
Abstract
Mechanical ventilation (MV) can induce lung oxidative stress, which plays an important role in pulmonary injury. This study compared protective conventional mechanical ventilation (CMV) and high-frequency oscillatory ventilation (HFOV) for oxygenation, oxidative stress, inflammatory and histopathological lung injury in a rabbit model of acute lung injury (ALI). Rabbits (n = 30) were ventilated at FiO2 1.0. Lung injury was induced by tracheal saline infusion (30 mL/kg, 38°C). Animals were randomly assigned to: (a) sham control (CG: tidal volume [V T] 6 mL/kg, positive end expiratory pressure [PEEP] 5 cmH2O, respiratory rate [RR] 40 ipm); (b) ALI + CMV (CMVG: V T 6 mL/kg, PEEP 10 cmH2O, RR 40 ipm); or (c) ALI + HFOV (HFG: mean airway pressure [Paw] 14 cmH2O, RR 10 Hz) groups. Lung oxidative stress was assessed by total antioxidant performance assay, inflammatory response by the number of polymorphonuclear leukocytes/bronchoalveolar lavage fluid/lung and pulmonary histological damage was quantified by a score. Ventilatory and hemodynamic parameters were recorded every 30 min. Both ALI groups showed worse oxygenation after lung injury induction. After four hours of ventilation, HFG showed better oxygenation (partial pressure of oxygen [PaO2] – CG: 465.9 ± 30.5 = HFG: 399.1 ± 98.2 > CMVG: 232.7 ± 104 mmHg, P < 0.05) and inflammatory responses (CMVG: 4.27 ± 1.50 > HFG: 0.33 ± 0.20 = CG: 0.16 ± 0.15; polymorphonuclear cells/bronchoalveolar lavage fluid/lung, P < 0.05), less histopathological injury score (CMVG: 5 [1–16] > HFG: 1 [0–5] > CG: 0 [0–3]; P < 0.05), and lower lung oxidative stress than CMVG (CG: 59.4 ± 4.52 = HFG: 69.0 ± 4.99 > CMVG: 47.6 ± 2.58% protection/g protein, P < 0.05). This study showed that HFOV had an important protective role in ALI. It improved oxygenation, reduced inflammatory process and histopathological damage, and attenuated oxidative lung injury compared with protective CMV under these experimental conditions considering the study limitations.
Keywords
Introduction
Acute respiratory distress syndrome (ARDS) is the most severe manifestation of acute lung injury (ALI) 1,2 and is associated with high mortality rate. 3–5 Despite better understanding of ARDS pathophysiology, its mechanism is still unclear.
Reactive oxygen species (ROS) are said to play an important role in pulmonary vascular endothelial inflammatory damage, 6 which is thought to be responsible for the development and progression of ARDS. 7 ROS are continuously generated by the body's normal metabolism as well as inflammatory mediators. 8 Increased ROS generation and decreased antioxidant capacity may be involved in ARDS pathogenesis. 9 In addition, an inflammatory process disrupts the alveolarcapillary barrier with interstitial and alveolar edema. 10,11 These effects can severely compromise cell viability or induce a variety of cellular responses through generation of secondary reactive species, ultimately leading to cell death by necrosis or apoptosis. 12,13
The main ARDS supportive treatment, mechanical ventilation (MV), 4 may lead to inflammatory lung injury. It is generally accepted that alveolar stretch induced by either large inspired tidal volumes (V T) or high ventilator pressures, and repeated alveolar collapse and re-expansion (known as atelectrauma) play an important role in the genesis of ventilation-induced lung injury. 14–16 Based on these concepts, conventional protective ventilation has been introduced as a new approach to ventilatory support for ARDS patients. This method aims to protect the lung by limiting V T (6 mL/kg) and providing adequate positive end expiratory pressure (PEEP) with plateau pressure ≤30 cmH2O. 17
High-frequency oscillatory ventilation (HFOV) is an attractive ventilatory method. 18–20 It uses a lower V T (1–3 mL/kg) with a frequency above normal physiological breathing (5–10 Hz), thus avoiding larger alveolar pressure and volume excursions, typical of conventional mechanical ventilation (CMV). In HFOV, a constant mean airway pressure (Paw) is applied to achieve and maintain alveolar recruitment even at end expiration. 21–24
Currently, there is no study available comparing the effect of HFOV and CMV on lung oxidative stress assessed by total antioxidant performance (TAP) assay. TAP assay determining overall antioxidant/oxidative stress can capture the biological antioxidant network between water- and fat-soluble antioxidants and their interactions 25 against oxidative stress. This method has been validated by Beretta et al. 12 and applied to tissues. 26 It is based on a lipophilic radical generator (MeO-AMVN) and a lipophilic oxidizable substrate (BODIPY) that specifically measures the lipid compartment oxidizability related to fat-soluble antioxidants as well as to water-soluble antioxidants acting through a synergistic/cooperative mechanism. 12
The aim of the current study was to compare HFOV with CMV treatment in ALI for antioxidant performance, oxygenation, inflammation and histopathology. The effects of two different ventilatory strategies were determined in an experimental ALI model.
Methods
Design, animals and instrumentation
This was a prospective, randomized, sham-controlled and in vivo animal study. Thirty male Norfolk white rabbits, weighing 2.0–3.0 kg, were anesthetized with ketamine (50 mg/kg intramuscularly) and xylazine (4 mg/kg intramuscularly). Animals were preoxygenated during spontaneous breathing with 100% oxygen by nose catheter. Anesthesia was maintained with continuous intravenous infusion of ketamine (10 mg/kg/h) and xylazine (4 mg/kg/h). Muscle paralysis was induced by intravenous administration of pancuronium bromide (0.2 mg/kg) and maintained with 0.1 mg/kg doses as needed to control minimal respiratory movements and disproportional tachycardia.
A tracheotomy was performed by inserting a tracheal tube (3.0–3.5 mm internal diameter; Portex, Hythe, UK) and securing it in position with umbilical tape. Immediately after tracheotomy, ventilation was initiated with a Galileo Gold ventilator (Hamilton Medical AG, Rhazuns, Sweden) in pressure-regulated-volume control mode with the following initial parameters: FiO2 = 1.0; V T = 6 mL/kg; PEEP = 5 cmH2O; respiratory rate = 40–50 breaths/min. These settings were maintained for 15 min for stabilization. Once tracheotomy had been performed, a vascular catheter was inserted into the common carotid artery (22 Gauge Jelco, Introcan® Safety™; B-Braun, Melsungen, Germany), and a double lumen catheter (5Fr; Arrow International Inc, Reading, PA, USA) was advanced into the superior vena cava through the jugular vein. The arterial catheter was used to assess blood gases and arterial blood pressures using a monitoring system (LogiCal® da Medex, Dublin, OH, USA) connected to a conventional physiological monitor (Dixtal 2010, Manaus, Brazil). The double lumen catheter was used for continuous infusion of sedatives, maintenance fluids and vasoactive drugs.
During the experiment, if mean arterial pressure fell below 50 mmHg, intravenous infusion of noradrenaline (0.5–1 μg/kg/min) was started. The need for inotropic support was measured by using a vasoactive-inotropic score. 27 Maintenance fluid was provided by a continuous infusion of 0.9% saline solution containing 5% dextrose at 4 mL/kg/h. Core temperature was monitored continuously by esophageal probe and body temperature was maintained at 38–39°C with electric warming pads. Continuous pulse oximetry was performed with the probe placed on a shaved portion of the rabbit's thigh.
Rabbits were cared for in accordance with the guidelines by the National Institutes of Health. This study was approved by the Experimental Research and Ethics Committee of Botucatu Medical School – Sao Paulo State University and Jean Mayer USDA – Human Nutrition Research Center on Aging at Tufts University.
Lung injury induction
Lung injury was induced by lung lavage with 30 mL/kg aliquots of 0.9% warm saline solution (38°C) as previously described. 11,15 After stabilization, an arterial blood gas sample was obtained to verify that animals were hypoxemic (two values of partial pressure of oxygen [PaO2] ≤ 200 mmHg 15 min apart). After this stabilization period, animals were subjected to two 30-s dynamic sustained inflations with Paw of 30 cmH2O in order to promote lung recruitment and equalize volume history. 28
Measurement of respiratory system compliance
Static respiratory system compliance was measured automatically by a Galileo Gold ventilator (Hamilton Medical AG) breath by breath using a statistical technique called ‘the least-square fit method’. This method is applied on a breath-by-breath basis, without the need for special inspiratory flow patterns and occlusions maneuvers when the animal and/or patient are relaxed. 29,30
Experimental groups
Animals (n = 30) were randomly assigned to three groups: (a) sham control (CG, n = 10: V T 6 mL/kg, PEEP 5 cmH2O, in the Galileo Gold ventilator [Hamilton Medical AG]); (b) ALI + CMV (CMVG, n = 10: V T 6 mL/kg, PEEP 10 cmH2O, Plato pressure limited to ≤ 30 cmH2O in the same ventilator); or (c) ALI + HFOV (HFG, n = 10: Paw 12–14 cmH2O, respiratory rate [RR] 10 Hz, inspiratory time of 33%, and initial pressure amplitude of 20 cmH2O, in the SensorMedics 3100A ventilator [Viasys Healthcare, Yorba Linda, CA, USA]). In the CMV, pressure-regulated volume control mode, respiratory rate was maintained at 40–50 breaths/min to reach the targeted partial pressure of carbon dioxide (PaCO2; 40–45 mmHg), as pressure amplitude in HFOV was modified to the same PaCO2 level. FiO2 was maintained at 1.0 throughout the experiment for all groups.
Arterial blood gas was obtained before (baseline) and after lung injury induction (lung injury), and every 30 min until completing four hours of observation, and was analyzed by an ABL-3 blood gas analyzer (Chiron RapidLab 865; Bayer Diagnostics, Tarrytown, NY, USA).
Tissue collection
The endotracheal tube was clamped at the PEEP level in use and the thorax was carefully opened to observe for signs of pneumothorax, to confirm proper catheter placement and to harvest tissue. Animals were exsanguinated before lung removal. The heart and lungs were removed en bloc from the thoracic cavity. The right lung in all groups was dissected and stored for oxidative stress analysis. Tissue specimens for oxidative stress study were snap-frozen in liquid nitrogen and stored at −80°C until analysis. In each group the left mainstream bronchus of five rabbits was cannulated and the left lung was lavaged with two 15 mL/kg aliquots of saline. Additionally, left lungs not instrumented for bronchoalveolar lavage were collected from five animals in each group and used for histopathological analysis.
Bronchoalveolar lavage
Bronchoalveolar lavage fluid was collected and total number of cells counted in a hemocytometer chamber. Cells were differentiated using a Panotic staining kit (Laborclin, Pinhais, Brazil) and the percentage of polymorphonuclear leukocytes was assessed.
Histopathological analysis
Lungs were filled with 10% buffered formalin and alveolar architecture preserved by slow gravity formalin drip at a maximum pressure of 30 cmH2O. After at least a 48-h fixation, fragments were embedded in paraffin and axial lung sections made, stained with hematoxylin and eosin, and blindly examined by two independent pathologists. Ten microscopic fields were randomly selected for examination of each slide, totaling 20 tests for each animal. Pulmonary histological damage was quantified by a score using seven variables (alveolar and interstitial inflammation, alveolar and interstitial hemorrhage, edema, atelectasis and necrosis). Injury severity was graded for each of the seven variables as follows: no injury = 0, injury to 25% of the field = 1, injury to 50% of the field = 2, injury to 75% of the field = 3, diffuse injury = 4. The maximum possible score was 28 and the lowest zero. 31,32
TAP analysis in lung tissue
TAP assay was used to measure oxidative stress status of rabbit lung from all groups. TAP in rabbit lung tissue was quantified by comparing the area under the curve relative to the oxidation kinetics of phosphatidylcholine liposome suspension used as the reference biological matrix. The antioxidant performance ranges from 0% (no protection) to 100% (total protection).
12
Liposomes for control were prepared as previously validated and reported by Ferreira et al.
26
in animal tissue. The dorsal portion of the right lung was weighed (0.4 g), minced and homogenized for 20 s on ice with 2 mL of phosphate buffer saline (100 mmol/L, pH 7.4) using an IKA Ultra-Turrax T8 homogenizer (Wilmington, NC, USA). Aliquots of supernatant were collected after centrifugation of lung tissue homogenate at 800
Statistical analysis
Data were analyzed by SigmaStat (version 2.03; SPSS Inc, Chicago, IL, USA). Normally distributed data were compared between the different treatment groups by one-way analysis of variance with all pairwise comparison procedures (Student–Newman–Keuls test) and expressed as mean ± SD. Data showing non-normal distribution were compared by Kruskal–Wallis one-way analysis of variance on ranks with all pairwise comparisons by Dunn's test and expressed as median (range). Intragroup comparisons at different time points were performed using Friedman's repeated measures analysis of variance on ranks with all pairwise multiple comparison procedures by Dunnett's method. Contingency tables of categorical data were compared by Fisher's exact test. Statistical significance was defined as P < 0.05.
Results
There was no statistical difference between groups for weight (CG: 2.65 ± 0.24 = CMVG: 2.41 ± 0.28 = HFG: 2.59 ± 0.16 kg; P > 0.05) and number of lung lavages to induce ALI (CMVG: 8.1 ± 2.72 = HFG: 7.2 ± 2.53; P > 0.05). Percentages of fluid recovered from the lavaged lungs were 85% and 83.2% for CMV and HFOV groups (P > 0.05), respectively.
One animal from the sham control group (refractory hypotension), two from the CMV group (pneumothorax and tracheal bleeding) and one from the HFOV group (refractory hypotension) died. These animals were not included and analyzed.
Hemodynamic, lung mechanics and gas exchange
There was no statistical difference in mean arterial pressure among groups. Animals from ALI groups required noradrenaline to maintain mean arterial pressure above 50 mmHg. Both injured groups were greater than sham control for vasoactive-inotropic score (CG: 0 [0–25] < CMVG: 50 [0–70] = HFG: 50 [0–50]; P < 0.05).
ALI groups showed significant hypoxemia and poorer ventilation after lung injury than baseline and the sham control group. There was significant increase in Paw and decrease in respiratory system compliance after lung injury induction (Table 1) lasting until the end of the experiment. Mean airway pressure and respiratory system compliance are shown in Figures 1 and 2, respectively.
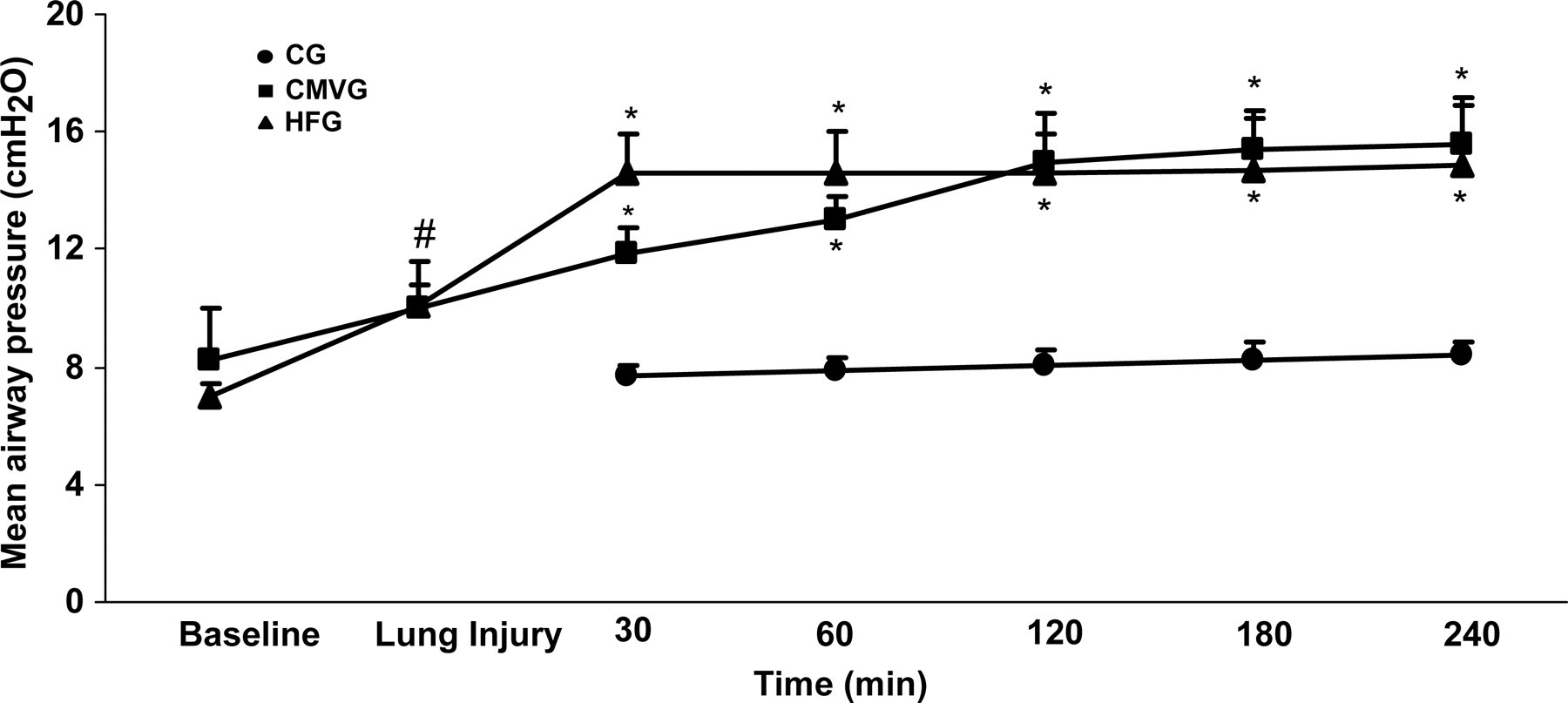
Mean airway pressure over time for the experimental groups. Data are shown as mean ± SD. *P < 0.05 versus sham control group (CG) and # P < 0.05 versus baseline. CMVG, conventional mechanical ventilation group; HFG, high-frequency oscillatory ventilation group
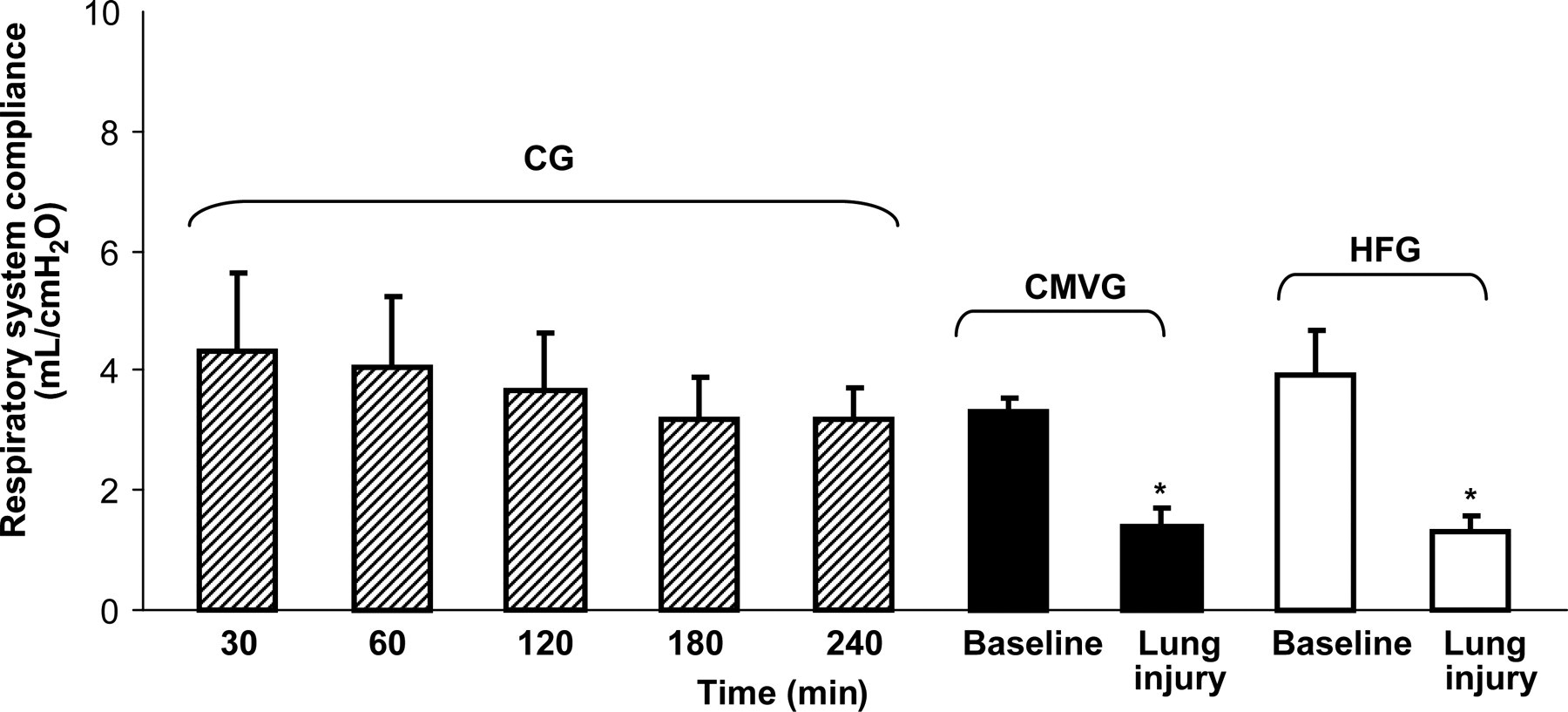
Respiratory system compliance on sham control group (CG), conventional mechanical ventilation group (CMVG) and high-frequency ventilation group (HFG). Data are shown as mean ± SD. *P < 0.05 versus CG and baseline
Oxygenation indexes, pulmonary mechanics and hemodynamic data at baseline and lung injury (mean ± SD)
PaO2, partial pressure of oxygen; PaCO2, partial pressure of carbon dioxide; n, animals; baseline, before lung injury induction; lung injury, right after lung injury induction; CMVG, conventional mechanical ventilation group; HFG, high-frequency oscillatory ventilation group. Oxygenation index = ([FiO2 ×mean airway pressure]/PaO2) × 100
*P < 0.05 comparing lung injury and baseline for each group
† P > 0.05 comparing groups in each moment. One-way repeated measures analysis of variance (Bonferroni test)
After four hours of MV, the HFOV group showed a significant improvement in oxygenation over the CMV group, presenting oxygenation indexes similar to baseline and the sham control group. Values of PaO2 and oxygenation index (oxygenation index: mean airway pressure x FiO2 × 100/PaO2; cmH2O/mmHg) are shown in Figure 3.
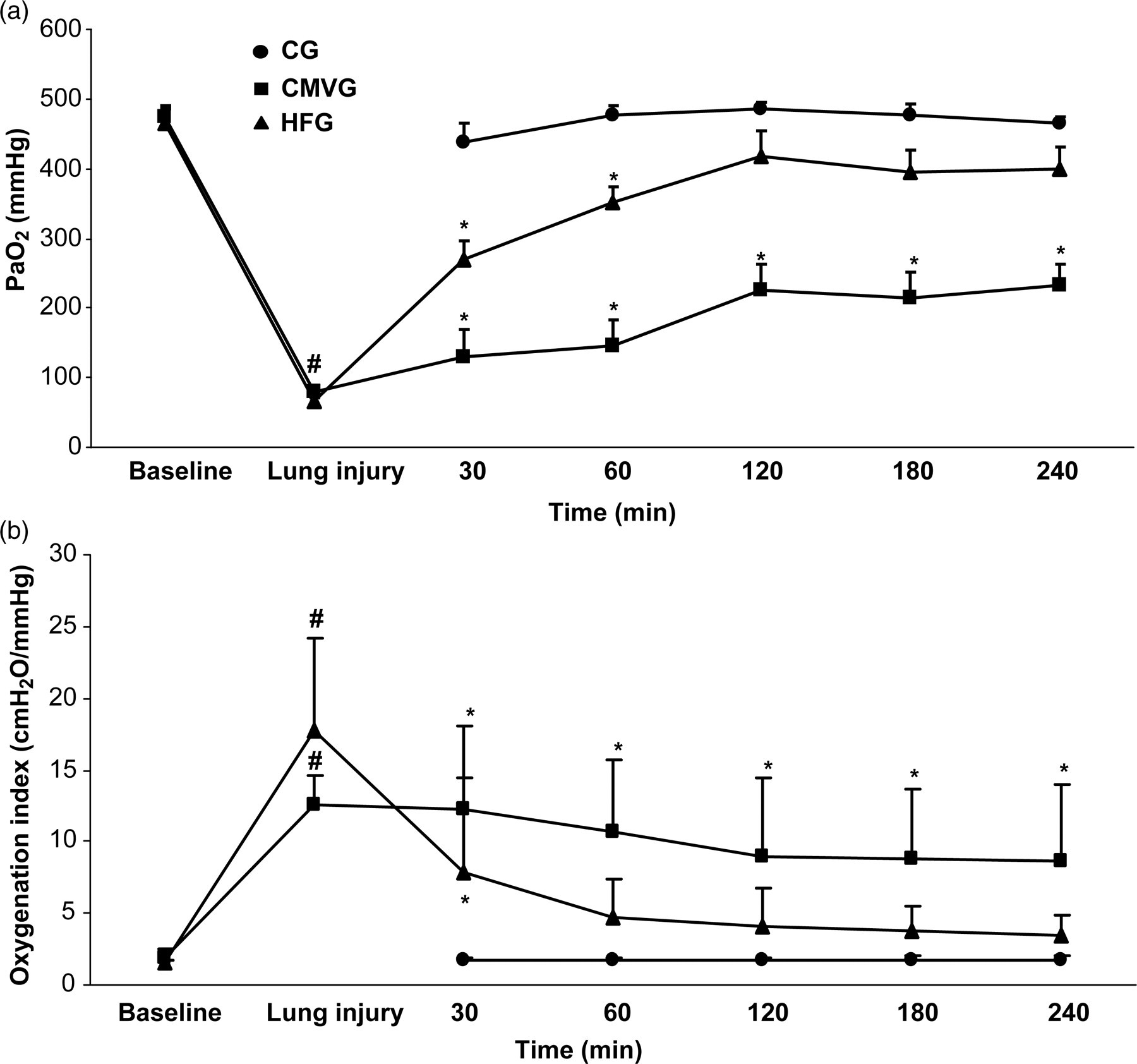
PaO2 over time for the experimental groups (a). Data are shown as mean ± SD.
Oxidative injury
TAP in lung tissue from the HFOV group was similar to the sham control group and significantly higher than the CMV group (CG: 59.4 ± 4.52 = HFG: 69.0 ± 4.99 > CMVG: 47.6 ± 2.58 percentage of protection/g protein; P < 0.05) (Figure 4).
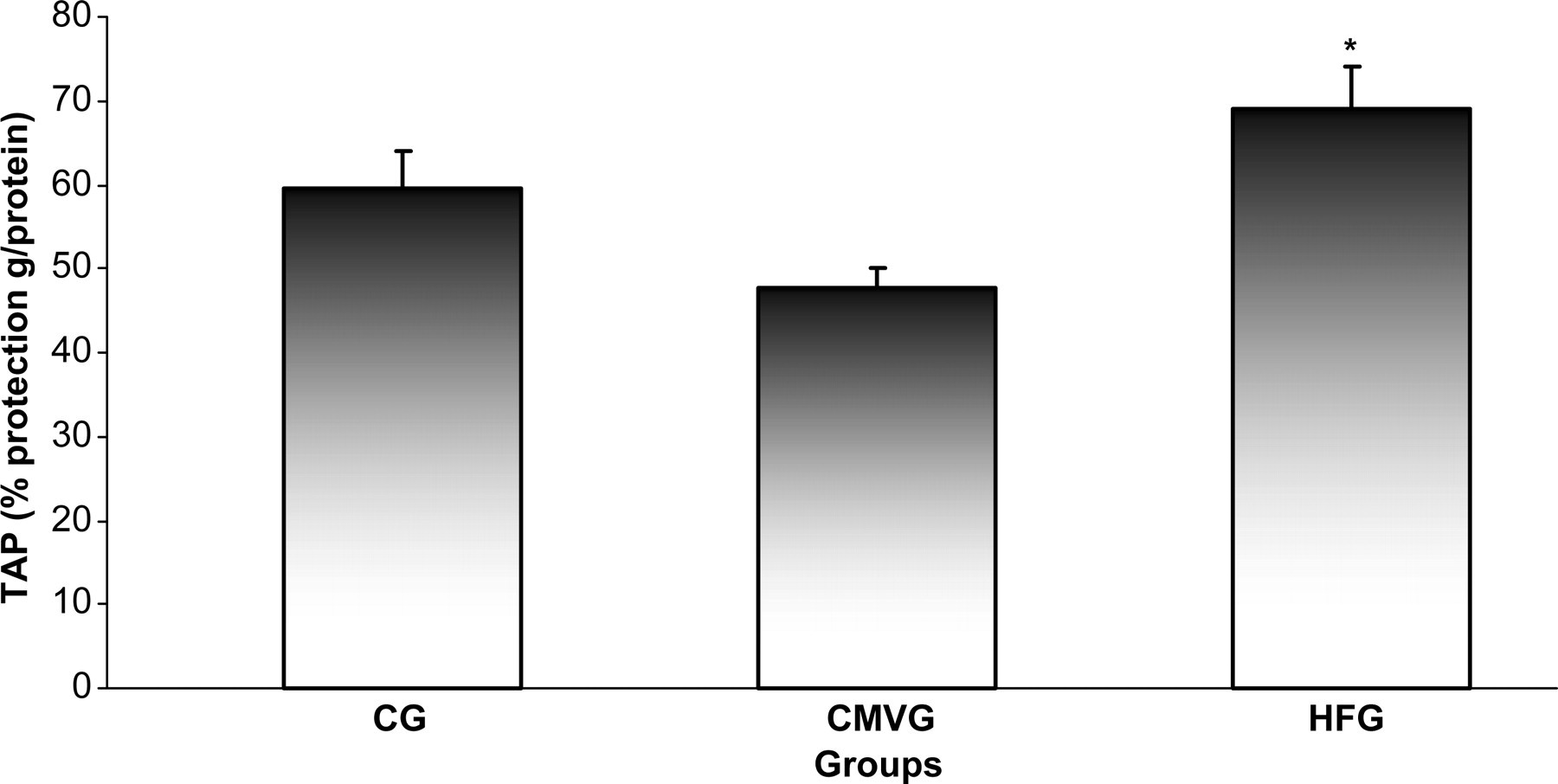
Lung protection by total antioxidant performance (TAP) assay for the experimental groups. Data are shown as mean ± SD. *P < 0.05 versus protective conventional mechanical ventilation group. CG, sham control group; CMVG, conventional mechanical ventilation group; HFG, high-frequency oscillatory ventilation group
Histopathology
The HFOV group showed a reduced histopathological injury score against the CMV group (CMVG: 5 (2–16) > HFG: 2 (0–5) > CG: 1 (0–2); P < 0.05) (Figure 5).
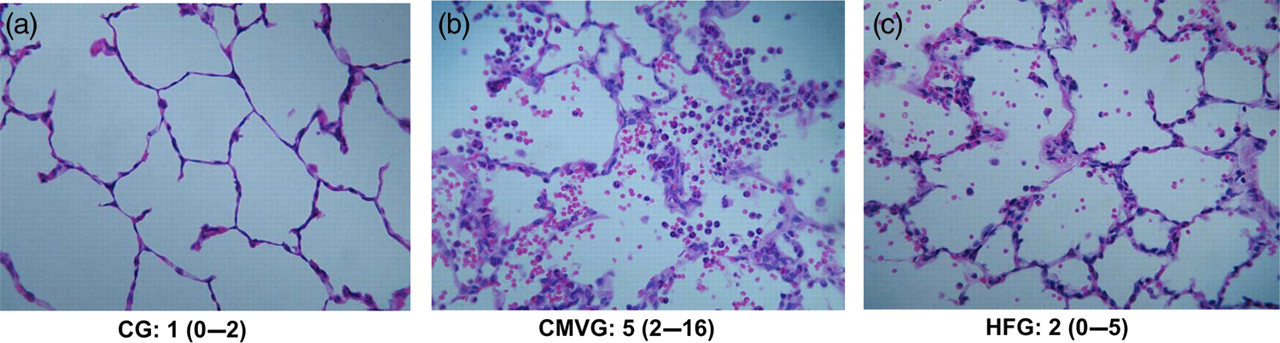
Optical microscopy digital photomicrographs (×200, hematoxylin and eosin) of representative samples of lung dependent areas from the sham control group (CG), conventional mechanical ventilation group (CMVG) and high-frequency ventilation group (HFG). Histopathological injury score: CMVG > HFG > CG, P < 0.05. Data are shown as median (range). Kruskal–Wallis analysis of variance, with subsequent comparisons by the Dunn test. (A color version of this figure is available in the online journal)
Polymorphonuclear counting
Recovered polymorphonuclear leukocytes cells from bronchoalveolar lavaged fluid were lower in the HFOV group than in the CMV group and similar to the sham control group (CMVG: 4.27 ± 1.50 > HFG: 0.33 ± 0.20 = CG: 0.16 ± 0.15; number of polymorphonuclear leukocytes cells/bronchoalveolar lavage fluid per lung, P < 0.05) (Figure 6).
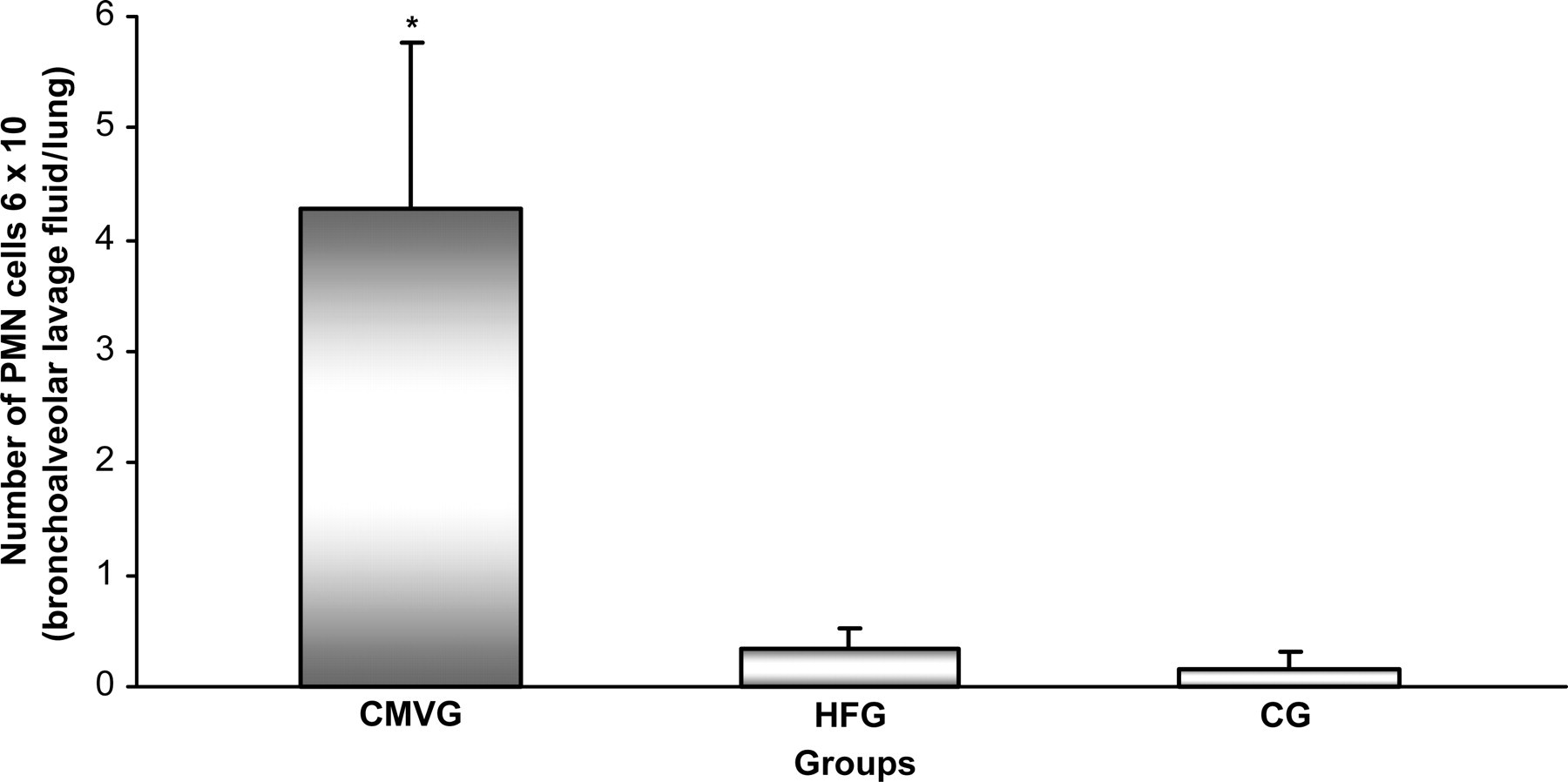
Number of polymorphonuclear leukocyte (PMN) cells recovered from bronchoalveolar lavage fluid at the end of experiment of the sham control group (CG), conventional mechanical ventilation group (CMVG) and high-frequency ventilation group (HFG): CMVG: 4.27 ± 1.50 > HFG: 0.33 ± 0.20 = CG: 0.16 ± 0.15, P < 0.05. Data are shown as mean ± SD. *P < 0.05 versus CG and HFG
Discussion
The benefit of MV at lower V T as a lung protective strategy has been reported in a large, multicenter, randomized, clinical trial. 17 Patients with ALI or ARDS ventilated at 6 mL/kg V T had a significant reduction in mortality compared with those ventilated at higher traditional V T. This concept leads to an interest in HFOV 24 as it uses a very small V T and constant Paw with greater pulmonary stability. Overdistension caused by increased airway pressure in CMV can be avoided when HFOV is used, preventing alveolar derecruitment and oscillations in alveolar volume (collapse and re-expansion), saving surfactant and decreasing local inflammation. 34
HFOV has shown consistent beneficial results in clinical and experimental ARDS. 11,15,24,35 In accordance with previous reports, our study confirmed that HFOV improved oxygenation, and reduced inflammatory and histopathological injuries. 11,15,35–37 Recently, Jian et al. 38 showed reduced inflammatory responses measured by tumor necrosis factor-alpha (TNF-α) production and neutrophil infiltration in bronchoalveolar lavage fluid in a rat model of ALI. Our ALI groups exhibited significant hypoxemia after lung lavage and prompt recovery by HFOV. Similar results have been observed by others. 11,17,34,39
While there are many studies evaluating the effects of HFOV on oxygenation, lung inflammation and histological injury in animal ALI models, only a few have analyzed oxidative stress. 11,18 Furthermore, to our knowledge, there is no study available on the effects of HFOV on lung oxidative status determined by TAP assay in pulmonary tissue. The TAP assay is a unique method of determining the antioxidant capacity of both lipophilic and hydrophilic compartments of a biological system. 12 The involvement of oxidant-mediated tissue injury is likely to be an important event in ARDS pathogenesis 40 and ARDS patients are reported to have low plasma concentrations of antioxidants. 41 Activated leukocyte aggregates in pulmonary microvasculature release ROS, which can attack membrane polyunsaturated fatty acid, thus initiating a peroxidation process. Peroxidation leads to the loss of cell membrane functional integrity, culminating in an acute increase of alveolar-capillary permeability. In ALI, activated lymphocytes stimulate TNF and other cytokines. These lymphokines augment free radical generation by polymorphonuclear leukocytes, macrophages and other cells, which may ultimately lead to ARDS. 42
Rotta et al., 11 in a similar model of ALI in rabbits, studied oxidative stress by measuring malondialdehyde, which is a non-specific biomarker of lipid peroxidation. 43 Although HFOV did show lower lipid peroxidation than CMV, this conventional assay has been criticized due to its low specificity and sensitivity. 44,45 Using another oxidative stress marker (myeloperoxidase), authors showed reduced lung oxidative damage in HFOV in a rabbit model of gastric juice aspiration. 18 Even though myeloperoxidase has been reportedly associated with tissue damage involving inflammatory cells, it only implicates oxidant activity of neutrophils and other myeloperoxidase-containing cells. 46
Control group (MV without lung injury) showed similar TAP values compared with HFG, suggesting that MV per se induced lung oxidative stress probably by repeated alveolar open/close cycles. Indeed, previous reports have stated that MV alone can induce lung injury very similar to human ARDS. 47,48
As expected, animals submitted to CMV and lung injury exhibited lower TAP than controls, indicating greater oxidative stress, probably due to the alveolar cyclic stretch or reduction in the mechanism of ventilator lung injury from exhalation to low volumes and pressures. It was interesting to note that HFOV with lung injury showed a significantly higher TAP value than CMV with lung injury, suggesting a substantial reduction in oxidative stress with HFOV. These findings could be explained by the differences in the lung injury animal models. Ideally, animal ALI models should reproduce human ALI mechanisms and consequences, including physiological and pathological changes. However, no single animal model reproduces all the characteristics of ALI/ARDS in humans. 47 Rabbits, for instance, have a 57% similarity with the human TLR4 hypervariable region but are also associated with double the nitric oxide production of human ALI. 47
Currently, one of the most commonly used animal ALI models is alveolar lavage with warmed normal saline. 47 This is primarily a surfactant depletion model, which causes a lung injury very similar to human ARDS in its effects on oxygenation, respiratory system compliance, atelectasis and edema perivascular/peribronchial. However, it induces less macrophage and neutrophil infiltration, unless another injury such as MV is added. 47 Additionally, surfactant removal can interfere with lung inflammatory/immune response and oxidative metabolism, as surfactant inhibits respiratory activation of neutrophils and has an antioxidant effect on alveolar macrophages. 49
Based on the pathophysiological and biochemical indexes which we have analyzed, it is noted that HFOV improved oxygenation and reduced histopathological damage. Therefore, we can hypothesize that HFOV induced lower alveolar stretch limiting both lung inflammatory and oxidative stress response.
Study limitations and future implications
Firstly, no single animal model can reproduce all the characteristics of ALI/ARDS in humans. In addition, 1.0 FiO2 during four hours may lead to lung parenchyma damage and interfere with oxidative metabolism. However, we used the same concentration of oxygen for all groups, which probably excluded any major variation among groups due to oxygen toxicity. Surfactant removal, characteristic of the model used, can interfere with lung inflammatory/immune response and oxidative metabolism because surfactant inhibits neutrophil respiratory activation and has an antioxidant effect on alveolar macrophages. 49 Secondly, we did not allow changes in ventilator settings (raise PEEP levels above 10 cmH2O) which may have contributed to sustained hypoxia. However, ALI rabbit models are all very sensitive to hypotension, making it difficult to use PEEP at the higher levels as used in ARDS patients.
Despite favorable experimental results, there are no clinical studies reporting significant reduction of mortality rate in ARDS patients submitted to HFOV. It would be very difficult to find a single therapy for ARDS management due to its pathophysiological complexity. Therefore, more studies are needed to evaluate the mechanisms of pulmonary tissue oxidative damage in ARDS using different ventilatory strategies and other adjuvant therapies, such as prone positioning, surfactant and inhaled nitric oxide. Evaluation of overall antioxidant/oxidative stress by TAP assay in patients with ARDS may provide useful information on antioxidant supplementation needs, which warrants further study.
Conclusions
The present study showed that HFOV had an important protective role in ALI. It improved oxygenation, reduced the inflammatory process and histopathological damage, and attenuated oxidative lung injury compared with protective CMV under these experimental conditions considering the study limitations.
Footnotes
ACKNOWLEDGEMENTS
This study was supported in part by Fundação de Amparo à Pesquisa do Estado de São Paulo, FAPESP, São Paulo, SP, Brazil (process number: 2008/08199-2) and by a grant from the US Department of Agriculture, Agricultural Research Service under Cooperative Agreement (USDA: 1950-51000-065-08S). We thank the Experimental Laboratory of Pediatrics Department – UNESP and Carotenoids & Health Laboratory at Human Nutrition Research Center on Aging – Tufts University staff for their assistance and Colin E Knaggs for text revision. Any opinions, findings, conclusion or recommendations expressed in this publication are those of the author(s) and do not necessarily reflect the view of the UNESP or US Department of Agriculture.