
Abstract
A major problem associated with diabetes is the complication of chronic non-healing wounds that can lead to the formation of debilitating ulcers, and can progress to more serious problems including amputation. There is no fully effective prevention of these complications, constituting an unmet medical need to understand the pathophysiology and treatment of wound healing in diabetes. This study determined whether blockade of opioid receptors from opioid peptides, known to inhibit cell proliferation and be overexpressed in diabetes, by topical application of the opioid antagonist naltrexone (NTX) reverses delays in wound closure. Rats with streptozotocin-induced type 1 diabetes (T1D) received topical applications of NTX (10−4–10−6 mol/L) or vehicle in a variety of carriers; DNA synthesis was evaluated 12 h later. DNA synthesis in the epithelium of T1D rats was significantly reduced from normal animals. Both systemic and topical application of NTX increased DNA synthesis (up to 2-fold higher) within 12 h of administration. In a second study, diabetic and normal rats received full-thickness cutaneous wounds and were treated three times daily with either 10−5 mol/L NTX or vehicle in topical carriers. Wound sizes were analyzed, and BrdU (5-bromo-2′-deoxyuridine) labeling in the skin was evaluated to determine DNA synthesis. Application of NTX in a variety of carriers to rats with full-thickness wounds resulted in significantly smaller wound areas relative to T1D animals receiving vehicle, and comparable to that of normal rats. Wound contraction in T1D animals was 50% of that in normal rats, with NTX-treated wounds restoring wound contraction to that of normal cohorts. DNA synthesis was also enhanced in NTX-treated T1D animals compared with T1D vehicle controls. These data suggest that topical application of NTX is a non-toxic and efficacious facilitator for healing full thickness wounds in T1D, with wound contraction serving as a particular target of NTX action.
Introduction
Impaired wound healing is a major complication of diabetes that can result in the formation of chronic debilitating ulcers. 1–3 Diabetes is the leading cause of amputations, 2,3 accounting for over 50% of patients having lower extremity amputations annually. With the number of diabetic patients estimated to reach 300 million worldwide by the year 2030, the burden of diabetic wounds and their complications is expected to rise simultaneously. 2 Although continuing medical care and patient self-management reduce the risk of long-term complications, and despite the availability of numerous dressing products, there is no fully effective prevention or treatment of these complications. Hence, there is an urgent need to understand the pathophysiology underlying wound healing in diabetes, and to translate this knowledge into treatment modalities in order to prevent or at least attenuate acute and chronic wound healing complications. 4
Initially studied for their role as neurotransmitters, 5 endogenous opioids have been shown to be present in neural and non-neural tissues, and to mediate a number of functions other than neuromodulation, including cell proliferation, angiogenesis, tissue organization, cell migration and immunity. 6–12 The relationship of native opioids to diabetes has received some attention. Studies concerned with circulating opioid levels in diabetes have shown that patients with type 1 diabetes (T1D) have high plasma [Met5]-enkephalin concentrations. 13–15 Elevated levels of [Met5]-enkephalin also have been reported in the plasma of genetically obese diabetic (db/db) mice. 16,17
A series of studies using systemic and topical applications of the opioid antagonist naltrexone (NTX) in rats with T1D reported delays in re-epithelialization following removal of ocular surface epithelium that were reversed by NTX and related to an increase in DNA synthesis. 7,18 These data suggest that dysfunctional ocular wound repair in T1D was due to an increase in opioid peptide–opioid receptor interactions that were disrupted by NTX. At least one opioid peptide, the opioid growth factor (OGF; chemical term = [Met5]-enkephalin) is known to suppress wound closure in the human cornea 19 and rat tail skin. 12
Endogenous opioids, and classical and non-classical opioid receptors, are present in the skin. 20–29 OGF is known to regulate DNA synthesis and cellular renewal of the stratum corneum, 21 whereas deletion of the δ opioid receptor in mice alters skin differentiation and delays wound healing. 23 Given that NTX can re-establish the processes of corneal epithelial wound healing, and that opioid peptides and opioid receptors are present in the skin, this study was designed to test the hypothesis that a topical dressing of NTX could facilitate full-thickness cutaneous wound repair in animals with streptozotocin (STZ)-induced T1D.
Materials and methods
Animals and induction of diabetes
Male Sprague-Dawley rats (∼150 g) were purchased from Charles River Laboratories (Wilmington, MA, USA), and housed under standard laboratory conditions; water and food were available ad libitum. All investigations conformed to the guidelines of The Pennsylvania State University College of Medicine Institutional Animal Care and Use Committee.
T1D was induced by intraperitoneal injections of 40 mg/kg STZ (Sigma, St Louis, MO, USA), on two consecutive days. 18,30 This regimen produced insulin-dependent diabetes in 100% of the animals within 72–96 h; rats with blood glucose concentrations measuring >350 mg/dL were considered diabetic (DB). Blood glucose concentrations were monitored from the tail vein using a True Track® Smart System glucometer (Home Diagnostics, Fort Lauderdale, FL, USA) before receiving STZ, and at one, four and eight weeks following induction of hyperglycemia. Control animals receiving an injection of an equivalent volume of sterile saline were termed Normal. All rats were weighed weekly.
Experiment I – NTX and unwounded skin
NTX application
Normal (n = 24) and DB rats (n = 24) were randomized eight weeks after injections of STZ or saline, and received NTX (Sigma-Aldrich, Indianapolis, IN, USA) systemically (30 mg/kg, intraperitoneal or subcutaneous at 08:00 h) or topically three times daily at 07:00, 12:00 and 17:00 h. For topical applications, NTX was dissolved in Sorenson's phosphate buffer (SPB), KY jelly (KYJ) (K-Y; Personal Products Company, McNeil-PPC, Inc, Skillman, NJ, USA), Neutrogena moisturizing cream (MCN; Neutrogena Corporation, Los Angeles, CA, USA) or dimethyl sulfoxide (VWR, Philadelphia, PA, USA). NTX was dissolved in sterile water at dosages of 10−4, 10−5 or 10−6 mol/L, and thoroughly mixed into each of the carriers (1:1, v/v); 0.5 mL of saline mixed into corresponding carriers served as the respective vehicle control.
On the day preceding NTX or vehicle treatment, an 8 × 8 cm area was shaved on the dorsal surface of each rat and four circles (approximately 20 mm in diameter) were made with a permanent marker to denote locations of subsequent topical applications and/or skin collection. Using an applicator stick, 0.1 mL of carrier containing NTX or vehicle was placed within the demarked areas. Applications of NTX formulations were randomized to different positions. Each animal received NTX in three different concentrations, as well as the vehicle, in the same carrier; some rats received only saline in a carrier or were untreated.
DNA synthesis
To assess cells undergoing DNA synthesis, rats were injected intraperitoneally with 100 mg/kg BrdU (5-bromo-2'-deoxyuridine) (Sigma-Aldrich) three and six hours before euthanasia with Euthasol (Virbac, Fort Worth, TX, USA). Appropriate regions of the skin were removed, fixed in 10% buffered formalin and paraffin sections (6 μm) stained with anti-BrdU-POD (Invitrogen, Carlsbad, CA, USA). BrdU-stained cells in the basal layer of the epithelium were counted in four 0.1-mm grids at ×250 magnification using two sections/specimen; three tissue specimens were analyzed for each dosage of NTX in each carrier.
Experiment II – NTX and wound healing
Full-thickness cutaneous wounds
In a second set of experiments, Normal (n = 70) and DB (n = 70) Sprague-Dawley rats, 12–14 weeks of age and eight weeks after injection of STZ, were subjected to wounding. Eight rats/treatment regimen were evaluated over the course of three independent experiments. The dorsum of the rat was shaved, and areas (20 mm in diameter) outlined with a marker in order to consistently position the wounds. Animals were anesthetized by intraperitoneal injection of ketamine (60 mg/kg), xylazine (10 mg/kg) and acepromazine (1 mg/kg), and a 6-mm full-thickness circular excisional skin wound was made in the center of the demarked area to the level of the panniculus muscle using an Acupunch (Acuderm Inc, Fort Lauderdale, FL, USA). Three wounds per rat were standardized such that the first wound was made 5 cm posterior to the occipital notch at the posterior of the animal's cranium and 1 cm off the midline. The second wound was created 7 cm posterior to the occipital notch at the posterior of the animal's cranium and 1 cm off the midline on the opposite side from the first wound. The third wound was placed 9 cm posterior to the occipital notch at the base of the animal's cranium and 1 cm off the midline on the same side as the first wound. To minimize the effects of diurnal rhythm, surgery was performed between 08:00 and 09:00 h. All wounds were left uncovered.
Topical administration of ∼0.1 mL of the carrier containing NTX or vehicle, using the dosage and carriers selected from the first experiment, was initiated immediately after wounding (08:00 h for those rats receiving agents only once per day, and at 08:00, 12:00 and 16:00 h for those animals receiving three applications daily); control rats received the carrier with vehicle either once or three times daily. Some animals in the Normal and DB groups were wounded but untreated.
Photography
Wound size was monitored by capturing images with a digital camera mounted on a tripod set 20 cm from the surface; a ruler was photographed with each wound. Animals were manually restrained without anesthesia for photography. Photographs were taken immediately after surgery and on days 3, 5, 7, 9 and 11. The area of each wound was analyzed using Image ProPlus 6.2 (Media Cybernetics, Inc, Bethesda, MD, USA). The percent residual wound was calculated at each time point for every rat. At eight days, wound closure also was quantified according to Pietramaggiori and colleagues 31 by measuring contraction, re-epithelialization and open wound as a percentage of the original wound area. The sum of contracted, re-epithelialized and open wound area was defined as equaling 100% of the original wound size. 32
DNA synthesis and histopathology
Cell proliferation was evaluated with BrdU on days 5 and 10 postwounding as described above. The number of labeled and unlabeled cells in the basal layer of the epithelium was counted in four 0.1-mm grids at ×250 magnification, and sampled from regions adjacent, and 0.5 mm peripheral, to the edge of the wound site. Three Normal and three DB rats receiving MCN + vehicle or MCN + NTX three times daily were injected with BrdU.
On day 20 following creation of the wound, some rats were euthanized and the original wound areas as well as tissue peripheral to the wound that encompassed the 20-mm diameter circle were excised and fixed in 10% neutral buffered formalin. Tissues were processed for paraffin embedding; sections were stained with hematoxylin and eosin. The thickness of the epithelium covering the granulation tissue was measured with an ocular micrometer. Five measures/section from seven to eight wounds/treatment group were evaluated at ×250 magnification.
Data analysis
Body weights and glucose measurements were analyzed with Student's two-tailed t-test. Areal measurements of defects (e.g. percent residual wound, contraction), thickness of the epithelium and DNA labeling indexes were evaluated using analysis of variance (ANOVA) with subsequent planned comparisons made utilizing Newman–Keuls tests.
Results
Experiment I – NTX and unwounded skin
All rats were hyperglycemic within 72 h of STZ injection, with blood glucose concentrations for Normal and DB animals being 119 ± 4 and 569 ± 9 mg/dL, respectively (Figure 1). The body weights of DB rats were reduced by 8–28% from Normal cohorts beginning one week after STZ injection and continuing throughout the experimental period (Figure 1). Rats in the DB group were not provided with insulin. No animals died from hyperglycemia.

Body weights (a) and glucose concentrations (b) of rats rendered diabetic with streptozotocin (STZ) (DB) or those untreated receiving saline (Normal). (a) Body weights were recorded prior to STZ injection (week 0) and weekly thereafter. (b) Blood glucose concentrations were recorded before (week 0) and at one, four and eight weeks after STZ administration. Values represent means ± SEM for at least five animals/group at each time point. Significantly different from Normal at **P < 0.01 and ***P < 0.001
Relative to the BrdU labeling index of 8.1 ± 0.3% in basal cells of the cutaneous epithelium of Normal rats, systemic injections of 30 mg/kg NTX by the intraperitoneal or subcutaneous routes elevated BrdU labeling by 172% and 51%, respectively. With respect to a labeling index of 8.1 ± 0.5% in the skin of animals with DB, intraperitoneal and subcutaneous injections of NTX increased BrdU incorporation by 181% and 59%, respectively.
The effects of topical application of NTX (10−4 to 10−6 mol/L) dissolved in four different carriers that had different properties (e.g. absorption, density) were examined in Normal and DB rats (Figure 2). Topical NTX dissolved in any of the four carriers consistently elevated (43–132%) DNA synthesis from baseline levels in Normal animals. Animals receiving NTX in SPB displayed the lowest level of increase in BrdU incorporation in the skin (43–56%) compared with baseline values, whereas rats treated with different dosages of NTX in MCN exhibited some of the greatest changes from baseline (73–132%). In the DB rats, topical exposure to NTX at all three dosages markedly elevated labeling indexes from baseline levels when delivered in KYJ (103–147%) or MCN (85–89%). NTX at concentrations of 10−4 and 10−5 mol/L delivered in SPB to DB rats had no effect on BrdU incorporation. The opioid antagonist combined with dimethyl sulfoxide only was efficacious at concentrations of 10−4 and 10−5 mol/L.

Histograms of the labeling indexes in stratum basale on the dorsum of rats topically treated with naltrexone (NTX) (10−4, 10−5 or 10−6 mol/L) dissolved in Sorenson's phosphate buffer (SPB), dimethyl sulfoxide (DMSO), KY Jelly (KYJ) or Neutrogena moisturizing cream (MCN); control rats received the corresponding vehicle (Vehicle). Animals received three topical applications of NTX. At three and six hours before euthanasia, animals received injections of BrdU (5-bromo-2'-deoxyuridine) (100 mg/kg; intraperitoneal). Two-way analysis of variance (ANOVA) for treatment (four carriers and four concentrations/carrier) and condition (diabetic, Normal) was performed. There was no overall effect for condition; treatment was significant at P < 0.001, F = 5.59 (15, 288). Data represent means ± SEM. Based on one-way ANOVA for each carrier and condition, significantly different from respective values for vehicle-treated rats at *P < 0.05, **P < 0.01 and ***P < 0.001
To examine whether topical application of NTX had systemic ramifications, some rats were treated with MCN + NTX (10−5 mol/L) or MCN + vehicle at different positions on their dorsum. The skin treated with MCN + NTX had a labeling index of 18.0 ± 0.9% compared with 8.1 ± 0.7% for wounds on the same animal receiving MCN + vehicle; the basal epithelium of separate, untreated rats had a labeling index of 8.2 ± 0.5%.
Examination of the skin, both grossly and by histological measures, revealed a similar appearance in Normal and DB rats receiving vehicle or any dosage of NTX in any carrier. The morphology of the treated skin was comparable to that in animals not exposed to any agent (Figure 3).

Histological preparations of dorsal skin from Normal and Diabetic rats subjected to 10−5 mol/L naltrexone (NTX) in Neutrogena moisturizing cream (MCN + NTX), moisturizing cream only (MCN + Vehicle) or no treatment. Sections were stained with anti-BrdU (5-bromo-2'-deoxyuridine) antibodies and counterstained with hematoxylin. Note increases in BrdU-positive cells in the NTX-treated groups. bl, basal layer; epi, epidermis; de, dermis. Arrow indicates BrdU-positive cell. Bar = 12 μm. (A color version of this figure is available in the online journal)
Experiment II – NTX and full-thickness wounds
Based on the labeling index data from the first experiment, NTX at 10−5 mol/L applied in two topical delivery systems, KYJ and MCN, was chosen for subsequent experiments examining the effects of opioid antagonist blockade on full-thickness wound healing. Normal and DB rats expressed body weight and glucose patterns similar to those in Figure 1. All rats tolerated the wounding procedure without problems (e.g. normal food consumption).
Normal and diabetic wound healing
Using a 6-mm trephine, the calculated wound size was 28.3 mm2, and wounds that deviated more than 10% were not included for analysis. Evaluation of wound closure in Normal and DB rats revealed that the area of residual wound in DB animals was 24%, 44% and 132% greater on days 5, 7 and 9 following surgery relative to those of Normal rats (Figure 5a).
Number of applications of NTX and efficacy of wound healing
To examine the effects of topical application of NTX on the healing of full-thickness wounds in Normal and DB rats, an investigation was initiated to study whether the number of daily applications of NTX was critical (Figures 4 and 5). Within three days of a single or three times daily regimen of 10−5 mol/L NTX in MCN to Normal rats, wound areas were reduced 30% and 11%, respectively, relative to that of animals receiving MCN + vehicle (Figure 5b). Wound sizes on days 3, 5, 7 and 9 in NTX-treated Normal animals were smaller than in cohorts receiving MCN + vehicle, with reductions ranging from 31% to 82% and 11% to 23% for the one and three times daily regimens, respectively; all data were statistically significant except for the value for the three times daily group on day 9. DB animals subjected to once daily application of MCN + NTX also had a decrease in wound size compared with DB rats exposed to vehicle, but with only 32% and 42% reductions recorded on days 5 and 7, respectively. However, in regard to the DB animals, MCN + NTX given three times daily consistently accelerated wound closure, with this group displaying mean residual wounds that were reduced 13% to 57% from DB rats treated with MCN + vehicle.
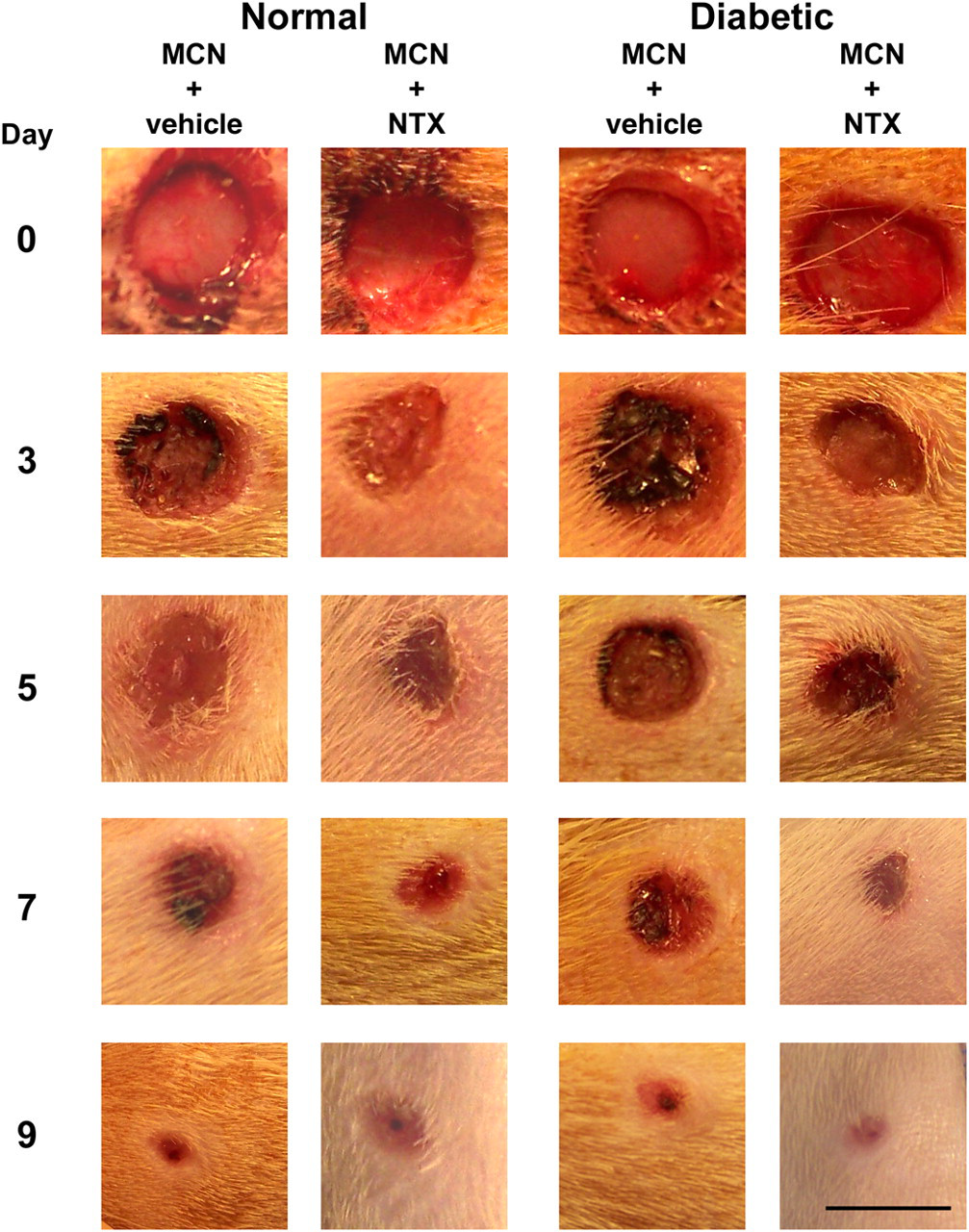
Photomicrographs of full-thickness wounds created on the dorsal surface of Normal and Diabetic rats. Wounds were treated three times daily with either 10−5 mol/L naltrexone (NTX) dissolved in Neutrogena moisturizing cream (MCN + NTX) or moisturizing cream alone (MCN + Vehicle) and photographed on days 0, 3, 5, 7 and 9 following wounding. Bar = 6 mm. (A color version of this figure is available in the online journal)

Histograms of residual defects (%) in rat skin after formation of 6-mm wounds and followed for nine days. (a) Normal and Diabetic (DB) rats receiving no treatment. (b) Normal and Diabetic rats treated one time (1×) or three times (3×) daily with 10−5 mol/L naltrexone (NTX) dissolved in Neutrogena moisturizing cream (MCN + NTX 1×; MCN + NTX 3×) or receiving vehicle alone (MCN + Vehicle 1×; MCN + Vehicle 3×). (c) The contribution of contraction and re-epithelialization to wound closure at eight days in DB and Normal (N) rats treated with MCN + NTX or MCN + Vehicle. Values represent means ± SEM. Significantly different from Normal or MCN + Vehicle at *P < 0.05, **P < 0.01 and ***P < 0.001; ++ P < 0.01
In addition to absolute wound closure, wound contraction and re-epithelialization, two of the main mechanisms contributing to healing, 31,32 were analyzed on day 8 in the MCN group (Figure 5c). DB rats receiving MCN + vehicle had an open wound 82% larger than that of Normal animals treated with MCN + vehicle, and rates of wound contraction were reduced by 38%; re-epithelialization, however, was comparable between these two groups. DB rats subjected to MCN + NTX were similar in all parameters (i.e. wound size and contraction, re-epithelialization) to that of Normal animals given MCN + vehicle, with the size of the open wound and wound contraction of DB animals treated with MCN + NTX being one-half that of DB animals treated with MCN + vehicle.
To examine whether the effects of NTX on wound closure were dependent on a particular type of moisturizing cream (i.e. Neutrogena), some animals were treated with NTX in Oil of Olay (MCOO; Procter & Gamble, Cincinnati, OH, USA). In comparison to Normal animals exposed three times daily to MCOO + vehicle, those rats receiving 10−5 mol/L NTX in MCOO had 24–65% smaller residual wounds on days 5, 7 and 9 (Figure 6). DB animals subjected three times daily to MCOO + NTX had wounds that were 33–80% smaller than counterparts receiving MCOO + vehicle on days 5, 7 and 9.

Histograms of residual defects (%) in rat skin after formation of 6-mm wounds and followed for nine days. Groups included Normal and Diabetic rats treated three times (3×) daily with 10−5 mol/L naltrexone (NTX) dissolved in Oil of Olay moisturizing cream (MCOO + NTX 3×) or receiving vehicle alone (MCOO + Vehicle 3×), or 10−5 mol/L NTX dissolved in KY jelly (KYJ + NTX 3×) or KY jelly alone (KYJ + Vehicle 3×). Values represent means ± SEM. Significantly different from the respective vehicle at *P < 0.05, **P < 0.01 ***P < 0.001
To address the question whether the action of NTX was reliant only on moisturizing creams, Normal and DB rats were treated three times daily with NTX in KYJ (Figure 6). Wounds in Normal animals receiving KYJ + NTX were 10–17% smaller on days 3 and 5 relative to wounds treated with KYJ + vehicle. In contrast to DB rats receiving vehicle in KYJ, DB animals subjected three times daily to KYJ + NTX had wounds that were 15–65% smaller on days 3, 5, 7 and 9.
Histopathology
The overall pathology of the wounded region 20 d following surgery was evaluated with hematoxylin/eosin stains (Figure 7). The general structure of the epithelium between Normal and DB rats receiving vehicle or NTX appeared to be similar (e.g. absence of necrotic cells). However, in comparison to a width of the epithelium overlying the granulation tissue of 24.6 ± 1.6 μm in Normal rats, DB rats receiving vehicle had a 44% reduction. Normal animals treated with NTX, as well as DB rats subjected to NTX, did not differ in the thickness of the epithelium relative to Normal animals receiving vehicle.
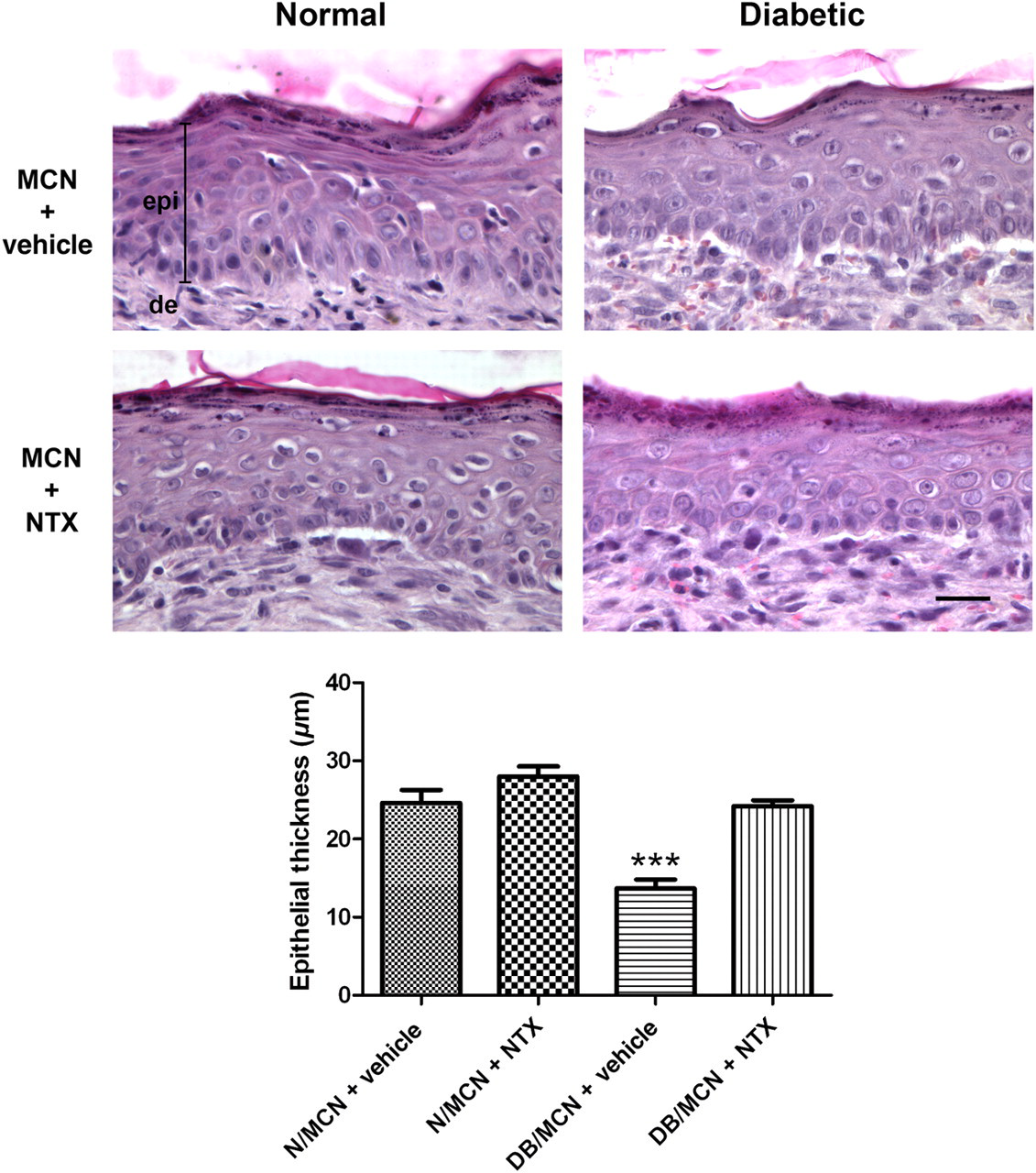
Photomicrographs of skin from Normal and Diabetic rats collected 20 d after the creation of 6-mm full-thickness wounds. Some wounds were treated three times daily with 10−5 mol/L naltrexone (NTX) dissolved in Neutrogena moisturizing cream (MCN + NTX) or receiving vehicle alone (MCN + Vehicle). Sections were stained with hematoxylin and eosin. epi, epidermis; de, dermis. Bar = 12 μm. Histograms of epithelial thickness (μm) measured 20 d after wounding. Values represent means ± SEM. Significantly different from N/MCN + Vehicle at ***P < 0.001. (A color version of this figure is available in the online journal)
DNA synthesis
In order to begin to decipher the mechanism of NTX action with respect to wound healing in DB rats, and keeping in mind previous reports that NTX targets cell proliferation, 6–12,19 normal and DB rats subjected three times daily to vehicle or 10−5 mol/L NTX in MCN were assessed for BrdU labeling on days 5 and 10 following wounding (Figure 8); skin adjacent and peripheral to the site of injury was evaluated. MCN + NTX altered DNA synthesis in the basal epithelium of skin adjacent to the wounds, but not in the peripheral region in both DB and Normal rats. In the DB rats, those treated with MCN + NTX had a 72% and 36% increase in labeling index on days 5 and 10, respectively, in the skin adjacent to the wound. In Normal animals there was an increase of 30% and 69% on days 5 and 10, respectively, in labeled cells located in the skin adjacent to the wound of Normal rats compared with cohorts receiving vehicle.
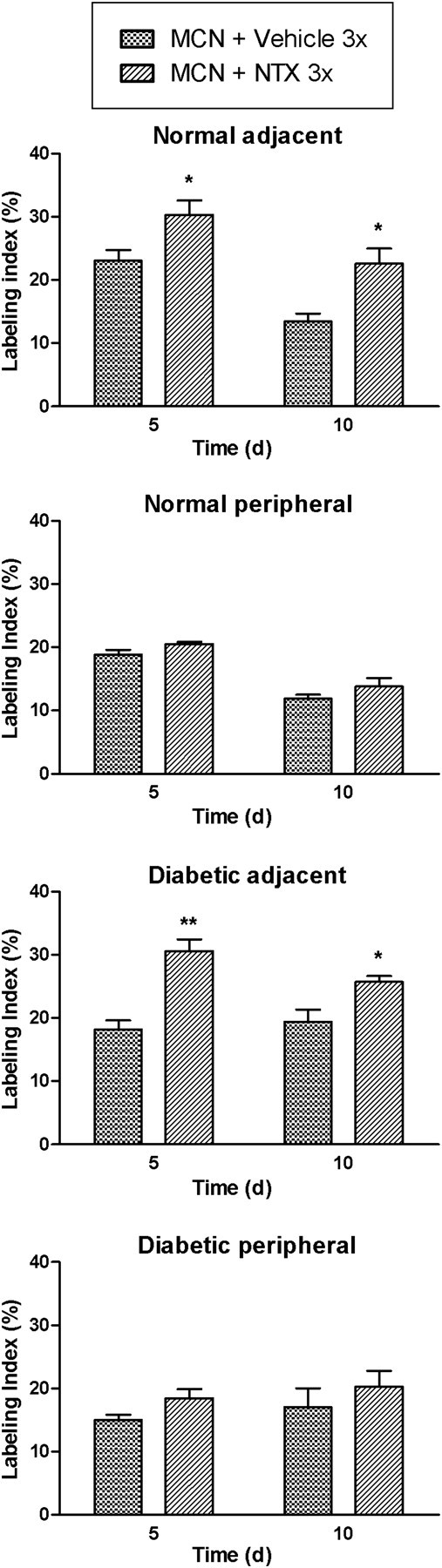
Histograms of the labeling indexes of basal epithelial cells in skin adjacent to and peripheral to wounds in Normal and Diabetic rats after topical treatment three times daily with 10−5 mol/L naltrexone (NTX) dissolved in Neutrogena moisturizing cream (MCN + NTX 3×) or receiving vehicle alone (MCN + Vehicle 3×); data were collected after 5 or 10 d of treatment. Values represent means ± SEM. Significantly different from their respective vehicle at *P < 0.05 and **P < 0.01
Discussion
With the use of a well-characterized model of T1D wherein rats developed typical physiological characteristics observed in diabetic humans such as hyperglycemia, weight loss and poor wound healing, 7,18,30 a major finding in this study is that disruption of endogenous opioid–opioid receptor interfacing with the opioid antagonist NTX can increase DNA synthesis in basal epithelial cells of the skin in T1D animals, as well as normal (non-diabetic) cohorts. The effects of NTX on cell proliferation were not toxic, relatively short-acting, and not dependent on either concentration (within a 100-fold range applied topically) or route of administration (systemic or topical). NTX administered by topical delivery was localized in influencing DNA synthesis, as cells subjacent to the carrier with drug were elevated in BrdU labeling but not basal epithelial cells distant from NTX application. Since NTX is a pure opioid antagonist and devoid of direct biological action, 33,34 the upregulation of DNA synthesis by interruption of opioid peptide–opioid receptor interfacing indicates that one or more endogenous opioid systems present in human and animal cutaneous epithelium 6 are intact and function as tonically active repressors of DNA synthesis under pathophysiological conditions related to T1D. Although some studies report that epithelium (e.g. ocular surface) of T1D animals has a subnormal level of DNA synthesis, 7 it is interesting to note that the basal layer of epithelial cells in the skin of diabetic animals had a rate of DNA synthesis comparable to that of normal rats, suggesting that at least two months after the induction of diabetes, abnormalities in cell replicative events were not evident in the skin. Whether differences in DNA synthesis of the basal epithelial cells between diabetic and normal animals occur at a subsequent time point after longstanding diabetes needs to be elucidated. Of course, if chronic diabetes does impact cell replication in the skin, modulation of the endogenous opioid system might serve to re-establish a homeostatic condition.
Based on these initial experiments, two carriers and one concentration of NTX were chosen to examine the effects of this agent on repair of full-thickness cutaneous wounds in T1D animals. Evaluation of closure rates showed that the wounds of diabetic animals were significantly slower to heal than those in normal rats, and that topical NTX placed in these carriers restored the rate of wound closure to levels comparable to and often exceeding that of normal animals. Rats with T1D had markedly reduced wound contraction compared with normal cohorts, but T1D animals receiving topical NTX were comparable to normal subjects. The structural appearance of the closed wounds in the diabetic rats receiving NTX was similar to that of normal animals, indicating that the increased rate of wound repair was not accompanied by abnormal morphological events. Although once daily application of NTX was sufficient to increase the rate of cutaneous wound closure in DB rats, three daily applications were superior. In future investigations, the optimal number of applications of NTX needed to restore wound healing to normal levels warrants consideration.
The successful use of NTX for topical delivery demonstrated herein raises the question of whether this drug has systemic repercussions. NTX is a small hydrophilic molecule that does not have the essential physicochemical properties necessary to achieve therapeutic doses for transdermal delivery, 35,36 but is known to enter human and animal cells rapidly by passive diffusion. 37 Our studies reveal that NTX had a localized but not systemic action, with DNA synthesis altered only at the site of delivery. Moreover, we employed a very small concentration of NTX that is non-toxic, but highly efficacious in terms of wound repair. Thus, in considering the application of topical NTX for the treatment of wounds clinically, our studies show that this is feasible in terms of biocompatability, and lack of toxicity and systemic action. Additionally, problems in compliance should be minimized by the localized effects of this opioid antagonist.
The present finding that an opioid antagonist can reverse the delayed rate of cutaneous wound healing recorded in diabetes to that of normal animals has some parallels with previous reports concerning corneal re-epithelialization in T1D rats. 7,18 These include: (i) efficacy of both topical and systemic NTX routes of delivery; (ii) response to similar concentrations (e.g. 10−5 mol/L) of NTX; (iii) NTX-induced increases in the rate of wound closure for both diabetic and normal animals; (iv) necessity for multiple daily applications of NTX to achieve optimal healing rates; and (v) DNA synthesis as a principle target for NTX action. However, some differences between the skin and cornea of diabetic and normal animals as to NTX's effects on wound healing should be noted and speak to the importance of the present studies. First, corneal wound healing is confined to the ocular surface epithelium and is reliant on re-epithelialization. In contrast, full-thickness cutaneous wound repair is related to both the epithelium and the stroma, and contraction plays a major role in repair. Second, studies on topical delivery of NTX to the cornea utilized only one aqueous carrier, but a variety of carriers (e.g. creams, gels) were utilized for repair of skin wounds. Third, the carrier for NTX in the cornea included an antibiotic, while no antibiotics were employed in the present study related to the skin. Thus, heightened opioid peptide–opioid receptor interaction as it relates to DNA synthesis and wound healing occurs in T1D, and blockade of this interfacing appears to be crucial in reversing the delayed repair of cutaneous, as well as corneal, wounds in a hyperglycemic environment.
Wound healing is a carefully orchestrated series of events with overlapping temporal and spatial relationships, and includes phases of inflammation, proliferation and remodeling. 1,38 In T1D, wounds often fail to progress through the normal stages of healing. 2,4 Some of the processes in wound repair that have been implicated as responsible factors include abnormalities in inflammation, migration, angiogenesis, neovascularization, cell proliferation, formation of granulation tissue and collagen, and re-epithelialization. 4,39,40 The present results demonstrate that opioid receptor blockade can restore the delayed wound healing recorded in diabetes to normal levels, indicating that endogenous opioid systems are fundamental to a major complication of T1D. Precisely how opioid peptides and opioid receptors are involved with the pathogenesis of diabetes is unknown. NTX is a general opioid receptor antagonist for classical (μ, δ and κ) 41 as well as non-classical (i.e. OGFr) 42 receptors. However, one clue provided in our investigation is the marked increase in DNA synthesis of the stratum basale in the skin of diabetic animals exposed to NTX. At least one endogenous opioid system, OGF-OGFr, is known to tonically regulate cell proliferation through an increase in the cyclin-dependent inhibitory kinase pathway. 43 The OGF–OGFr axis has been reported to depress T- and B-cell proliferation, 10,11 cell migration, 44 proliferation of keratinocytes and fibroblasts 6–12,19 and angiogenesis, 8,9 all of which have been implicated as factors in diabetic complications. Interestingly, patients with T1D as well as mice with T2D have elevated levels of OGF ([Met5]-enkephalin), 13–17 suggesting that diabetes is accompanied by an increase in an opioid peptide associated with an inhibition of cell replication. Hence, it may be postulated that excessive OGF–OGFr interaction retards wound closure such as is found in diabetes. Moreover, interruption of this activity by NTX is responsible, at least in part, for restoring related processes to a normal condition. Further studies are needed to elucidate the role of opioid peptides and opioid receptors in diabetes.
The glucose concentrations of the diabetic rats in this study were not only extraordinarily high compared with those of humans, but the duration of hyperglycemia was sustained for three months, emphasizing the magnitude of the diabetic condition. Thus, it is difficult to draw parallels with the human situation. However, the data suggest that even in the face of such uncontrolled diabetes, wound healing could be restored with topical NTX. This finding provides evidence that the action of NTX must be extremely potent, and that opioid–receptor interactions are capable of being disrupted by NTX in animals with persistently high glucose concentrations. Whether the combination of insulin-managed diabetes and topical NTX would be even more efficacious in healing full-thickness cutaneous wounds than either insulin or NTX alone remains to be addressed. At least in the repair of corneal abrasions, animals that were diabetic but receiving insulin to maintain euglycemia had an acceleration in corneal re-epithelialization with topical NTX treatment that even exceeded untreated animals. 45
Impaired wound healing is a major complication in both T1D and T2D. 1–4 The studies herein represent a paradigm shift regarding the etiology and pathogenesis of complications from diabetes by identifying opioid peptides and opioid receptors as key players in this disease. In keeping with our goal to translate our preclinical studies into the clinical setting, it is important to recognize that NTX is an US Food and Drug Administration-approved drug used at far higher dosages in the treatment of addiction (e.g. drug abuse, tobacco, gambling). 46,47 In addition, an ongoing phase I clinical trial is assessing the safety of topical NTX in the eye for the treatment of diabetic keratopathy, and the results heretofore indicate that NTX is without toxicity (Dr J Sassani, Penn State University College of Medicine, Hershey, PA, USA, personal communication). The utilization of small dosages of NTX in a topical application with localized but not systemic effects eliminates any potential adverse events, even for patients using opioids for pain management. Thus, topical NTX warrants clinical consideration as a treatment for delayed cutaneous wound repair.
Footnotes
ACKNOWLEDGEMENTS
This work was supported in part by a grant from the American Diabetes Association (7-09-BS-128).