represented; (c) BMMSCs after the induction for four weeks, myofibril in the plasma was represented; (d) cardiomyocytes in primary culture as control. Magnification: ×8000
Finally, we investigated the expression of molecular markers for myocardial cells in the induced BMMSCs. By reverse transcription (RT)-PCR we found that ANP, BNP, α-MHC and β-MHC were expressed in induced BMMSCs but not in BMMSCs that were not induced. As a positive control, primary cultured myocardial cells showed the expression of these markers for myocardial cells (Figure 3). Taken together, these data demonstrated that the induced BMMSCs were cardiac-like cells.
Reverse transcription polymerase chain reaction analysis of the expression of cardiac-specific genes in bone marrow mesenchymal stem cells (BMMSCs) before and after the induction by 5-azacytidine. (a) ANP; (b) BNP; (c) α-MHC; and (d) β-MHC. 1: cardiomyocytes; 2: BMMSCs before the induction; 3: BMMSCs after the induction for four weeks; M: marker
Transplantation of induced BMMSCs improves the cardiac function of rabbits
The vitality of the rabbits was decreased after being given adriamycin, with a 10% (8/80) mortality rate after the establishment of the model. Compared with the normal group, the ejection fraction was reduced significantly (62.3 ± 6.4 versus 85.2 ± 3.7, P < 0.05) while LVEDD was increased significantly (13.7 ± 1.9 versus 11.2 ± 1.2, P < 0.05) in the control group, indicating that the DCM model was successful. Rabbits exhibited poor endurance of the operation, with the postoperation survival rate of the transplant group (T) at 73% (27/36), and the survival rate of the control group (C) with heart failure at 80% (29/36).
Notably, compared with the control group, the transplantation group had a significantly higher maximum rate of rise and decline (±dp/dt) of left ventricular pressure and LVSP (P < 0.05), and a significantly lower rate of LVDP (P < 0.05) (Tables 1–4), indicating that the cardiac function was significantly improved in the transplantation group.
Comparison of left ventricular systolic pressure (LVSP) between transplant group and control group (mmHg, 
Transplant group had higher LVSP than control group, *P < 0.05
Comparison of left ventricular diastolic pressure (LVDP) between transplant group and control group (mmHg, 
Transplant group had visibly lower LVDP than control group, *P < 0.05
Comparison of maximum rate of rise of left ventricular pressure (LVP) between transplant and control group
dp/dt, rate of rise of left ventricular pressure
Transplant group had visibly higher +dp/dt than control group,*P < 0.05
Comparison of maximum rate of decline of left ventricular pressure (LVP) between transplant and control group
dp/dt, rate of rise of left ventricular pressure
Transplant group had visibly higher −dp/dt than control group, *P < 0.05
Change of the basic structure of myocardium
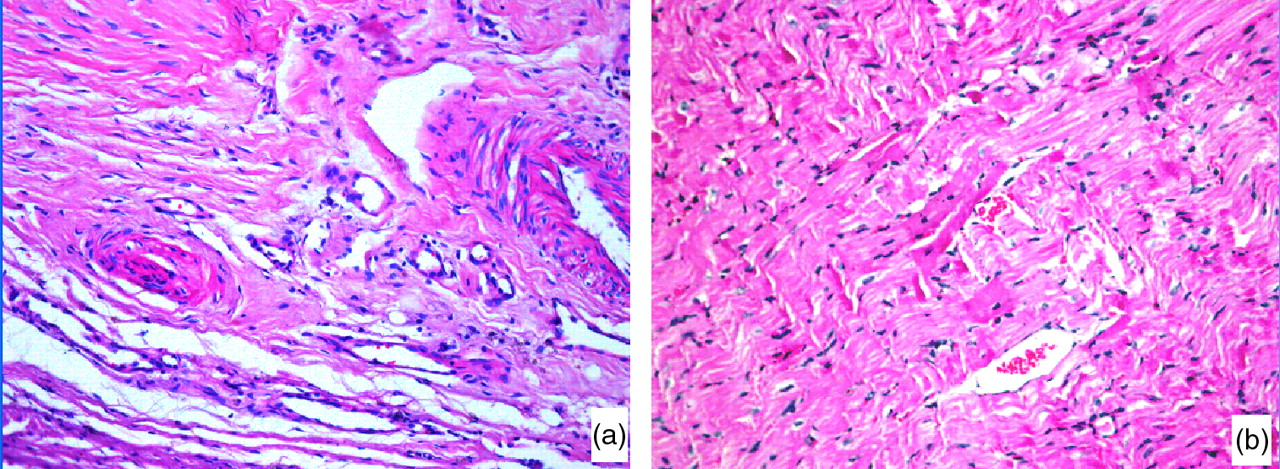
Hematoxylin and eosin staining showed that adriamycin caused minor vacuolar degeneration, accompanied by myocardial atrophy in the control group (Figure 4a). However, after transplantation, these abnormalities of the myocardium were alleviated (Figure 4b).
Immunohistochemical analysis of myocardium in the control and transplantation groups. (a) Hematoxylin and eosin (HE) staining of the myocardium in the control group four weeks after the operation. (b) HE staining of the myocardium in the transplantation group four weeks after the operation. Magnification: ×200 (A color version of this figure is available in the online journal)
Survival of transplanted BMMSCs
To confirm that transplanted BMMSCs directly contribute to the improved cardiac function, we performed DAPI tracing and immunofluorescence analysis, which showed that DAPI-marked BMMSCs were still visible in the fourth week after the operation (Figure 5).
Labeling of bone marrow mesenchymal stem cells (BMMSCs) showing their survival four weeks after the transplantation. Magnification: ×400 (A color version of this figure is available in the online journal)
Detection of myocardial collagen fibers
In the first and fourth week after the operation, more deposition of collagen fibers was observed in the control group, and the fibers had obvious fusion and a disordered arrangement. In contrast, much less deposition and fusion of collagen fibers were observed in the transplantation group (Figure 6). In addition, a semiquantitative analysis based on the optical density value confirmed significantly less deposition of collagen fibers in the transplantation group than in the control group (P < 0.05, Table 5).

Messon staining of myocardium in normal, control and transplantation groups. (a) Normal group; (b) control group; (c) control group one week after the operation; (d) control group four weeks after the operation; (e) transplantation group one week after the operation; (f) transplantation group four weeks after the operation. Magnification: ×200 (A color version of this figure is available in the online journal)
Comparison of optical density of myocardial collagen fibers
*P < 0.05 versus control group; **P < 0.01 versus control group
Transplantation of induced BMMSCs upregulates the expression of VEGF and its receptors in the myocardium
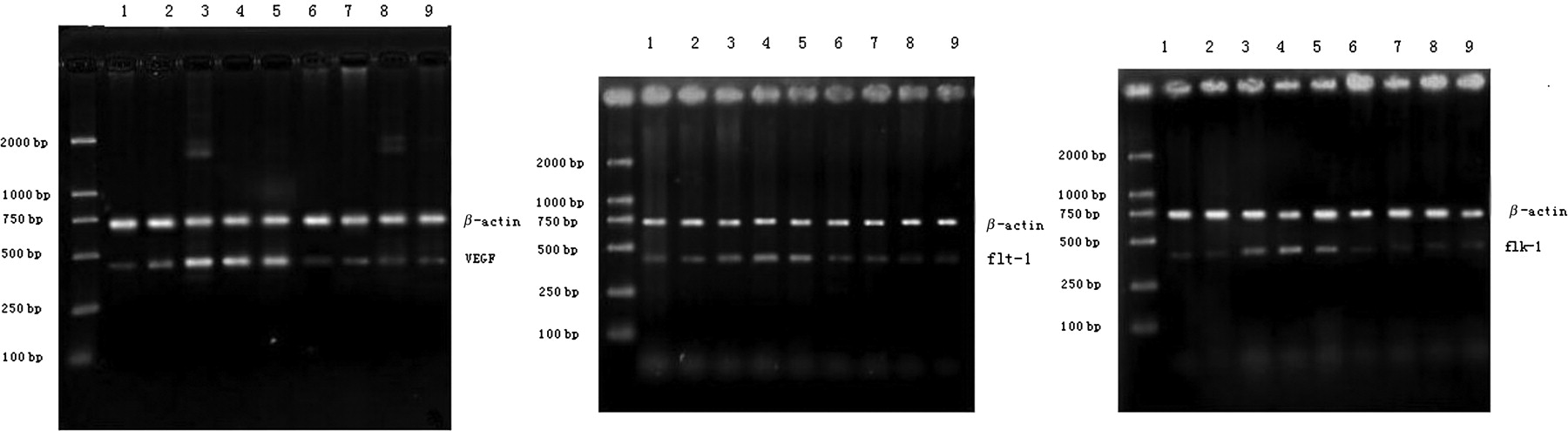
To explore the potential mechanism by which transplanted BMMSCs improve the cardiac function of rabbits with DCM, we detected the expression of VEGF and its receptors in the myocardium of rabbits. RT-PCR analysis showed that VFGF expression in the transplantation group was higher than that of the control group in the first, second and third week after the operation, reaching a peak in the second week and then declining gradually. Similarly, the expression of Flt-1 and Flk-1 was higher in the transplantation group than the control group after the operation, reaching a peak in the third week after the operation and then declining gradually (Figure 7). The semiquantitative analysis of the expression of VEFG and its receptors is listed in Table 6.
Reverse transcription polymerase chain reaction analysis of the expression of vascular endothelial growth factor and its receptors in the myocardium from the normal, control and transplantation groups. 1: normal group; 2–5: transplantation group; 6–9: control group
Ratio of the optical density of VEGF, flk-1 and flt-1 mRNA levels normalized to β-actin (
VEGF, vascular endothelial growth factor
Discussion
Inspiring achievements have been achieved in basic and clinical research on the use of stem cell transplantation in the treatment of cardiovascular diseases. Currently, various kinds of stem cells have been tested as potential donor cells. Embryonic stem cells are not suitable for clinical application because they raise ethical problems, and could cause immunological rejection, differences with myocardial cell action potential and even arrhythmia. 15 BMMSCs possess the capability of multidirectional differentiation because they are autologous cells, making them the most promising source of donor cells. 16 Although myocardial infarction has gained much attention in the past, 17,18 DCM that features myocardial diffuse injury is another important cardiovascular disease that could cause CHF. Reduction of total myocardial cells caused by DCM will bring continuous adverse effects to cardiac function. Therefore, BMMSC angioplasty has been proposed to promote the regeneration of myocardial cells and prevent ventricular remodeling, with the potential of preventing heart failure. Although the long-term benefits of stem cell transplantation for DCM are still controversial, most studies suggest that BMMSC transplantation is safe and effective, especially for BMMSCs that have been induced and optimized in vitro.
Experimental and clinical studies with animals have proven that BMMSCs transplantation could improve cardiac function. It has been postulated that transplanted cells differentiate into myocardial cells, participate in the host's cardiac contraction and improve ventricular function. 19–21 However, the mechanism by which BMMSCs differentiate into myocardial cells remains elusive.
In this study we used 10 μmol/L 5-azacytidine to induce BMMSCs to differentiate into cardiac-like cells in vitro. Troponin T is exclusively expressed in myocardial cells and is the specific marker for myocardial cells, Based on immunohistochemical analysis, we observed positive staining for α-sarcomeric actin and negative staining for troponin T in some BMMSCs before the induction, indicating that a small number of BMMSCs could spontaneously differentiate into various kinds of cells, 22 but could not spontaneously differentiate into myocardial cells. After being inducted by 5-azacytidine, a large part of BMMSCs showed positive staining for both α-sarcomeric actin and troponin T, indicating that BMMSCs gradually differentiate from muscle cells into myocardial cells after being inducted by 5-azacytidine, which is consistent with the previous report. 14
Next, we characterized the induced BMMSCs by electron microscopy and molecular biology techniques. Electron microscopy showed that after 5-azacytidine induction, the intracellular organelles of BMMSCs developed, with glycogen granules and obvious myofibril arrangement, similar to the structure of myocardial cells. RT-PCR analysis showed that after induction, BMMSCs expressed the components of the main structure of myofibrils: α-MHC and β-MHC, the two subunits of thick filament myosin heavy chain. In addition, induced BMMSCs expressed myocardial specific factors ANP and BNP, which are important peptide hormones for humoral regulation. Taken together, these data provide evidence that BMMSCs differentiate into cardiac-like cells.
Notably, we demonstrated that autologous transplantation of BMMSCs improved the cardiac function of rabbits with DCM caused by adriamycin. We observed that the maximum rates of rise and decline of left ventricular pressure and LVSP were significantly higher in the transplantation group than in the control group, but the rate of LVDP was much lower in the transplantation group. Importantly, the improvement of cardiac function was only obvious three weeks after the transplantation, suggesting complex processes such as further differentiation of BMMSCs into myocardial cells in the host's body, interaction with the host's myocardial cells and time needed to form electric-mechanical coupling. Indeed, the differentiation from BMMSCs into cardiac-like cells is related to the biochemical and physical factors in the myocardial microenvironment, 23 including direct contact with myocardial cells, traction force between cells and the electrophysiological environment. The myocardial structure of induced BMMSCs examined under electron microscope suggested that excitation–contraction (E–C) coupling may be formed between the transplanted cells and host cells, but to confirm this, further electrophysiological studies are needed. Meanwhile, cell factors, hormones, ion gradients and other soluble factors produced by neighboring cells modulate BMMSCs to differentiate into myocardial cells. 24–26
Mechanistically, we found that BMMSC transplantation prevented the fusion of collagen fibers to some extent and maintained the orderly structural arrangement of myocardial tissue, which may help improve myocardial stretch, compliance and ventricular function. The formation and deposition of collagen fibers involve a lot of cytokines such as TGF-β1, IGF-1 and TNF-α. 27 These factors protect the basic structure of myocardium by adjusting fibronectin and organizing the content and composition of collagen fibers. The influence of BMMSC transplantation on the expression of these factors are yet to be studied, which may provide possibility for preventing myocardial fibrosis and improving ventricular function.
VEGF and its receptors play an important role in the continuous promotion of angiogenesis of ischemic myocardium. 28 Angiogenesis and regeneration of myocardial cells caused by transplantation contribute to further improvement of cardiac function. 29 Therefore, we wonder whether angiogenesis is a possible mechanism by which BMMSC transplantation improves cardiac function. When we compared the expression of VEGF and its receptor in the myocardium before and after BMMSC transplantation, we found that BMMSC transplantation not only upregulated the expression of VEGF, but also upregulated the expression of VEGF receptors, Flt-1 and Flk-1. Interestingly, unsynchronized upregulation of VEGF and its receptors was observed. VEGF expression reached a peak in the second week after the operation, whereas the expression of its receptors reached a peak in the third week. The asynchrony in upregulation could promote angiogenesis and the restoration of ischemic cardiac function continuously and steadily.
Undoubtedly, further studies are necessary to explore other benefits brought by BMMSC transplantation, including increased secretion of antiapoptosis factors, electrophysiological characteristics of transplanted cells, factors that promote muscle protein synthesis, and other autocrine and paracrine functions of transplanted BMMSCs. These experimental investigations will pave the way for the application of BMMSCs in cardiovascular regenerative medicine.
Footnotes
Acknowledgements
This study was sponsored by a grant (no. 200821145) under the Natural Science Foundation of Xinjiang Uygur Autonomous Region. We thank Dr Chunmei Wang and Dr Tao Jiang for their advice and support.