
Abstract
Bi-ventricular (BiV) pacing is an effective therapy for the treatment of cardiac electromechanical (EM) dysfunction. The reason(s), however, for therapy non-response in approximately one-third of the subjects remains unclear, especially as it relates to myocardial perfusion and pacing location. In this study, we examined how acute BiV pacing response may be related to underlying myocardial perfusion coupled with pacing near or distant to the area of perfusion. In 10 open-chest anesthetized canines, coronary blood flow to the left ventricular (LV) anterior wall (AW: n = 5) and lateral wall (LW: n = 5) was controlled during four pacing conditions: right atrial, right ventricular (pseudo-left bundle branch block; [pseudo-LBBB]), BiV-LW and BiV-AW. Local EM function (piezo-electrical crystals and electrodes), along with global hemodynamic parameters, were measured during all pacing conditions at three coronary perfusion rates (≥0.40 mL/min/g, 0.20–0.40 mL/min/g and <0.20 mL/min/g). A positive BiV therapy response was assessed by a significant increase in the maximum cardiac output compared with the pseudo-LBBB condition. Despite no improvement in QRS duration, BiV-LW pacing improved LV function compared with the pseudo-LBBB pacing condition (P value <0.01). This improvement with BiV-LW pacing was seen above a certain myocardial perfusion threshold and was independent of any increases in regional coronary blood flow with BiV pacing. At lower myocardial perfusion rates, LV function was not improved with BiV pacing at any location. This study underscores the significance of even mild ischemia on BiV pacing response.
Introduction
Over the last 15 years, bi-ventricular (BiV) pacing has been an effective treatment option for patients with moderate to severe heart failure (HF) with electromechanical (EM) dysfunction and asymptomatic ischemic HF patients with left bundle branch block (LBBB). 1–3 Despite the utility of the therapy, 30% of patients show no improvement in functional and/or clinical status after treatment (non-response). 4 Due to the EM nature of the therapy, research has focused largely on echocardiographic or electrocardiographic measures of left ventricular (LV) function. However, no EM parameter or etiological classification of the HF condition has been useful in prospectively predicting therapy response. 5,6
While it has been widely accepted that pacing in scarred regions does not promote a positive response to therapy, 7–11 little research has been done regarding the role of myocardial perfusion as it relates to therapy response. Most studies suggest that pacing at or near sites of previous myocardial infarction does not promote therapy response, 7–11 but a recent study suggests that pacing at ischemic or scarred sites can still produce a positive response to therapy. 12 In addition, numerous reports suggest that certain pacing regions, like the lateral LV wall, are more beneficial for response, 10,13–19 while others suggest that all LV regions can be ‘optimal’ sites for the third lead placement. 20–24
Despite the fact that terms such as ‘ischemic’ and ‘non-ischemic’ are used to describe the heart condition prior to device implantation, the true myocardial perfusion rate is unknown. Even though BiV therapy is effective in patients with and without ‘ischemic’ heart disease, 6 simple classifications of ‘ischemic’ or ‘non-ischemic’ heart disease are not adequate to describe the true state of myocardial perfusion in each patient. For example, patients with certain ‘non-ischemic’ cardiomyopathies have diminished micro-circulatory perfusion, despite having a classification of ‘non-ischemic’ heart disease. 25
There has been no systematic study on the role of myocardial perfusion coupled with lead location on BiV therapy response. Therefore, the focus of this study was to determine whether LV mechanical response is dictated by myocardial perfusion rate and LV pacing location in non-infarcted hearts with EM dysfunction. We tested the hypothesis that the lateral LV wall is the optimal BiV pacing site only with sufficient ventricular perfusion.
Materials and methods
A total of 10 male mongrel dogs were used in the study (body weight = 22 ± 2 kg; heart weight = 186 ± 22 g). Each animal was given a subcutaneous injection of morphine (3 mg/kg) as a preanesthetic and bolus injections of α-chlorolose (100 mg/kg intravenous) to maintain a surgical plane of anesthesia. Additional doses of morphine and α-chlorolose were given as needed (as monitored by heart rate and reflex reactions). Each animal was intubated and mechanically ventilated with supplemental oxygen. Constant venous drips of pure 0.9% NaCl solution and 0.9% NaCl solution with 2 mg/mL of lidocaine (one dog) and 0.008 mg/mL of levophed (two dogs) were used to maintain a stable experimental preparation.
After the establishment of a stable anesthetic plane, the chest was opened using a left lateral thoracotomy and the heart was placed in a pericardial cradle and instrumented (Figures 1a and b). The most proximal portion of the left anterior descending (LAD; n = 5) or left circumflex (LCX; n = 5) artery was cannulated, connected to a servo feedback pump (EMKA, Inc., Middletown, PA, USA and Idex Corp., Northbrook, IL, USA) and perfused with an arterial blood supply from a femoral cannula. Coronary flow through the cannulated artery was measured with an in-line flow probe, cardiac output (CO) was measured with a perivascular probe around the ascending aorta (Transonic Systems, Inc., Ithaca, NY, USA), aortic pressure was measured using a standard fluid filled transducer and LV pressure was measured using a Millar® Mikro-Tip SPR-524 catheter (Millar Instruments, Inc., Houston, TX, USA). Ultrasonic crystals (Sonometrics, Inc., London, ON, Canada) with barb electrodes were placed in the epicardial/mid-wall of the mid/apical LV anterior territory (LAD territory) and the basal LV anterolateral territory (LCX territory) to measure local EM function. Pacemaker leads (CapSureFix Novus Model 5076; Medtronic, Inc., Minneapolis, MN, USA) were placed epicardially in the right atrial (RA) appendage, the right ventricular (RV) apical freewall near the septum, the mid LV lateral freewall (LW) and the LV anterior apical wall (AW). The electrocardiogram limb leads, augmented leads and one precordial lead were recorded. A coronary venous catheter was placed in a local vein for blood sampling. Data were acquired, low-pass filtered and stored at a rate of 2000 Hz (ADInstruments, Colorado Springs, CO, USA; Biopac, Inc., Goleta, CA, USA; and Grass Technologies, Astro-Med, Inc., West Warwick, RI, USA).
Diagram of experimental setup: (a) frontal view and (b) ventricular cross-sectional view. (c) The timeline of pacing and coronary perfusion pressure conditions for each animal. Note that in between each pacing condition, there was a five-minute or longer period at baseline (80 mmHg RA pacing) before proceeding to the next condition. AoP, aortic pressure; AW, anterior wall; BiV, bi-ventricular; CO, cardiac output; LV(P), left ventricular (pressure); LW, lateral wall; RA, right atrial; RV, right ventricular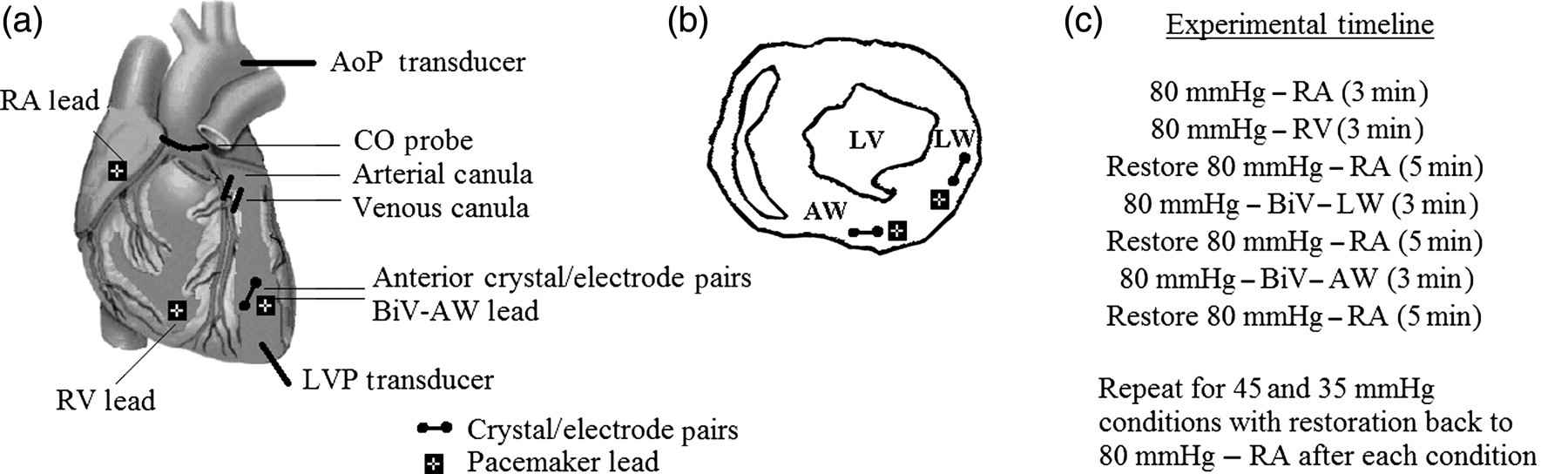
The study was approved by the Animal Care Use Committee on the campus of Indiana University-Purdue University Indianapolis and was done in accordance with the Animal Welfare Act, Institute of Laboratory Animal Research guidelines and the Public Health Service policy.
Cardiac recordings
In each animal, testing occurred at four pacing conditions: (1) RA; (2) RV (i.e. pseudo-LBBB); 15 (3) BiV-LW; and (4) BiV-AW and at three coronary perfusion pressures: (1) 80 mmHg; (2) 45 mmHg; and (3) 35 mmHg. The coronary perfusion pressures were chosen to examine the effects of perfusion within and outside the coronary artery auto-regulation range for each pacing condition. 26 These three coronary perfusion pressures translated into perfusion rates of ≥0.40, 0.15–0.40 and <0.15 mL/min/g for the LAD experiments and ≥0.40, 0.25–0.40 and <0.25 mL/min/g for the LCX experiments. For analysis, the data were further grouped into just two groups: ≥0.15 and <0.15 mL/min/g for the LAD experiments (29% of baseline) and ≥0.25 and <0.25 mL/min/g for the LCX experiments (66% of baseline). The divisions were near the lower limit of the coronary auto-regulation range for each experimental group as observed by the local crystal recordings. The cut-off level was higher for the LCX than the LAD region due to the higher degree of perfusion in the LCX for the same coronary perfusion pressure (i.e. LCX has a lower resistance than the LAD in canines).
At each perfusion rate, RA pacing established the intrinsic baseline condition, RV pacing provided the pseudo-LBBB condition, and BiV-LW and BiV-AW pacing produced two different therapy conditions. The pacing parameters were similar for all animals in their respective perfusion groups. Specifically, the atrioventricular (AV) delay was ∼30 ms for most animals to create an appropriate pseudo-LBBB condition during RV pacing. The mean interventricular delay was similar between BiV pacing conditions and was optimized for each animal to achieve the largest CO response at each perfusion condition.
The four pacing conditions were examined first at the coronary perfusion pressure of 80 mmHg and then at the lower perfusion pressures for three minutes (Figure 1c). After a given pacing condition below 80 mmHg, the perfusion pressure was restored back to baseline to allow recovery of the myocardium before proceeding to the next pacing/perfusion condition. To ensure the myocardium was viable, the crystal segment length waveform (to ensure local systolic shortening) and/or the reactive hyperemia response (to ensure oxygen debt repayment) was monitored following the restoration of the coronary perfusion pressure back to baseline at 80 mmHg. Once the coronary flow recovered to its baseline condition, the next experimental condition was tested. At each perfusion pressure and pacing condition, hemodynamics along with local and global EM function were recorded. Coronary arterial and venous blood samples were taken in the region of interest during each condition for blood gas analysis (Gem Premier 3000; Instrument Laboratory, Bedford, MA, USA). At the end of the study, the animal was euthanized and the heart was excised and weighed.
Data analysis
The analysis of the cardiac recordings took place offline using custom-made software developed in Matlab® (Mathworks®, Natick, MA, USA) and in LabChart 7 (ADInstruments). For each animal and condition, data were sampled from multiple (at least 10) cardiac cycles in the middle of the file. Myocardial oxygen consumption (MVO2) was derived by multiplying the LAD or LCX flow rate times the difference between the arterial and venous O2 content divided by the heart weight times 29% or 39%, respectively. 26 The global EM delay (EMDglobal) for a given cardiac cycle was determined by taking the difference in time between the onset of the QRS complex and the occurrence of the LV dP/dt max. The local mechanical delay (MED) was defined as the time difference between the onset of local shortening and the occurrence of the LV dP/dt max. Global LV therapy response was assessed using the maximum cardiac output (COmax), a measure of LV contractility. 27 A therapy responder was identified if the global response (COmax) was statistically greater for a given BiV pacing condition compared with the pseudo-LBBB pacing condition (Mann-Whitney test; P value <0.01).
Statistical analysis
At a given pacing regimen, comparisons were made for all physiological parameters relative to each pacing condition and the largest myocardial perfusion rate. A non-parametric Mann-Whitney test (P value <0.01) was used due to the non-normality of the data.
Results
Hemodynamic variables for all animals (mean ± standard deviation)
HR, heart rate; LAD, left anterior descending (artery); LCX, left circumflex (artery); MAP, mean arterial pressure; MVO2, myocardial oxygen consumption
Mann-Whitney test: *P value <0.01 versus respective RA, † P value <0.01 versus respective RV, ‡ P value <0.01 versus respective BiV-LW and § P value <0.01 versus respective higher perfusion rate
Electromechanical variables for all animals (mean ± standard deviation)
CO, cardiac output; EMD, electromechanical delay; LAD, left anterior descending (artery); LCX, left circumflex (artery); QRSd, QRS duration
Mann-Whitney test: *P value <0.01 versus respective RA, † P value <0.01 versus respective RV, ‡ P value <0.01 versus respective BiV-LW and § P value <0.01 versus respective higher perfusion rate
Crystal and electrogram data (Figures 2a and b) showed that BiV-LW pacing re-established local and global EM function better than the pseudo-LBBB and BiV-AW pacing conditions when LAD and LCX myocardial perfusion was ≥0.15 and ≥0.25 mL/min/g, respectively. Local and global improvements were identified by smaller MEDs and larger COmax values for the BiV-LW pacing condition versus the pseudo-LBBB and BiV-AW pacing conditions, respectively. However, when LAD/LCX perfusion was reduced, BiV pacing at the lateral and AW did not improve local or global EM function (Figures 2c and d). In several cases, MEDs were undefined (UD) for all pacing conditions due to the lack of a sustained systolic shorting period. At this lower perfusion rate, BiV pacing at either wall region did not improve local MEDs or global COmax as compared with the pseudo-LBBB condition.
Local electrogram, local myocardial displacement, body surface electrocardiogram lead II, left ventricular pressure (LVP) and aortic cardiac output (CO) tracings in canines with (a) LAD perfusion >0.15 mL/min/g, (b) LCX perfusion >0.25 mL/min/g, (c) LAD perfusion <0.15 mL/min/g and (d) LCX perfusion <0.25 mL/min/g. The mechanical delay (MED) is the time delay between the start of the rise in the LV pressure (vertical line) and the start of local shortening (asterisk). Note that (c and d) have undefined (UD) MEDs since there was no sustained systolic shortening period (no asterisk). Scale shown for the right atrial (RA) tracings. AW, anterior wall; BiV, bi-ventricular; ECG, electrocardiogram; LAD, left anterior descending (artery); LBBB, left bundle branch block; LCX, left circumflex (artery); LW, lateral wall
Due to the higher perfusion rate in the LCX versus the LAD for the same coronary perfusion pressure, a perfusion rate of 0.15 mL/min/g for the LAD and 0.25 mL/min/g for the LCX was used to separate BiV responders and non-responders (Figure 3). The response was seen in 67% of the cases during BiV-LW pacing and 13% of the cases during BiV-AW pacing when the LAD myocardial perfusion was ≥0.15 mL/min/g. When myocardial perfusion was <0.15 mL/min/g in the LAD, no response to therapy was seen with BiV-AW or BiV-LW pacing. Myocardial perfusion ≥0.25 mL/min/g in the LCX resulted in a positive response rate of 83% with BiV-LW pacing and 67% with BiV-AW pacing. For a myocardial perfusion rate <0.25 mL/min/g in the LCX region, response to therapy was seen in 34% and 17% of the cases with BiV-LW and BiV-AW pacing, respectively.
Percentage of responders versus myocardial perfusion rate with respect to pacing location for the (a) LAD and (b) LCX cannulation experiments. A responder was one that had a larger maximum cardiac output for the BiV versus the pseudo-LBBB condition (P value <0.01). AW, anterior wall; BiV, bi-ventricular; LAD, left anterior descending (artery); LCX, left circumflex (artery); LW, lateral wall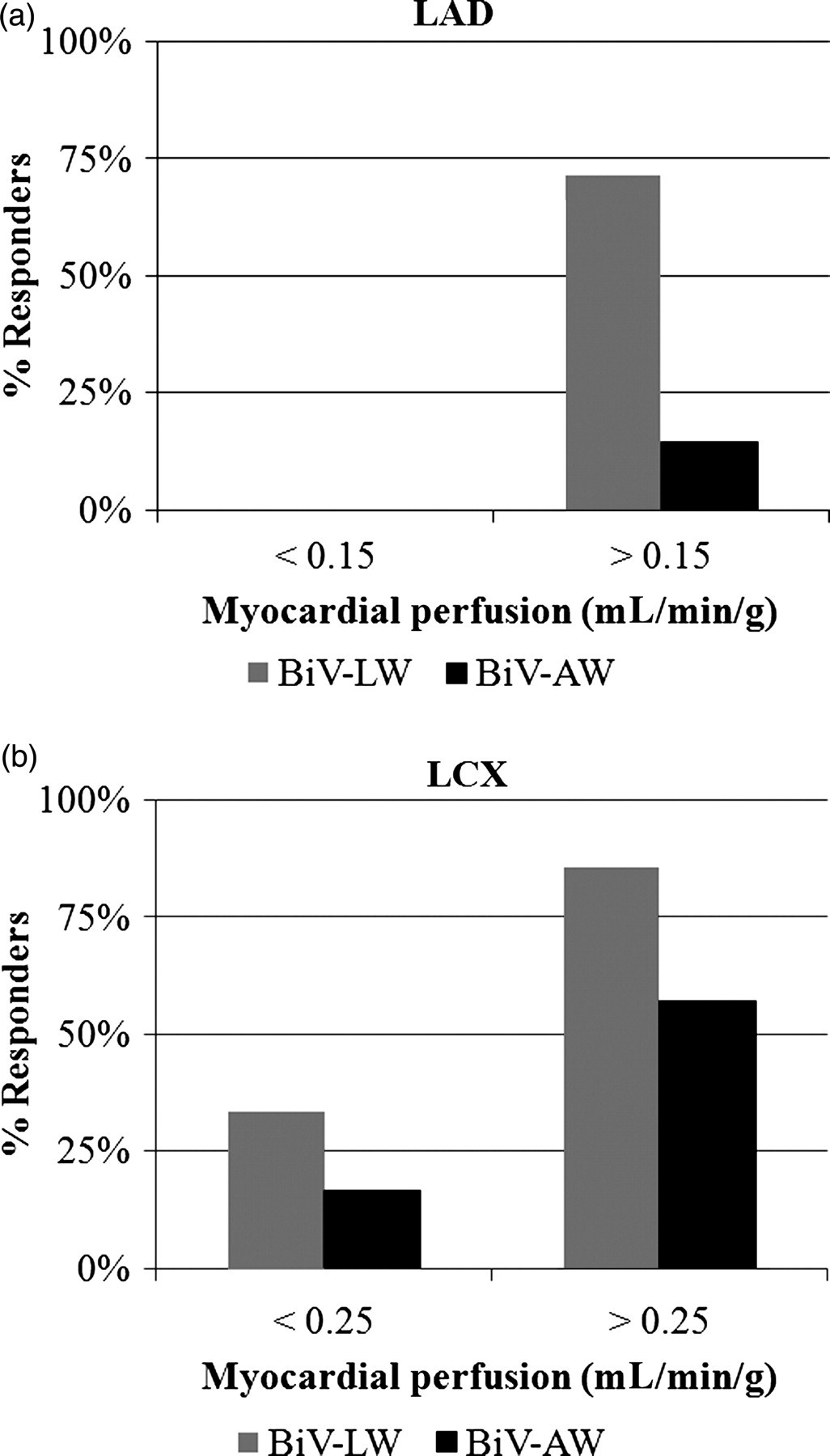
Discussion
This study shows that response to BiV therapy is dependent both on myocardial perfusion rate and LV lead location in hearts with EM dysfunction and some degree of ischemia, but no necrosis. When myocardial perfusion was greater than 0.15–0.25 mL/min/g, lateral wall pacing gave a significantly higher response to therapy compared with AW pacing in experiments with flow regulation in both the anterior and lateral wall (Figures 2 and 3). This report of superior outcomes with lateral versus anterior LV wall pacing is consistent with numerous reports in patient studies. 10,13–19
While the lateral wall is often thought to be the best pacing location, no systematic study has shown whether lateral wall pacing is still beneficial if the myocardium in that region becomes ischemic. Therefore, the AW pacing condition was used primarily to examine whether or not pacing remotely in the AW during times of lateral wall ischemia may promote a better BiV response. The results showed that even during lateral wall ischemia, BiV-LW pacing had a higher response compared with BiV-AW pacing, which highlights the importance of the lateral wall location for BiV therapy. The AW responder rates were higher during the LCX versus the LAD flow regulation experiments. This is not unexpected since the LAD perfuses the AW and is consistent with reports that show AW pacing can be a beneficial site for BiV therapy. 20–24 An additional pacing location on the posterior wall was tested in several animals, but was not shown to consistently improve LV function compared with lateral wall pacing.
When myocardial perfusion fell below 0.15 mL/min/g (LAD) or 0.25 mL/min/g (LCX), there was a greatly reduced response to BiV therapy at either location (Figures 2 and 3). By examining the EM function at a local myocardial perfusion rate, it is clear why myocardial perfusion is a critical factor in BiV therapy response (Figures 2a and d). When myocardial perfusion exceeded 0.15 mL/min/g in the LAD region (Figure 2a) and 0.25 mL/min/g LCX region (Figure 2b), BiV-LW pacing improved both local shortening timing response in the regions of interest (see MEDs) and improved global COmax. Thus, the coronary perfusion rate was able to adequately supply the myocardium and pacing helped to improve local and global EM function. However, when the myocardial perfusion was <0.15 mL/min/g (LAD) and <0.25 mL/min/g (LCX), BiV pacing at neither the lateral nor the AW was able to restore normal local or global LV function. This was evidenced by the lack of systolic shortening (MEDs were UD in Figures 2c and d) and the unchanged or diminished COmax. To our knowledge, this is the first time that lack of BiV response has been shown directly related to diminished, but not complete, obstruction of coronary flow.
Although there is no question that human cardiac resynchronization therapy (CRT) recipients have some degree of ‘ischemic stability’ that allows them to sustain life and in some cases even improve with therapy, perfusion is often compromised in these patients. A recent study was the first to show both myocardial perfusion and metabolism data in CRT patients. 12 In CRT patients, perfusion below 50% of the maximum baseline with a concurrent reduction in metabolism was seen in 30–48% of the myocardial mass. 12 In this study, we showed similar results with a 34–75% reduction in baseline perfusion in the LV regions that made up 29–39% of the total myocardial mass (i.e. LAD region versus LCX region, respectively).
Several studies related to atrial fibrillation (AF) and CRT have shown that increased pacing rate with CRT (i.e. increased demand) can diminish effectiveness of the therapy. Two of these AF/CRT studies showed that for higher basal heart rates, the LV function was diminished with CRT during an increase in pacing rate. 28,29 However, two additional reports have shown some improvements in exercise endurance outcomes (e.g. exercise duration) during rate-responsive pacing. 30,31 In particular, one report showed improved metabolic outcomes during exercise only evidenced in patients with lower baseline heart rates and lower heart rate reserves. Coronary flow reserve (CFR) was shown to be significantly increased in CRT responders, but not in CRT non-responders. 32 In this study, however, it could not be determined whether the higher CFR in responders was a result of CRT or whether the positive CRT response was due to an increase in coronary perfusion. Therefore, all of these studies seem to suggest that some, but not all, CRT recipients are able to show increased myocardial supply during increased myocardial demands. This is not unreasonable since some patients are responders and others are non-responders to CRT. These reports underscore the need for further investigations on myocardial supply/demand matching related to CRT response in humans.
It may be hypothesized that BiV pacing helps to increase coronary flow, which in turn improves LV pump performance. Myocardial perfusion pressure (not flow) was regulated in this study, thus this hypothesis could not be fully tested, since coronary perfusion (flow) was allowed to adjust according to physiological and pacing conditions. However, at both the high and low coronary pressures, myocardial perfusion (flow) was not increased related to BiV pacing at either location. Thus, for this model, BiV pacing did not seem to increase coronary flow to elicit a positive LV response. This is an important finding, but will require additional validation in diseased hearts.
In this study, there was no statistical difference in overall myocardial blood flow (perfusion) between the baseline, pseudo-LBBB and BiV pacing groups (Table 1), which is consistent with results in human patients with BiV therapy turned ‘on’ or ‘off’. 33 Although not measured in this study, it may be that while overall coronary flow was not increased, the distribution of the flow to specific locations in the myocardium (e.g. endocardial/epicardial distribution) was affected. It has been shown that septal-to-lateral blood flow distribution can become more homogeneous with BiV pacing in patients, 33 but this kind of redistribution seems unlikely in this study since coronary flow was regulated either in the septum (100% supplied by the LAD in canines) or the lateral wall (mainly supplied by the LCX dominant artery), 34 but not both.
Numerous studies have shown that BiV therapy can help to restore LV dyssynchrony in some patients, 4,13,35 but no study has shown why non-response occurs in others. For the first time, this study shows that a lack of restoration of LV dyssynchrony can be at least partially related to a lack of adequately perfused myocardium. The myocardium, at the lower perfusion rates, was not necrotic since restoration of the coronary perfusion pressure back to the baseline rate after each lower myocardial perfusion rate resulted in a reactive hyperemia response (debt repayment) and restoration of the local systolic shortening. Thus, these results suggest that ischemia, without full occlusion of coronary blood flow, may result in a BiV non-response, even with ‘proper’ LV lead location. Although untested at this time, it is logical to assume that there is a myocardial perfusion threshold in man, below which an effective response to BiV pacing cannot occur.
Since positive therapy response was not 100% even at normal coronary perfusion conditions, other factors may be involved in BiV therapy response. This is not unexpected since BiV therapy response is complex and related to multiple factors. 5 Since local LV mechanical work is directly related to local myocardial blood flow, 36,37 the myocardial perfusion rate was the major focus of this study. Additional work is required to understand the complex interactions between myocardial perfusion, lead location and other factors in BiV therapy response in failing human hearts.
This study supports previous findings that traditional EM measures are not able to predict BiV pacing response. 38 Although not done with a chronic HF model, this acute animal model with a wide QRSd and pseudo-LBBB, showed that the widely used QRSd measure was not able to predict response to BiV therapy. When separated, BiV-LW and BiV-AW responders did not have a narrower QRSd compared with non-responders (Mann Whitney; P value < 0.01). The fact that QRSd did not narrow with response to therapy was not unexpected given the short AV interval and the numerous reports that show unchanged or even widened QRSds in therapy responders. 30,38,39
Critique of method
These experiments were not done in chronically diseased hearts, which is required for BiV therapy indication in humans. 1–3 Therefore, application of these findings in acute ischemia to chronically diseased, human, failing hearts requires further validation. Although the animals were not chronically diseased, they did exhibit important aspects seen in failing hearts, such as a wide QRS complex, an LBBB-type activation pattern, various degrees of myocardial ischemia and diminished LV pump function. Further experiments should be completed to understand BiV therapy response related to myocardial perfusion in the diseased failing heart and how therapy may be augmented with increased myocardial perfusion during pacing.
The blood flow through the cannulated coronary artery was measured directly using an inline flow probe and no statistical difference in perfusion was seen between the RA, RV and BiV pacing conditions (Table 1). However, coronary flow to the microcirculation was not measured (e.g. using microspheres). Based on the well-established left dominant nature and consistency of myocardial flow in the canine heart, 34 microsphere measurements did not seem necessary to confirm perfusion regions. Collateral flow was not assessed in this study. At the lowest perfusion rates, the local crystal morphology showed systolic lengthening (Figures 2c and d) indicative of underperfused myocardium. Even if some collateral flow was present at the lowest perfusion pressures, it is clear that the overall flow to the myocardium was not adequate to sustain normal LV function and did not greatly affect BiV pacing response (Figures 1 and 2). While it is clear from this study that overall changes in coronary flow were not seen during BiV therapy, future studies should examine transmural flow distributions throughout the myocardium during BiV therapy to determine how transmural flow may be regulated at various perfusion pressures and pacing conditions.
Two different perfusion rates were used to separate the LAD and LCX experimental groups. These two different rates were used because of the higher coronary flows seen in the LCX versus the LAD groups for the same coronary perfusion pressures. The perfusion often fell below 0.15 mL/min/g in the LAD group at the lowest coronary perfusion pressure, but rarely reached such a low concentration in the LCX group. Thus, it was important to use a unique perfusion limit for each perfusion territory, near the lower limit of the effective auto-regulation range.
Qualitative data were shown for the local MEDs (Figure 2). At lower perfusion conditions (Figures 2c and d), local shortening was diminished such that local MEDs were largely UD and thus we showed qualitative, rather than quantitative, data.
Significance
The need for effective therapies is substantial, with over six million HF cases in the USA alone. 40 While BiV therapy has been a useful treatment option for many patients, the therapy is currently not effective for all recipients. The identification of a measure to delineate between BiV responders and non-responders is considered a pivotal objective of current clinical cardiac electrophysiology. Since numerous factors seem to be involved in BiV therapy response, no single index is likely to be useful in identifying BiV responders versus non-responders. Therefore, there is an obvious need for additional research related to how all the factors involved in EM dysfunction relate to therapy options.
The present findings suggest that myocardial perfusion may provide additional diagnostic information useful for identifying which patients have an adequate myocardial substrate for responsiveness to therapy. The clinical translation of this finding will require additional animal and human studies using non-invasive imaging modalities, such as positron emission tomography, to prospectively determine whether myocardial perfusion is a key factor related to therapy response.
Conclusions
During pseudo-LBBB with myocardial perfusion ≥0.15–0.25 mL/min/g, LV function is improved more with BiV-LW versus BiV-AW pacing. Improvements in LV function with lateral versus AW pacing were not related to increased overall myocardial flow in the perfusion territory. At myocardial perfusion rates below 0.15–0.25 mL/min/g, BiV therapy response was drastically reduced at either pacing location. Both lead location and myocardial perfusion are important factors involved in acute BiV therapy response in hearts with EM dysfunction. Additional research is needed to determine if myocardial perfusion is an important factor related to BiV therapy response in chronically failing human hearts.
Footnotes
ACKNOWLEDGEMENTS
We would like to acknowledge Steven Moberly and Meredith Kohr for their assistance with the animal experiments. This research was funded in part by the National Institutes of Health grant HL-084529 and a grant (0810055Z) from the American Heart Association.