
Abstract
Previous studies have indicated that prolyl hydroxylases (PHDs) function as tumor suppressors in human colorectal cancer (CRC), but their clinical and prognostic significance is uncertain. Expressions of PHD1, PHD2, PHD3 and hypoxia-inducible factor (HIF)-1α were detected using immunohistochemistry in an independent CRC cohort of 93 specimens represented on a tissue microarray (TMA). PHD expression levels were correlated with clinicopathological features, patient survival and presumed corresponding HIF-1α expression. Pearson χ 2 test was used to compare clinicopathological features with protein expressions. Survival was estimated by Kaplan–Meier analysis. Cox regression analysis was performed for multivariate analysis of prognostic factors. Of the TMA, 47, 68 and 51 from 93 specimens had low expressions of PHD1, PHD2 and PHD3, respectively. HIF-1α was positively expressed in 75 specimens. Low expression of PHD2 correlated with the high-grade group and a terrible overall survival (P = 0.017 and P = 0.032). Patients who had early stage CRC with low PHD2 expression had a poorer survival (P = 0.015), whereas patients with advanced-stage disease did not demonstrate such a difference (P = 0.691). Besides, PHD2 was uncorrelated with HIF-1α expression. The present study indicated that low expression of PHD2 in CRC predicts poor survival independent of HIF-1α, specifically for patients who have early stage tumors.
Introduction
The hypoxic milieu of tumor mass is a well-recognized microenvironmental factor that causes cancer progression and resistance to cancer therapy. 1,2 This involves multiple mechanisms of which the best-elucidated ones are mediated through a series of transcriptional gene activation by the hypoxia-inducible factors (HIFs). 3 HIFs in turn are regulated by an oxygen- and 2-oxoglutarate-dependent evolutionarily conserved enzyme family, namely the prolyl hydroxylases (PHDs). The hitherto known members of the family are PHD1, PHD2 and PHD3. 4
Several studies have revealed variable expression patterns of PHDs as well as their particular subcellular distribution in normal cells or tissues; nevertheless, in malignancies, PHDs are mostly indicated as tumor suppressors. 5 Absence of PHD1 expression was significantly associated with perineural invasion in pancreatic adenocarcinomas. 6 A germ line PHD2 mutation has been reported in human endometrial cancer, paraganglioma and recurrent extra-adrenal phaeochromocytoma. 7–9 Decreased expression of PHD3 blunts neuronal apoptosis, which may play a pivotal role in pheochromocytoma pathogenesis. 10 Additionally, PHDs are uncommonly found to correlate with each other. Elevated PHD1 concomitant with decreased PHD2 are causatively related to RNA polymerase hydroxylation and oncogenesis in human renal cell carcinoma. 11
For colorectal cancer (CRC), the expression status of PHDs is much more complicated. Aberrant expression of PHD1 inhibited tumor growth through increased necrosis and decreased microvessel density in CRC. 12 Recently, Xue et al. found that low PHD3 expression enhances cell viability and promotes colorectal tumorigenesis, while another group demonstrated that PHD2 suppresses tumor growth via reducing angiogenesis. 13,14 Although PHDs are implicated as putative antioncogenes, the expression patterns of PHDs in cancers, especially in CRC, are still intricate and whether or not expression of PHDs is associated with clinical and prognostic significance remains unknown. The purpose of this study was to assess the expression of PHDs in colorectal adenocarcinoma, evaluate the expression correlation between PHDs and HIF-1α, and investigate the association of PHD expression with clinicopathological characteristics and patient survival.
Materials and methods
Patients and tissue microarray construction
Patients with primary colorectal adenocarcinoma who underwent initial surgery at Southwest Hospital, Third Military Medical University, from 1999 to 2003, were retrospectively selected for this study. No patient had a history of hereditary CRC or had received chemotherapy/radiotherapy prior to resection. Postoperative treatments were applied according to the guidelines of National Comprehensive Cancer Network. All tissues were fixed in 10% buffered formalin and embedded in paraffin. Slides from these blocks stained with hematoxylin-eosin were reviewed by two pathologists (L Yi and SL Xu, Department of Pathology, Southwest Hospital, Third Military Medical University) to identify the histological grade. According to the World Health Organization guidelines, the CRC tissues were categorized as well differentiated, moderately differentiated, poorly differentiated or undifferentiated. The examined CRC cases were divided into two groups: the low-grade group consisted of well and moderately differentiated tumors, and the high-grade group consisted of poorly differentiated and undifferentiated tumors.
A tissue microarray (TMA) consisting of 93 primary colorectal adenocarcinomas, 15 colorectal adenomas and 12 normal colorectal tissues was constructed as described previously. 15 In short, a single 1.0 mm core was extracted from each donor tissue block and introduced into a recipient paraffin block using a Tissue Microarrayer (Beecher Instruments, Silver Spring, MD, USA). The recipient paraffin block was subsequently cut and slices transferred with adhesive tape to coated slides. The utilization of the tumor material for research purposes was approved by the ethical committee of Southwest Hospital.
Immunohistochemistry
Consecutive sections (5 μm) of paraffin-embedded TMA blocks were prepared and processed for immunohistochemistry (IHC) assay. After deparaffinization in xylene, the sections were rehydrated in graded alcohols, and microwaved with antigen retrieval solution for 20 min. Each section was incubated with 3% H2O2 for 10 min to block the endogenous peroxidase activity and treated with 3% goat serum at room temperature for 1 h to reduce non-specific immunostaining. The TMA sections were then incubated with the different antibodies at a dilution of 1:250 for PHD1 (Novus Biologicals Inc., Littleton, CO, USA), 1:200 for PHD2 (Novus Biologicals), 1:200 for PHD3 (Novus Biologicals) and 1:100 for HIF-1α (Santa Cruz Biotechnology, Santa Cruz, CA, USA). The primary antibody reaction was carried out at 4°C overnight, with sections incubated with phosphate-buffered saline instead of the primary antibodies for a negative control. This was followed by incubation with the secondary biotinylated goat polyvalent antibody (Santa Cruz Biotechnology) for 20 min and then incubated with peroxidase-labeled streptavidin for 20 min at room temperature. The staining was visualized by incubating with 3,3′-diaminobenzidine (Santa Cruz Biotechnology) for 5 min at room temperature, and then counterstained with hematoxylin. The TMA sections were then washed in water, dehydrated in an alcohol gradient, followed by xylene treatment, and mounted.
Evaluation of IHC
The immunostained TMA sections were analyzed by two pathologists (F Wu and J Yang, Department of Pathology, Southwest Hospital, Third Military Medical University) without knowledge of the clinicopathological outcomes of the patients. Re-evaluation was necessary for reaching a consensus when there was a disagreement between the two pathologists. For the four proteins, IHC staining was evaluated in a semi-quantitative protocol as described. 16 Briefly, a score was calculated by multiplying the intensity by percentage of stained cells, based on which a median value was obtained. Tumors with a score greater than the median value were considered at high protein expression.
Statistical analysis
All statistical analyses were performed using the SPSS statistics version 17.0 (SPSS Inc., Chicago, IL, USA). Associations of tested factors and clinicopathological characteristics were studied by Pearsons χ 2 test and Spearman rank correlation. The clinicopathological features include were demographic variables (age, gender and status of follow-up), pathological variables (tumor size, site, differentiation, lymph node invasion and pathological TNM stage) and clinical stage. The statistical significance of each test was set at <0.05.
The endpoint of the follow-up was June 2010. The follow-up information was retrieved from medical records, telephone visits and annulment of household registration. Survival analysis was used to model time from the date of surgery to the date of death from CRC. Individuals who died of causes other than CRC and those who were alive at the end of the study were considered to be censored. Survival analyses were performed using the Kaplan–Meier (KM) method for overall survival (OS). The log-rank tests and KM survival curves were used to compare low and high expression of proteins in each group of patients with low-stage disease (stages I and II) and high-stage disease (stages III and IV), or with lymph node invasion and without lymph node invasion, or with tumor size greater than 4 cm and tumor size equal or lesser than 4 cm. Cox regression analysis was performed for multivariate analysis of prognostic factors including tumor stage, tumor differentiation, tumor size and PHD2 expression. All statistical tests were two-tailed. The type I error rate of each test was controlled at <0.05.
Results
Characteristics of the study cohort
Relationships of PHDs and HIF-1α expression with colorectal lesions and clinicopathological features
NS, not significant; PHD, prolyl hydroxylase; HIF, hypoxia-inducible factor; pTNM, pathological tumor-node metastasis
*Fisher's exact test
†Pearson χ 2 test
P < 0.05 was considered significant
Decreased expression of PHD2 in CRC tissues
Immunohistochemical assay showed that the expressions of PHDs and HIF-1α were predominantly in cytoplasm or nucleus (Figure 1). PHD2 staining was significantly decreased in primary cancer tissues compared with that in non-cancerous tissues (colorectal adenoma and normal colorectal tissue), while there was no such significant difference among those tissues for the expressions of PHD1 and PHD3. As many as 85% (23 of 27) of the non-cancerous tissues were positively stained for PHD2. Consistent with our previous results,
17
HIF-1α was significantly over-expressed in CRC compared with non-cancerous colorectal tissues. Among 93 CRC cases, PHD1, PHD3 and HIF-1α were highly expressed in 49, 45 and 49% of the tumor tissues, respectively; only 25 cases (27%) were defined as high or strong expression of PHD2 (Table 1).
Representative high and low immunohistochemical staining of prolyl hydroxylase 1 (PHD1), PHD2, PHD3 and hypoxia-inducible factor (HIF)-1α in colorectal tumor tissue microarrays. Original magnification, ×100. (A color version of this figure is available in the online journal)
Correlation between expression of PHD2 and pathologic grading of CRC
Correlation coefficients among PHD2 and expression frequencies of the related proteins
PHD, prolyl hydroxylase; HIF, hypoxia-inducible factor; r, Spearman's rho
Low PHD2 expression is associated with shorter overall survival in CRC
The prognostic impact of clinicopathological variables on patient survival was evaluated by univariate and multivariate analyses. KM curves representing univariate survival analysis are shown in Figure 2. For all the patients, overall survival was significantly better for individuals that retained PHD2 expression as compared with those that did not (log-rank P = 0.032) (Figure 2a). Stage-specific survival analyses demonstrated that patients who had early-stage CRC (stages I and II) with low PHD2 expression had a significantly shorter OS than those who had CRC with high expression (log-rank P = 0.015) (Figure 2b), whereas the survival curve of patients with advanced-stage CRC (stages III and IV) indicated no statistically significant difference in OS between individuals with high and low PHD2 expression (log-rank P = 0.691) (Figure 2c). Furthermore, lower PHD2 expression in patients with lymph node invasion or tumor size greater than 4 cm was significantly associated with poorer OS (log-rank P = 0.046 or log-rank P = 0.024), compared with those with higher PHD2 expression (Figures 2d–g). In contrast, univariate survival analyses demonstrated no significant OS differences between these patients with high and low PHD2 expression based on other clinicopathological parameters. No significant difference was noted in OS between patients with PHD1/PHD3-higher tumours and patients with PHD1-lower tumors. The OS between stage-specific patients with PHD1-higher tumours and stage-specific patients with PHD1/PHD3-lower tumours was not significantly different either.
Evaluation of prolyl hydroxylase 2 (PHD2) expression as a prognostic indicator in colorectal carcinoma (CRC) by Kaplan–Meier survival curves. (a) Overall, CRC patients with low PHD2 expression had shorter CRC-specific survival than those with high PHD2 expression (log-rank P = 0.032). (b) In early-stage CRC (stages I and II), patients with high PHD2 expression had a significantly increased CRC-specific survival compared with those with low expression (log-rank P = 0.015). (c) The survival difference between high and low PHD2 expression among patients who had advanced-stage CRC (stages III and IV) was not statistically significant (log-rank P = 0.691). (d) and (e) Lower PHD2 expressions in patients with lymph node invasion (log-rank P = 0.046 versus log-rank P = 0.277) or (f) and (g) tumor size greater than 4 cm was significantly associated with poorer overall survival (log-rank P = 0.024 versus log-rank P = 0.488), compared with those with higher PHD2 expressions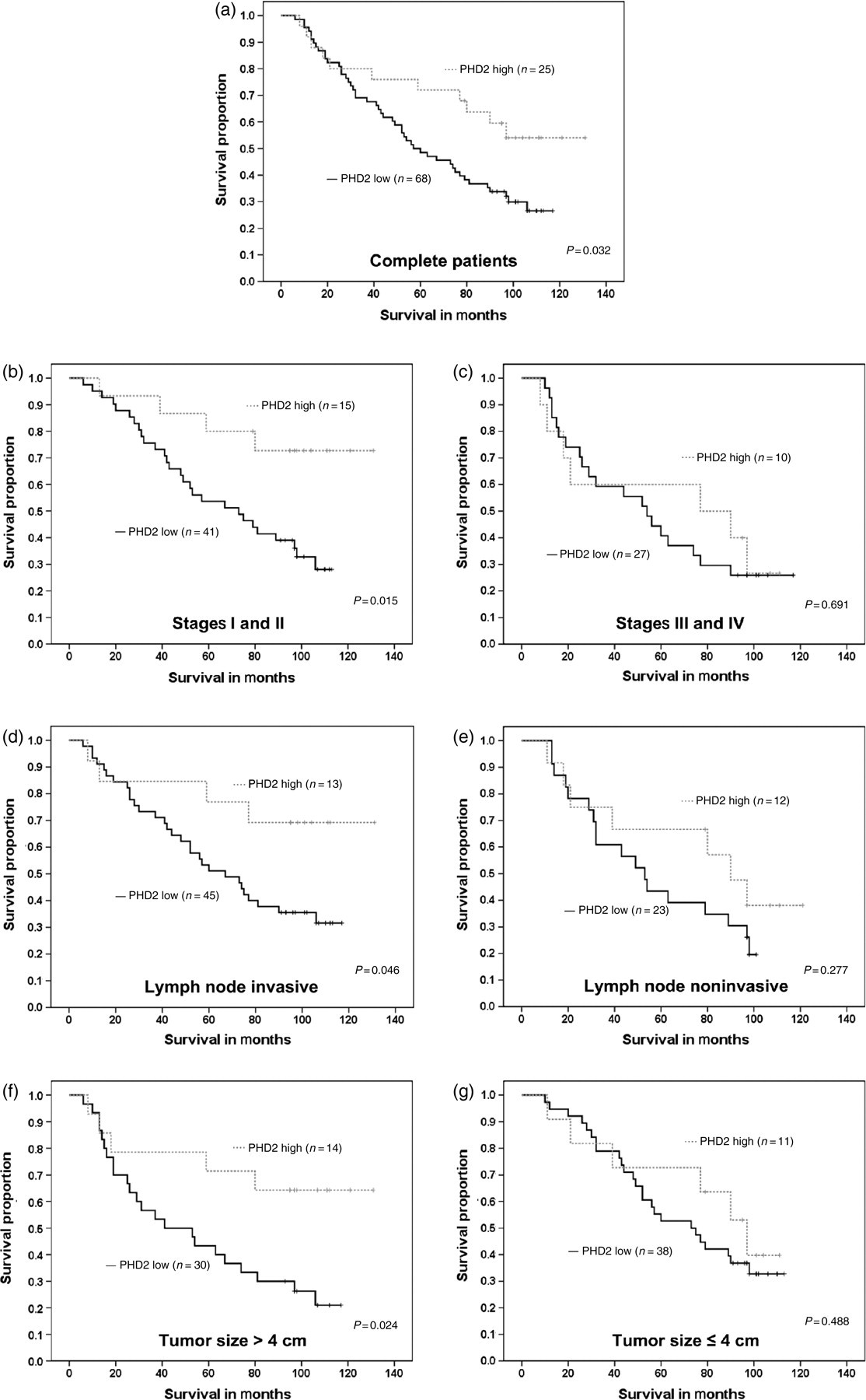
Cox regression analysis assessing the potential prognostic significance of the clinicopathological parameters and PHD2 expression
PHD, prolyl hydroxylase; HR, hazard ratio; CI, confidence interval
Discussion
PHDs are important regulators of cancerous angiogenesis and tumorigenesis. However, the clinical use of PHDs as prognostic markers in colon cancer has not been established. To our knowledge, this current study is the first to report the prognostic value of phenotypic expression of PHD2 in primary CRC. By using TMA immunostaining, we convincingly showed that PHD2 expression level is significantly down-regulated in cancer and that loss of PHD2 is an independent predictor of survival.
PHDs contain a hypoxia response element and its expression is induced under hypoxia. 18,19 Of the three PHDs, PHD2 appears to be the primary HIF-1 prolyl hydroxylase. In the normoxic state, PHD2 is the main cellular oxygen sensor. Berra et al. showed that under normoxic conditions, small interfering RNA inhibition of PHD2, but not PHD1 or PHD3, resulted in the stabilization of HIF-1α. 20 PHD2 levels are significantly reduced in certain malignancies such as colon and breast tumors and the reduction in PHD2 plays a critical role in up-regulating tumor angiogenesis. 14 In the present study, low PHD2 expression was found to be significantly associated with a poor overall survival according to univariate analysis, providing accumulating evidence for its putative role of a tumor suppressor.
The known function of PHD2 is to keep HIF-1α at a low level in normoxic conditions. Simplistically, one might expect PHD2 expression to correlate with HIF-1 inversely in normoxic tumor regions or vice versa. Nevertheless, the rank correlation coefficient of Spearman indicates that these two proteins are not significantly correlated in CRC; in other words, PHD2 and HIF-1α are considered to be independent from each other (P = 0.118, Table 2), although the expression of HIF-1α is a marker of poor prognosis in this cohort of population (log-rank P = 0.018, data not shown). Our results suggest that the elevated PHD2 is not necessary to down-regulate HIF-1α in CRC. Not surprisingly, PHD2 expression has indeed also been detected in large tumor regions simultaneously with HIF-1α. Jokilehto et al. found similar results in head and neck squamous cell carcinomas where HIF-1α and PHD2 expression could be simultaneously detected. 21 It was also reported that PHD2 was up-regulated under hypoxic milieu, suggesting changes in PHD2 levels were not responsible for HIF-1α stabilization under low oxygen tensions. Immunoblotting analysis of a set of 60 human cancer cell lines derived from nine distinct tissues including colorectum revealed that PHD levels do not necessarily inversely correlate with HIF levels as one would think. HIF levels are also sometimes elevated despite the presence of PHD2 in cases where there is a loss of von Hippel-Lindau (VHL). In some cases, a reduced level of PHD2 correlates with an increase in HIF-2α levels but not HIF-1α. 14 All together, these paradoxical results can be partly explained by the demonstration that HIF and PHDs form a feedback loop that limits hypoxic signaling, PHD2 being a direct HIF target gene. Moreover, it is also possible that PHD2 may have other targets in addition to HIF.
In our study, survival analyses based on tumor stage indicated that decreased expression of PHD2 was a prognostic factor for reduced survival of CRC patients (Figure 2a). Furthermore, stage-based survival analyses demonstrated that PHD2 elimination was associated with shortened survival for patients with early-stage CRC, but not for patients with advanced-stage CRC (Figures 2b and c). This may result from a stronger prognostic role of tumor stage compared with PHD2 expression. Additional larger studies are needed to assess the prognostic importance of PHD2 expression in patients with advance-stage CRC. In addition, we found that lower PHD2 expressions in patients with lymph node invasion or tumor size greater than 4 cm was significantly associated with poorer OS, compared with those with higher PHD2 expressions (Figures 2d–g), which indicates that IHC detection of PHD2 is helpful for predicting prognosis in those categorized patients.
In summary, this study indicated that low expression of PHD2 in CRC predicts poor survival independent of HIF-1α, specifically for patients who have early stage tumors. These findings remain to be validated in larger retrospective and prospective studies. More detailed elucidation of the function of PHD2 also requires performance in further studies.
Footnotes
ACKNOWLEDGEMENTS
We thank H Zeng for technical assistance. This work was supported by grants awarded to HJL from the Natural Scientific Foundation of China (Grant No. 30873015).