
Abstract
The purpose of this study was to analyze the incidence, etiology and clinical characteristics of community-acquired pneumonia (CAP) among outpatients with sore throat and/or cough, and thus to provide theoretical basis for timely and accurate diagnosis and treatment for CAP. We used chest X-rays for fever (a temperature greater than 37.58C) patients, who were recruited since 2007, presenting with sore throat and/or cough. The patients’ age, gender, days of fever, respiratory symptoms (e.g. cough and sputum), peripheral blood count and etiology (pathogens) of CAP were recorded. Of all the 6539 fever outpatients, those aged 10-39 and above 60 years old accounted for 61.0% and 15.6%, respectively. In total, 402 were diagnosed with CAP with an incidence rate of 6.1%. Among them, 38.1% were above 60 years old. The prevalence increased with age. Of the 402 CAP patients, 36.8% (148/402) presented no respiratory symptoms and 30.1% (121/402) had positive etiology. The top three pathogens were Mycoplasma pneumoniae (23.1%), Streptococcus pneumoniae (17.3%) and Haemophilus influenzae (9.1%). Among the 121 etiology-positive patients, 14 cases were mixed infections (at least one atypical pathogen). Nine cases were M. pneumoniae mixed with bacterial/virus infection, and five cases were Chlamydia pneumoniae mixed with other bacteria/ mycoplasma infection. We found that fever outpatients have a higher prevalence of CAP, which increases with age, i.e. older people are more susceptible to CAP. S. pneumoniae and H. influenzae are common pathogens in CAP; however, atypical pathogens, especially M. pneumoniae, remain the most common pathogens in CAP.
Introduction
Although community-acquired pneumonia (CAP) is a common disease and is also a serious threat to human health worldwide, very few large-scale epidemiological studies have been conducted in China. The incidence of adult CAP is affected by many factors, including regional geography, climatic conditions, age, gender and economic status. The regional incidence of CAP is quite different. For example, the overall incidence of CAP in Mediterranean coastal areas, Lu'beckof Germany and Shanghai was reported as 12/10,000,1–4 3.7–10.1/10005 and 0.35%, 6 respectively. The reported mortality rate is 1–5% for outpatient CAP, 12% for hospitalized patients with fever and 40% for intensive care unit patients. 1 A large prospective multicenter study showed that the mortality rate of CAP in Asia was 7.3%. 7 However, large-scale studies on CAP epidemiology, morbidity and mortality in China need to be conducted. Some studies have indicated that the starting time of the first dose of antibiotic therapy is correlated to CAP mortality, which should be carried out within 4-6 h. The mortality rate was increased if the treatments were delayed beyond six hours. 2 Thus, a timely and accurate diagnosis and use of antibiotics will help to reduce the mortality of CAP patients. Most CAP patients suffer from fever, so chest X-rays to demonstrate the prevalence and incidence of the CAP will help to improve the CAP diagnosis and to avoid the delay in treatment. In this study, we analyzed the disease incidence, etiology and clinical characteristics of CAP outpatients presenting with a sore throat and/or cough to provide a theoretical basis for timely and accurate diagnosis and treatment.
Materials and methods
Study design and patient selection
In this prospective study, we recruited 6539 newly diagnosed patients with fever (body temperature ≥37.5°C, age ≥10y) in our hospital from 1 January 2007 to 1 January 2008. All patients underwent a chest X-ray examination. Demographic information on age, gender and clinical information on days of fever, respiratory symptoms (e.g. cough and sputum) and laboratory blood test of each patient were recorded. The CAP cases were diagnosed according to the CAP clinical diagnosis standard formulated by the Chinese Society of Respiratory Diseases in 2006. 3 The diagnostic criteria included the presence of patchy infiltrates or interstitial changes shown by chest X-ray along with at least one of the following symptoms: (1) emerging cough, sputum or a deterioration in the original respiratory symptoms; (2) fever; (3) pulmonary consolidation and/or moist rales; (4) white blood cell (WBC) count >10 × 109 /L or <4 × 109 /L, with or without the nucleus left-shifting phenomenon. This study did not include patients with pregnancy, hospital-acquired pneumonia, obstructive pneumonia, active tuberculosis, acquired immunodeficiency syndrome (AIDS) and long-term use of hormones or other immunosuppressive agents. Patients with a medical history of human immunodeficiency virus (HIV) infection (diagnosis based on the confirmatory test result) were excluded because HIV would increase the number of patients with fever and pulmonary infiltrates in the 20-40 range and the pathogens isolated. After patients with CAP were recruited, they were screened for HIV antibody by enzyme-linked immunosorbent assay test.
Blood test
The peripheral blood counts were conducted using a Japanese Sysmex Kx-21 automatic multiproject equipment (Sysmex Corporation, Tokyo, Japan).
Pathogen detection
Sputum sample collection
With self-precautions, the nurses double-checked the requesting items, names and registration no. of the patients, and explained patiently and carefully the objective, importance and method of sputum sample collection. The first fresh sputum sample early in the morning was collected to increase the sensitivity because the quantity of the sputum, as well as the bacteria/fungi and exfoliated cells, are relatively high after accumulating overnight. The nurses instructed the patients to brush the teeth and rinse with clean water in order to reduce the opportunity of infection caused by normal flora or other subjects in the mouth. The patients were told to take a deep breath, cough deeply when aspirating to produce a sample of sputum. The nurses tapped on their chests to help loosen the deep sputum stick on the trachea. The patients were asked to inhale an aerosol mist to help to cough when they had trouble coughing up a sample.
Bacteriological testing
Timely collected specimens of respiratory secretions (sputum, throat swab or nasopharyngeal drawing objects) in patients were inoculated with blood agar, chocolate plate and MacConkey plate and cultured in 35°C for 16-24 h using the conventional methods of bacterial isolation and identification. The K2B method was used to determine the susceptibility of isolated and cultured bacterial activity in vitro. The dilution method was used to determine the minimum inhibitory concentration values and thus categorized as sensitive (S), moderately sensitive (I) and resistant (R).
Collecting paired serum samples of CAP patients at acute and convalescent (2-4 weeks) stage
Particle agglutination detection was applied to detect the Mycoplasma pneumoniae antibodies in paired serum (Fujirebio, Tokyo, Japan). Micro-immunofluorescence was applied to test the IgM antibodies to Chlamydia pneumoniae in paired serum (Focus, Cypress, CA, USA). Detection of double serum anti-Legionella pneumophila antibody IgG was performed by indirect immunofluorescence assay (Mardx, Carlsbad, CA, USA).
Positive etiology criteria
Positive etiology criteria included: (1) ≥1 strain of bacteria obtained from qualified sputum with moderate growth (semi-quantitative bacterial concentrations ≥7); (2) pathogens detected by blood culture; and (3) two samples collected at an interval of 2-4 weeks with antibody titer changes of ≥ 4 times. Of all the 402 cases, 602 sputum samples and 198 blood samples were cultured. Patients of the same strain were counted only once. To exclude the false-positive blood culture caused by other types of infections, we only included patients with normal results of stool/urine routine test, without sign/evidence of meningeal irritation/consciousness disturbances, or symptoms of co-morbid inflammatory disease.
Statistical analysis
All data were analyzed using statistical software SPSS 13.0 (Bizinsight Information Technology Co Ltd, Beijing, China). Differences in proportion ratios/clinical index among different age groups were analyzed by F-test, χ2 test, Cochran-Armitage trend test or Fisher's exact test. A P value of less than 0.05 was considered statistically significant.
Results
Significant differences in the incidence of blood cell increasing were observed between groups 20–29 and >60; as well as between groups 30–39 and 70–79 (Figure 1, Tables 1–5).
(a) Proportions of community-acquired pneumonia (CAP) in different age groups of fever patients. (b) CAP prevalence ratio in different age groups of fever patients
Status of fever outpatients and community-acquired pneumonia (CAP) patients
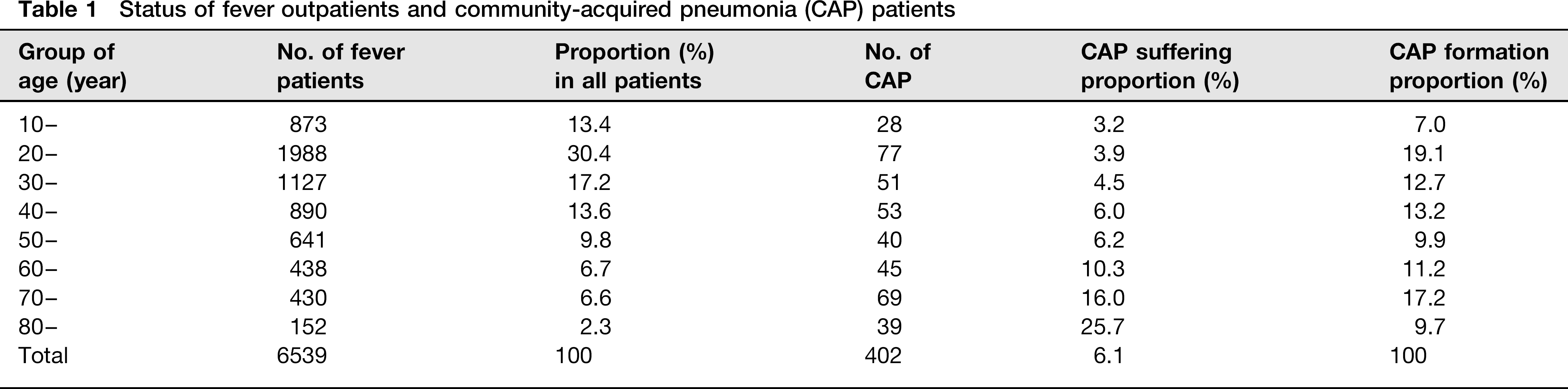
Correlation of prevalence ratio (PR) with age of onset of community-acquired pneumonia (CAP)

One-way sequence contingency test P < 0.001 indicating that CAP suffering proportion correlate to age. Cochran–Armitage trend test P < 0.001 indicating that CAP suffering proportion increased with age
Comparison of the general clinical condition of community-acquired pneumonia patients among different age groups

WBC, white blood cell
P value was from F-test;
P value was from χ2 test
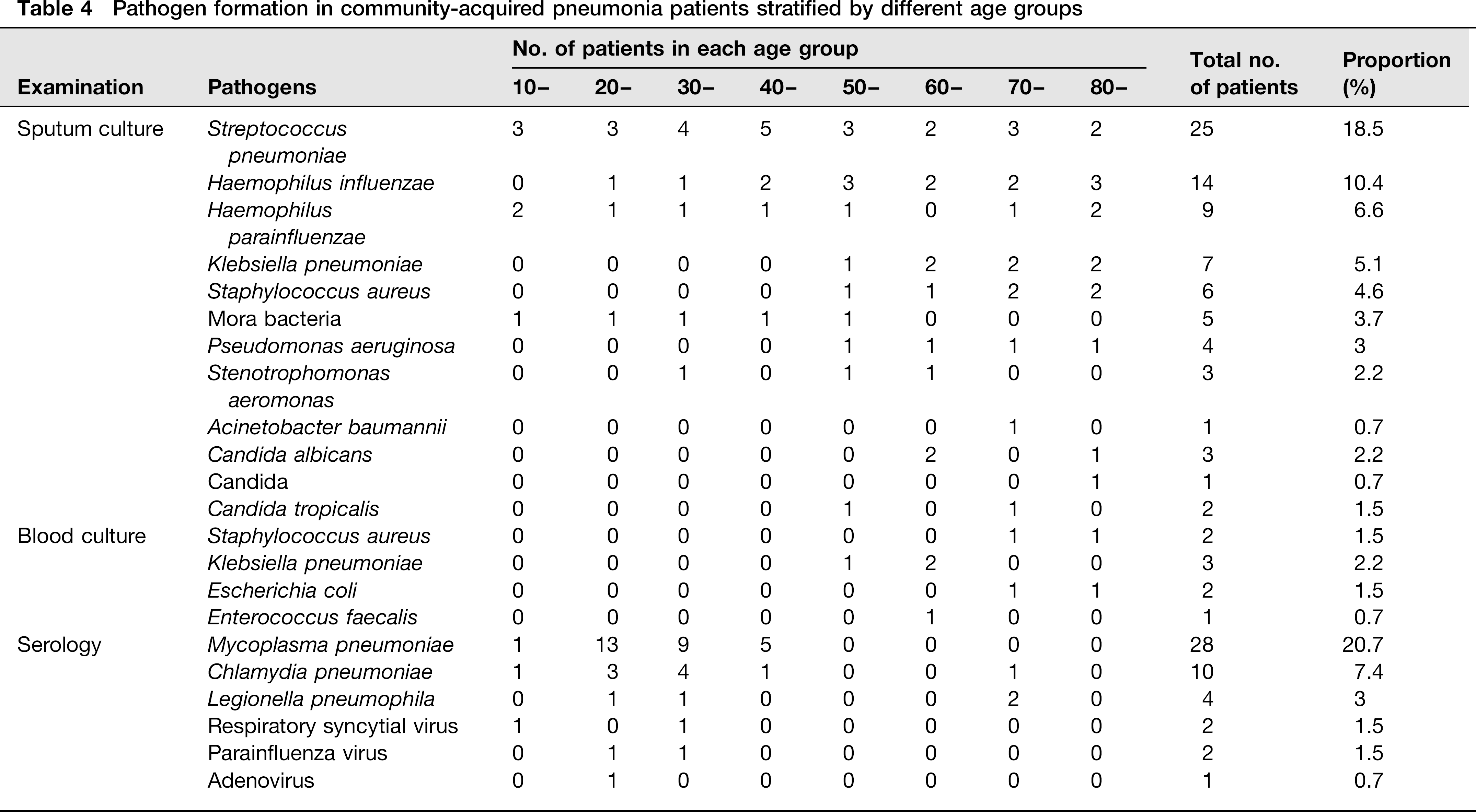
Pathogen formation in community-acquired pneumonia patients stratified by different age groups
Formation of the mixed infection of community-acquired pneumonia

General condition
Among the 6539 cases of newly diagnosed fever patients, 3314 men and 2823 women had non-CAP and the gender ratio (men:women) was 1.17. Of all CAP patients, 257 cases were men and 145 cases were women with a gender ratio of 1.77, indicating that the incidence of CAP was higher in men than that in women (Table 1).
Constitution of prevalence ratio in different age groups
The age group 20–29 ranked as the first one in all the fever patients, accounting for 30.4%. Those aged at 10–19 and 30–59 years old accounted for 61.0%, and those aged at >60 years old accounted for 15.6%. Interestingly, for the incidence composition of CAP, young patients (< 60) accounted for 15.6% (Cochran–Armitage trend test P < 0.001) indicating that the proportion of CAP prevalence increased with age (Table 2).
Clinical characteristics of CAP
The mean body temperature of CAP patients in each age group was above 37.5°C. The proportion of WBC count increased in the age groups of 20-29, 30-39 and 40-49 was 40.3%, 27.5% and 43.4%, respectively, with an average of 37.6%. But the proportion of WBC count in patients over 50 years old increased slightly, with an average of 58.5%. A significant difference was observed between the young and old patients. CAP patients without respiratory symptoms accounted for 36.8% of all CAP patients. There was no significant difference in WBC count between the CAP and non-CAP patients. The neutrophil count was not statistically significant either. However, a significant difference was observed in the items of respiratory symptoms between CAP and non-CAP patients (Tables 3 and 4).
Pathogen test of CAP
Of the 402 CAP patients, 121 (30.1%) cases were pathogen-positive, including 76 men and 45 women, with a gender ratio of 1.68%, and 11.6% (14/121) of them were mixed infections (≥1 atypical pathogens). One hundred and thirty-five results of different types of pathogens were obtained among the 121 patients with positive tests. Among them, 14 patients had mixed infections. Atypical pathogen infections were more frequent in young- and middle-aged patients, while Pseudomonas aeruginosa and Candida were more frequent in the elder patients (Table 4). The top three pathogens were M. pneumoniae (23.1%, 28/121), Streptococcus pneumoniae (17.3%, 21/121) and Haemophilus influenzae (9.9%, 11/121), respectively (Table 4). Among the 14 patients with mixed infection, nine cases were M. pneumoniae mixed with bacterial or viral infection; and five cases were C. pneumoniae mixed with other bacteria or mycoplasma infection (three cases were mycoplasma mixed with Chlamydia infection) (Table 5).
Discussion
We found that the incidence of CAP was 6.1% based on initial screening in those patients suffering from fever with sore throat and/or cough. In our study, 38.1% of all CAP cases were aged over 60, which may be attributed to reduced immunity and susceptibility to respiratory diseases. We found that the incidence of CAP in fever patients increased with age and the prevalence ratio increased from 3.2% to 25.7%. Consistent with the results from other studies, the men were more likely to suffer from CAP than the women.4,8 The proportion ratio of patients over 60 and 80 years old suffering from CAP was 10% and 25.7%, respectively. This suggests that doctors should pay attention to screening for CAP in old people with fever.
Almost half of the CAP patients (49.3%) had increased WBC count and even more in the >50 age group (58.5%). The 16 patients with atypical pathogen infections had normal blood tests; however, all of them had higher neutro-phil amounts. Among them, 12 patients had mixed infections. The WBC increasing is mostly caused by bacterial infection. The pathogens of CAP with normal/reduced leukocytes were mostly atypical pathogens or viruses, especially in the 20-40 age groups (62.4%). Unfortunately, this study failed to analyze the correlation of the pathogen distribution with increased WBC. Whether the patients with reduced/normal leukocytes carried atypical CAP pathogens/viruses needs further investigation. M. pneumoniae infection was common in patients < 50 years old (detection rate of 30.0%). Klebsiella pneumoniae infection rate (8.5%) in patients ≥ 50 years old was higher than that in < 50 years old. M. pneumoniae was the most common pathogen in patients 17-44 years old with the infection proportion of 43.2% followed by S. pneumoniae (40.7%). 10 The CAP bacterial infection in Beijing and Shanghai was 21.7% and 27.2%, respectively, and the pathogens were mainly S. pneumoniae, H. influenzae and K. pneumoniae. The infection rate of atypical pathogens (mainly M. pneumoniae) was 26.2 — 33.6%. However, the incidence rate of CAP atypical pathogens (M. pneumoniae, C. pneumoniae and L. pneumophila) was recently reported to be increasing between 3% and 40%.13–15 L. pneumophila infection accounted for mostly CAP pathogens without WBC increasing. 16 Therefore, to provide timely and effective treatment, antibiotic selection for CAP should be based on peripheral WBC count in combination with CAP pathogen distribution and antimicrobial susceptibility. The seasonal influenza presents the same way as other CAP pathogens and is associated with co-infections, which could impact the result of our study. Regretfully, we did not screen the seasonal influenza in the current study, which should be taken as a limitation.
Most CAP patients have respiratory symptoms and fever. About 30% of CAP patients had no respiratory symptoms.17,18 In this study, 36.8% of the patients had no respiratory symptoms and fever was the only symptom. Therefore, we provided chest X-ray as a screening tool in all fever patients to reduce the missing cases. The diagnosis rate of CAP with one, two, three and four days fever was about 50%, 70%, 86.1% and 92.3%, respectively. For patients with fever, without respiratory symptoms, and with at least one of the following characteristics: (1) fever lasted more than three days or fever without any reason; (2) .60 years old regardless of the peripheral blood leukocyte count, should do chest X-ray screening to detect the existence of CAP and to avoid the delayed or missing diagnosis.
CAP pathogen formation is very complicated and varies according to region, population and season. With the improvement of the examination methods, the detecting rate of the atypical pathogens such as M. pneumoniae, C. pneumoniae and Legionella was on the rise and they became the most common pathogens. The national multi-center survey of CAP etiology showed that the detection rate of atypical pathogen was 31.3% and M. pneumoniae was the most common pathogen.9,19 Our study demonstrated the important sequence of the atypical pathogens in CAP: the top three pathogens in order were M. pneumoniae, S. pneumoniae and H. influenzae. The treatment of CAP should take the atypical and mixed pathogens into account. S. pneumoniae or C. pneumoniae combined with M. pneumonia were the most common pathogens. The rates of Mycoplasma and Chlamydia co-infections are high in our study. As both of these pathogens were serological diagnoses instead of sputum culture, a false-positive result could not be excluded. However, similar high rates were reported by other research groups in China, and the underlying reason needs to be further investigated. The mixed infection rate in Britain was 28%, with a multiple infection rate of 47% in S. pneumonia. 20 An epidemiological survey in China indicated that 11.5% of the patients had mixed infections with more than two pathogens, and bacteria combined with atypical pathogens accounting for most of the patients. 9 In our study, 11.16% of CAP had mixed infections and eight cases were M. pneumonia combined with bacteria. The mixed infection rate may be lower than that in reality due to the limitations of the traditional bacteriological diagnostic methods.