
Abstract
Breast prostheses have been criticized for being responsible for triggering systemic autoimmune disease. The presence of breast implants causes a natural foreign body reaction characterized by the infiltration of macrophages and T-cells. Using PubMed, Medline and eMedicine, we performed a systematic literature review on the stages of periprosthetic capsule formation and cells involved in order to understand which immunological pathways could be responsible for giving rise to, and the development of, connective tissue disease such as systemic sclerosis. We focused on the relationship between tissue growth factor-β, interleukin (IL)-1, IL-6 and T helper 17 or T regulatory cells, as well as on their effects on the different steps of capsular tissue formation. A disturbance in the modulation of these key cytokines may be responsible, in susceptible individuals, for a perpetuation of the inflammatory reaction which can locally lead to capsular contracture and at the systemic level may contribute to triggering autoimmune diseases.
Introduction
Since its discovery, silicone has been considered biologically inert and has been used in many medical devices including artificial valves, joints, needles and teats. 1 Due to its characteristics, in the 1960s, silicone became the major component of breast implants and was used to form the prosthetic surface and content. After an initial period in which the silicon breast implant (SBI) had a smooth silicon surface and fluid silicone inside, the surface was textured and in some cases coated with polyurethane, and fluid silicone was gelled in order to prevent the risk of capsular contracture; the typical foreign body reaction mounted by the immune system which is unable to reject the prosthesis through phagocytosis. 2–4 In fact, the presence of phagocytes adhering to the outer surface of the prosthesis was reported. 5
Three types of prosthetic surface, round or anatomical, united by the presence of silicon as its components are currently available on the market: (1) smooth surface (not much used); (2) textured surface characterized by pores or microvilli (depending on home manufacturer) that allow the implant to be anchored to the surrounding tissue and thus remain in place (most used); and (3) textured silicone surface coated with polyurethane foam which is used in cases of recurring capsular contracture; in this case, the prosthesis is characterized by a double surface.
Regarding the content, the prosthesis may contain silicone cohesive gel or saline; the latter is widely used especially in the USA where silicone was banned in 1992 because of frequent bleeding from the implants and as a potential inducer of autoimmune connective tissue diseases (CTD).
In recent years, breast implants have been widely used since they are very useful for women in order to reconstruct their body image. However, persistent foreign body reaction, which they may induce, has been implicated in triggering autoimmune diseases, especially rheumatoid arthritis (RA) and systemic sclerosis (SSc). 1,6,7
This occurrence has recently been reported by Shoenfeld and colleagues 8,9 as siliconosis, a part of a new syndrome, named ASIA syndrome, which is the acronym of autoimmune/autoinflammatory syndrome induced by adjuvants. 10 ASIA syndrome mediated by the exposure to silicone (the adjuvant) has been characterized by immune phenomena and the subsequent onset of autoimmune disease defined by general symptoms such as body aches, morning stiffness, dry eyes and mouth and unexplained fever, among other symptoms.
Siliconosis has been studied for many years and has appeared in the literature as a potential link between SBIs and CTD since the 1960s. 11 Initially, there were reports based on a few cases of women with clinical symptoms characteristic of unspecified and/or well-defined connective tissue autoimmune diseases such as SSc or Sjogren's syndrome (SS), conditions in which antisilica antibodies or other autoantibodies were detected.
Later, especially in the 1990s and 2000, researchers also carried out studies using animal models (e.g. New Zealand Black mice versus BALB/c albino mice). However, the great majority of these studies were cross-sectional or case-control studies based on large groups of patients. 12,13 In this last group of studies, autoimmune symptoms, immune cells, including T-cells, and autoantibodies were analyzed in order to explore the relationship between SBIs and the occurrence of CTD.
Some autoimmune diseases such as human adjuvant disease, SSc, RA, systemic lupus erythematosus (SLE), morphea, SS and fibromyalgia have been reported in association with SBI. 1,6,11–14
Notably, some immune abnormalities were found, including changes in CD4+ T-cells and macrophages, autoantibodies such as antisilica and anticollagen, and to a lesser extent, antinuclear antibodies, anticardiolipin, antitireoglobulin and antithyroid antibodies and rheumatoid factor.
However, the studies on the association between breast implants and CTD are contradictory and failed to explain why in some patients SBI may stimulate CTD and why the removal of these implants may reverse the disease 14,15 after a long time ranging from months to years.
Proinflammatory biomarkers, including heat shock protein 60, myeloid related proteins 8-14, procollagen III, circulating immune complexes and antiphospholipid antibodies, were demonstrated in the serum or adhering to the surface of SBI. 16–18 This finding is in keeping with the development of massive capsular fibrosis and contracture, as well as with the induction of autoimmune syndromes, especially in predisposed patients.
Since the presence of breast implants causes a natural foreign body reaction characterized by the infiltration of macrophages and T-cells, and since these cells are involved in the development of CTD in implant carriers, we reviewed the stages of periprosthetic capsule formation and the cells involved in order to understand which immunological pathways could be responsible for triggering and developing CTD such as SSc.
We performed a systematic review using PubMed, Medline and eMedicine as the source and the following words: breast implant, periprosthetic capsule, mammary capsule, autoimmune diseases, autoimmune disorders, breast capsule and immunology.
The periprosthetic capsule and CTD
Capsular formation is a dynamic inflammatory process, and the frequent bleeding of silicone from the SBI's surface, due to the mechanical presence of the implant, can transform a ‘normal foreign body reaction’ to a chronic inflammatory process. The continuous stimulation of a foreign body reaction is confirmed by many histological studies that have described the development of granuloma years after implantation. 4,19
In normal subjects, this process can lead to capsular contracture, but in genetically predisposed individuals, chronic inflammation could give rise not only to a fibrotic capsule with subsequent capsular contracture, but may also stimulate an autoimmune response 20 characterized, for example, by anticollagen autoantibodies. 21 Initially, the immune system tries to reject the implant, inducing a foreign body reaction that due to the implant's size, isolates the implant from the surrounding tissue, thus making a new tissue (a granulation tissue).
This first step is characterized by the infiltration of CD68+ macrophages 2,22–24 mixed in the inner layer with secretory cells producing proteoglycans in order to lubricate the space between the capsule and the implant. 25
In this stage, macrophages produce cytokines such as tumor necrosis factor α (TNF-α), interleukin (IL)-1 and IL-6, 26,27 leading to an acute inflammatory response and recruitment of other immune cells including T-lymphocytes. These cells are reported as CD4+ T helper (Th) cells 28–30 which could be activated by antigens like silica particles derived from the implant surface to produce IL-2 31 and probably IL-6 with the consequent activation of B-cells 32 and production of antisilica antibodies observed in capsular biopsies by some authors. 33,34
TNF-α and tissue growth factor β (TGF-β), produced by macrophages and activated T-cells, may stimulate neoangiogenesis and fibroblast growth with the formation of proteins such as collagen and connective tissue, leading to the transformation of the foreign body reaction in a fibrotic capsule. Notably, using indirect immunohistochemistry, Kuhn et al. 35 detected TGF-β1 and TGF-β2 in all of the fibrotic capsules.
TGF-β reduces and abrogates immune and inflammatory responses by inducing T regulatory cells (Treg)
36,37
(Figure 1).
Immunological steps in capsular formation. (a) Foreign body reaction characterized by macrophages that produce tumor necrosis factor α (TNF-α) and interleukin (IL)-1 and IL-6, and by the presentation of silica particles to T-cells; (b) CD4+ T-lymphocytes and macrophages: note the production of IL-2 and IL-6; (c) activated CD4+ T-cells and B-cells with antibodies: note the production of tissue growth factor-β (TGF-β); and (d) fibrotic capsule formation with fibroblasts and collagen
Based on the immunological steps of capsular formation, cytokines, especially TGF-β, and the new class of lymphocytes Th-17, poorly susceptible to the anti-inflammatory effects of TGF-β, seem to play a major role in the development of CTD induced by SBI. 38
In fact, IL-1 and IL-6 have been implicated in the differentiation of Th cells into Th17, which produce IL-17, and seem to be responsible not only for the transformation from acute to chronic inflammatory responses, but also for the onset and maintenance of autoimmune diseases such as RA. 39–46
The balance between Treg and Th17 cells is a critical issue in maintaining an inflammatory process and preventing an autoimmune response. 47,48
In a normal subject, the activation of fibroblasts, resulting in deposition of extracellular matrix (ECM), leads to a down-regulation of the inflammatory reaction and its transformation into a fibrotic reaction. However, in genetically predisposed individuals, the continuous stimulation, due to the presence of the implant, leads to a perpetuation of an immune inflammatory response.
The continuous activation of macrophages and the production of TNF-α, IL-1 and IL-6 prolongs the inflammatory response with production of large amounts of Th-17. 46,48–50 The production of IL-1 and IL-2 promotes the switch in Treg/Th17 cell balance in favor of Th17 cells. 51
TGF-β stimulates the overproduction of IL-6 and fibroblast growth factor, resulting in fibroblast proliferation and ECM deposition. 52 Specifically, TGF-β, in addition to stimulating macrophages with positive feedback, is able to induce the differentiation of fibroblasts into myofibroblasts which present alpha smooth muscle actin in the cytoskeleton and are responsible for contraction of the scar and deposition of proteoglycans and collagen III. 53–55
Activated macrophages and fibroblasts produce angiotensin II, which, by means of nicotinamide adenine dinucleotide phosphate (NADPH), leads to further production of TGF-β1 and subsequent reactivation of the inflammatory process described above. 45,47
TGF-β1 and IL-6 can, in turn, induce the differentiation of naïve Th cells, which have never come into contact with silicone before, into Th17 by activating the RORC2 gene. 48,56
Notably, the presence of Th17, the over-expression of TGF-β1 and the over-production of fibroblasts and ECM (collagen and proteoglycans III), may be responsible, in susceptible individuals, for a perpetuation of the inflammatory reaction which locally can lead to capsular contracture and at the systemic level may contribute to triggering autoimmune diseases, especially SSc.
57
This autoimmune disease is characterized by the deposition of procollagen III and proteoglycans in the skin, lungs, heart and other organs, and seems to be related to fibroblast proliferation and TGF-β gene overexpression which could stimulate fibroblasts, in an autocrine fashion, to produce more collagen
52,56–60
(Figure 2)
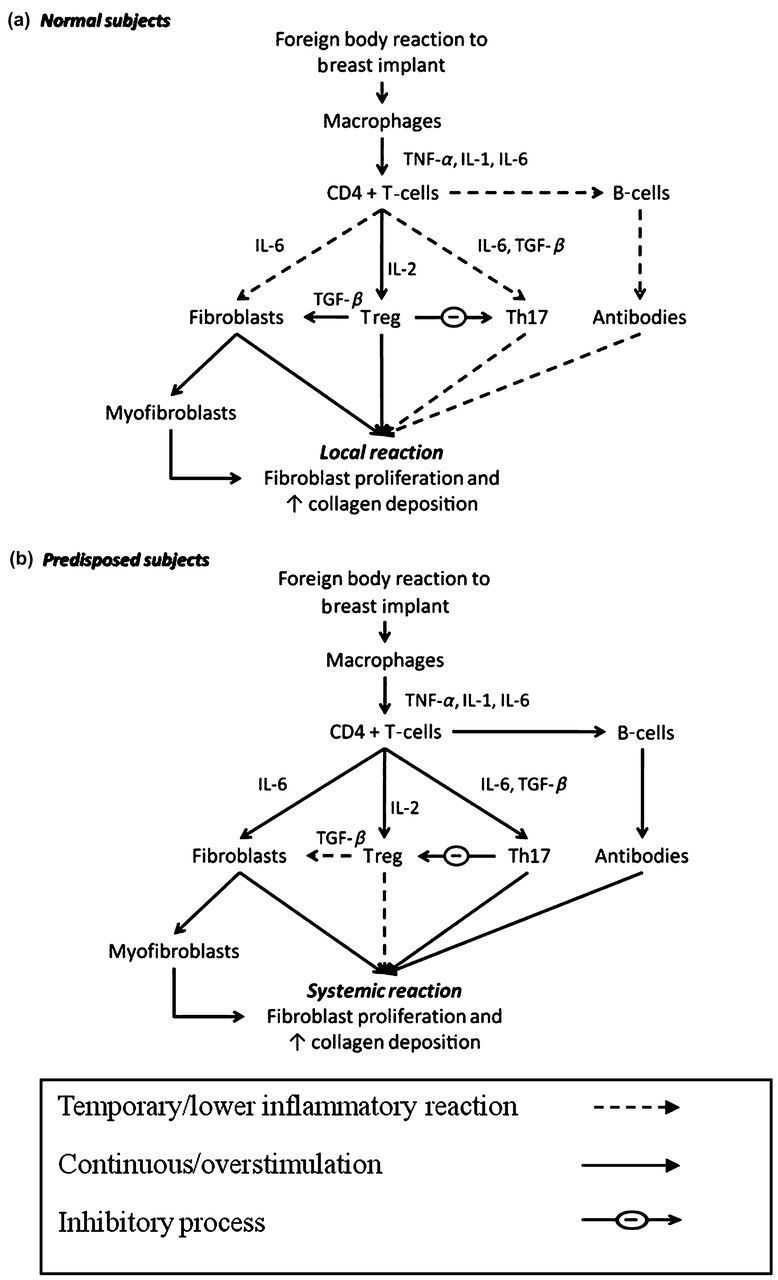
Immunological response following breast implants depends on genetic background of patients. (a) Normal subjects with local reaction: note the temporary stimulation of immune inflammatory reaction and the subsequent marked response of T-regulatory cells with moderate production of collagen fibers and inhibition of T helper 17 production; (b) genetically predisposed subjects with systemic reaction: note the continuous stimulation of the immune inflammatory reaction with consequent overproduction of collagen fibers and lower activation of T-reg cells and their inhibition by Th17. TNF-α, tumor necrosis factor α; IL, interleukin; TGF-β, tissue growth factor β
Potential treatment
The involvement of TGF-β could open many new approaches to the therapy of fibrotic capsules and surrounding inflammation. Using a rat model, it has been shown that the local application of oligonucleotides targeting connective tissue growth factor (CTGF) and TGF-β can reduce CTGF and capsular formation. 61
More recently, Zimman et al. 62 have noted a reduction of TGF-β1, anticollagen III monoclonal autoantibodies and periprosthetic fibrosis in rats treated with angiotensin converting enzyme inhibitors (enalapril) which block the renin–angiotensin system and consequently the inflammatory and profibrotic effects of angiotensin II.
Notably, 9-cis-retinoic acid, an antifibrotic drug, increased cyclooxygenase 2 expression and prostaglandin E2 production, inhibiting the expression of CTGF as well as type-I and -III collagen in scleroderma cultured fibroblasts. 63
The use of leukotriene receptor antagonists, zafirlukast and montelukast, which showed antifibrotic potential, is controversial. Initially developed as a treatment for asthma, zafirlukast was demonstrated to reduce capsular thickness impairing collagen density. Even this effect could be useful in order to prevent capsular fibrosis and contracture. However, there are some reports on the occurrence of Churg–Strauss syndrome 64 in patients treated with leukotriene receptor antagonists and a direct immunomodulatory role for these drugs in the development of vasculitis has been postulated. 65,66
Recently, Lina et al. 53 reported a reverse in the Th1/Th2, Th17/Treg imbalance in patients with RA treated with a therapeutic strategy based on the combined treatment with methotrexate (MTX) and etanercept. The authors demonstrated that etanercept and MTX play an immunomodulatory role on the cytokines involved in the capsular process (IL-1, IL-6, TNF-α, TGF-β and IL-17), ameliorating RA by normalizing the imbalance between Th17 and Treg.
Thus, some drugs, such as anti-TNF-α, might play a role by inhibiting not only the local, but also the systemic, inflammatory responses.
Conclusion
Although the causal role of SBI on CTD cannot be considered conclusive, we speculate that some genetically predisposed individuals may develop CTD because of the stimulation provided by a foreign body. The continuous stimulation of the immune system might also explain why the lag-time between SBI and CTD onset can vary from months to years. The possibility of using new therapeutic strategies could reduce both the risk of capsular contraction and systemic diseases.
Footnotes
ACKNOWLEDGEMENTS
No funding was obtained for this study.