
Abstract
The isolated perfused rat kidney technique is one of the most widely used methods in renal research. It has proven useful to investigate biochemical, physiological, pharmacological and pathophysiological aspects of renal function, allowing variables to be changed in a controlled manner and eliminating systemic influences. This study was designed to test a new surgical procedure to isolate both kidneys for their utilization in this technique, mainly as a vascular preparation. The viability of the resulting preparations was compared with those obtained by the classical method, analyzing the responsiveness to the vasoconstrictor phenylephrine and to the endothelium-dependent vasodilator acetylcholine. Vascular reactivity was evaluated under normal conditions and in endothelium-denuded preparations. The dose response curves to phenylephrine and to acetylcholine were similar in the three experimental groups, regardless of the procedure used for kidney isolation, in both endothelium-intact and endothelium-denuded preparations. We give a step-by-step description of the isolation method and key points for the success of the technique. In conclusion, the surgical procedure proposed in this paper reduces the number of animals required by half and hence reduces the cost of the experiments. This novel procedure is of special interest for acute experiments to test new vasoactive drugs and for analysis of the action mechanisms of these drugs. It could also be used in chronic studies or in genetically modified animals when different experimental protocols are performed on the left and right kidneys and to improve the accuracy of the results by analyzing cases in duplicate.
Keywords
Introduction
Utilization of the isolated perfused rat kidney method derives from pioneering studies by Weiss et al. 1 in the 1950s. Since then, isolated perfused rat kidney preparations have been successfully used as a study model in different scientific approaches to the study of renal function. 2 Its advantages were recently summarized by Hu et al. 3 These authors indicate that: (1) neural and hormonal influences on renal circulation are eliminated, and perfusion pressure and composition can be controlled; (2) vasoactive agents can be administered to the perfusate and (3) tubular and vascular relationships are preserved and the tubuloglomerular feed-back system is intact, and that the circulation network is largely preserved, and pressures, flow and vascular diameters can be directly measured.4,5
The isolated perfused kidney method has recently been used to investigate several aspects of renal physiology, including renin release, 6 other renal secretions7,8 and vascular reactivity.9–11 This approach has also proven useful in analyses of the effects on renal function of high salt intake, 12 ageing,13,14 diabetes,15,16 metabolic syndrome 17 and hypertension,18–20 as well as in pharmacology21,22 and toxicology23,24 studies, and in the characterization of new endogenous vasoactive compounds.25–27 Moreover, basic researchers in Western countries are increasingly faced by limited funds and calls to reduce the use of animals for experimentation.
With this background, we propose a new surgical procedure that allows both rat kidneys to be used in the isolated perfused kidney technique, mainly as a vascular preparation, halving the number of animals used and therefore reducing the cost of the experiments. The viability of preparations so-obtained was tested by comparing the responsiveness to phenylephrine (Phe) and acetylcholine (ACh) in kidneys isolated by the new procedure with the responsiveness in kidneys obtained by the classical method in endothelium-intact and endothelium-denuded preparations.
Methods
Animals
Twenty-four male Wistar rats (18–20 weeks old) born and raised in the experimental animal service of the University of Granada were used in this study. They were maintained on standard chow and tap water ad libitum and randomly assigned to the experimental groups (n = 6 in each group). The experiments were performed according to University of Granada and European Union guidelines for the ethical care and use of laboratory animals.
Surgical procedures
In all surgical procedures, rats were anesthetized with pen-tobarbital sodium (40 mg/kg, intraperitoneally), removing the capsule after exposure of the kidney(s) to avoid renal edema. Immediately after removal of the kidney(s), the animals were killed with an overdose of pentobarbital sodium.
Classical kidney isolation procedure
The operator, sitting at the tail side of the rat, opened the abdomen in cross through a midline incision in the alba line from above the bladder to above the xiphoid process. The left renal and superior mesenteric arteries were exposed. The area around the anastomosis of the superior mesenteric artery, renal artery and aorta was cleared of connective tissue, and loose ligatures were placed around the superior mesenteric artery and renal artery. Continuous renal perfusion was maintained by cannulating the superior mesenteric artery with a beveled blunt needle (18-gauge), which was advanced into the left renal artery and secured with ligatures. The kidney was then excised from its surrounding tissues and removed.
New kidney isolation approach
The surgical procedure is depicted in Figure 1. The abdomen was opened as in the classical procedure. The left renal and abdominal aorta arteries were exposed, cleaned and dissected. A loose ligature was placed around the left renal artery, and the digestive tract was shifted to the right. The abdominal aorta, right renal artery and mesenteric arteries were exposed, forming a cross. These three arteries were cleaned and dissected. Loose ligatures were placed around the proximal aorta and renal artery, and three additional ligatures were placed around the mesenteric artery. Next, the position of the rat was changed to present its left side to the operator, who inserted a beveled 18-gauge needle into the superior mesenteric artery via a small incision and passed it along the superior mesenteric artery, across the aorta and into the renal artery, where it was tied in place. Perfusion was then initiated, and the needle was secured with ligatures when the kidney turned white. The aortic ligature was tied, and the kidney was quickly excised from its surrounding tissues and removed, leaving the distal aorta open. Immediately after removal of the right kidney, the animal was turned so that the head was next to the operator. The operatory field was then cleaned, the blood removed, and the aorta cannulated with a beveled 18-gauge needle. Perfusion was initiated and the needle was simultaneously advanced into the left renal artery, identified by the ligature that had been placed around it. The needle was secured with a ligature immediately the kidney turned white. A special effort was made to minimize the time between right kidney removal and the start of left kidney perfusion (i.e., the period of ischemia for the left kidney), which was reduced to around three minutes. The entire surgical procedure was completed in <15 min by a single operator.

Summary of the surgical procedure for isolating both rat kidneys. (a) A loose ligature is located around the left renal artery, and the digestive tract is moved to the right. (b) Abdominal aorta, right renal artery, and mesenteric arteries are cleaned and dissected and loose ligatures are located around the proximal aorta and renal artery, and three additional ligatures are placed around the mesenteric artery; these manipulations are performed from the left side of the animal. (c) The superior mesenteric artery is cannulated with a beveled 18-gauges needle and the needle is passed across the aorta and into the renal artery where it is tied in place. Perfusion is then initiated, and the needle is secured with ligatures immediately the kidney turns white. (d) The aortic ligature is tied and the right kidney quickly excised from its surrounding tissues and removed, leaving the distal aorta open. (e) The blood is removed and the aorta immediately cannulated with a beveled 18-gauge needle. (f) Perfusion in the left kidney is initiated. (g) The needle is advanced into the left renal artery and secured with a ligature. (h) Finally left kidney is removed these manipulations are performed from the head side of the rat. (A color version of this figure is available in the online journal)
Experimental protocols
The kidneys were perfused at a constant flow rate (5 mL/g of kidney weight/min) by means of a roller pump (IPS-4, Ismatec S.A. Zürich, Switzerland) with Tyrode solution (37°C) composed of (mmol/L): NaCl (137), KCl (2.7), CaCl2 (1.8), MgCl2 (1.1), NaHCO3 (12.0), NaH2PO4 (0.42) and D(+) glucose (5.6) and aerated with 5% CO2 in O2. The kidney was placed in a chamber containing the non-recirculated perfusate lost from the renal vein maintained at 37°C. A TRA-021 transducer connected to a two-channel Letigraph 2000 recorder (Letica S.A., Barcelona, Spain) was used to record renal vascular responses as changes in the renal perfusion pressure (RPP) downstream from the pump. A stabilization period of 30 min was allowed before commencing the experiments. Bolus injections (50 μL/g of kidney weight) of the agonists (vasoconstrictor and vasodilator) were administered into the perfusion system close to the kidney. Injection of these volumes caused a small, transient increase in RPP that preceded the agonist-evoked response. A control injection of vehicle was made in each preparation to verify that the responses to drug injections were not artifacts. The minimum time between successive doses of agonist was five minutes. When necessary, these periods were extended until the previous response had disappeared.
The renal vasoconstrictor response to Phe and, subsequently, the endothelium-dependent vasodilator responsiveness to ACh were analyzed in the left kidney isolated by the classic method and in the two kidneys isolated by the new approach. The dose–response curves to Phe and to ACh were performed in separate preparations with intact endothelium or in preparations without endothelium.
The endothelium was removed bypassing air in the per-fusion system rather than Tyrode solution through the chosen isolated kidney for 4.5 min. Endothelium removal was assessed by measuring the vasodilator response to a bolus dose (10–8 mol/L) of ACh administered to the Phe-preconstricted vascular bed. The vasodilator response of these preparations to ACh is less than <10%. This method of endothelium removal does not affect vascular smooth muscle cell responses to the nitric oxide donor, nitroprusside (unpublished observations).
After 30 min of equilibration, the dose–response curve to Phe (10–9 to 10–7 mol/L) was performed. After a further 20-min interval, the renal vasculature was preconstricted with a continuous infusion of Phe (10–6 mol/L) in the per-fusion circuit, and the dose–response curve to ACh (10–11 to 10–8 mol/L) was performed when a stable vascular tone was attained.
Because the endothelium-denuded preparations evidenced an increased responsiveness to Phe, the concentration of vasoconstrictor was adjusted to achieve a similar level of preconstriction to that observed in endothelium-intact preparations (112±2 mmHg). The approximate mean dose administered to the endothelium-denuded group was 5.10–7 mol/L. Changes in RPP in response to ACh were expressed as the percentage decrease in the vasoconstriction obtained with Phe.
Drugs
Pentobarbital sodium was purchased from Serva (Heidelberg, Germany) and Phe hydrochloride and ACh from Sigma (Madrid, Spain).
Statistical analysis
Nested-design analysis of groups and doses was used to compare dose–responses; the design had two fixed effect factors (group and dose) and one random effect factor (kidney), nesting this factor in the group. Because the tests for group-dose interaction were not significant, groups with different doses were not compared.
Results
Figure 1 provides a step-by-step description of the new isolation method. The basal perfusion pressure values at the end of the stabilization period were similar in the kidneys, regardless the surgical procedure followed: 45.5+0.3 in the left kidney obtained by the classic surgical procedure and 45.2 ± 0.1 and 45.0 ± 0.1 in the right and left kidneys obtained by the new method, respectively. Figure 2 depicts the renal responsiveness to the vasoconstrictor Phe and the endothelium-dependent ACh in rat kidneys isolated and obtained by the classic method and by the new technique. The dose–response curves to Phe and to ACh were virtually identical in all three experimental groups and in endothelium-intact and endothelium-denuded preparations, regardless of the procedure used to isolate the kidney.
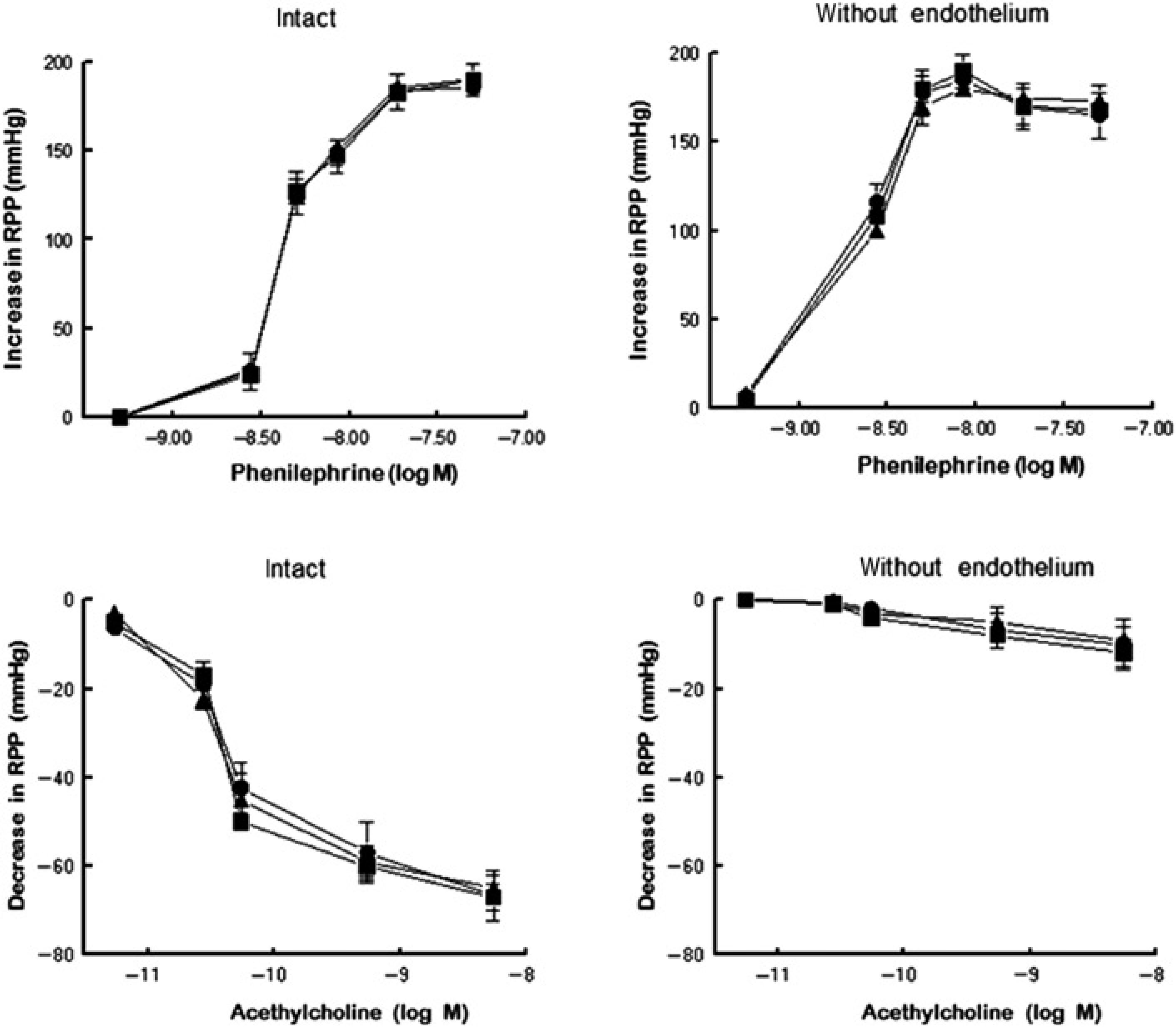
Dose-response curves to phenylephrine and acetylcholine in endothelium-intact (left graphs) or endothelium-denuded (right graphs) kidneys isolated from Wistar rats using the classic surgical procedure (classic) or the new method (right and left) for isolating both kidneys (n = 6 in each group). RPP, renal perfusion pressure. Data are means ± SEM. (•), Control (classic); (▴), left kidney; (■), right kidney
Discussion
Right rat kidneys isolated with this novel surgical procedure, which underwent a brief (2–3 min) period of ischemia, showed the same responsiveness to the vasoconstrictor Phe and to the endothelium-dependent vasodilator ACh as observed in left kidneys isolated by the classical method, both under baseline conditions and after endo-thelium removal. Hence, the endothelium, the vascular structure most sensitive to ischemia, was well preserved in all preparations, regardless of the kidney isolation approach.
The procedure could be modified if the study is concerned about even the brief period of ischemia. Left kidney would be first isolated via the abdominal aorta and then the right kidney via the mesenteric artery. Using this method, it is possible to isolate both kidneys with no cessation of perfusion, but it produces a marked elevation in mean arterial pressure, greater than 20 mmHg, in the right kidney due to the aortic ligature during its period of isolation. Since, aortic ligature is a way to increase blood pressure in pressure-diuresis-natriuresis experiments. 28
The isolated kidney is usually selected as a vascular preparation because it includes the complete renal vasculature with small resistance arteries and arterioles, which are physiologically more relevant to the control of vascular resistance. Furthermore, endothelial and smooth muscle cell function can be studied under different experimental conditions without extrarenal interferences. Research into the mechanisms regulating vascular tone in the kidney are especially relevant, because it receives 20% of cardiac output, and renal hemodynamics play an essential role in the regulation of total peripheral resistance, renal sodium excretion and blood pressure. 29
Adoption of the surgical procedure proposed in this paper would halve the number of animals needed for these experiments and reduce costs. It could be especially valuable in acute experiments to test new vasoactive drugs and analyze the action mechanism of vasoactive compounds. Moreover, it may also be used in chronic studies or in genetically modified animals when different experimental protocols are followed with each kidney and to improve the accuracy of the results analyzing the cases in duplicate.
Footnotes
Acknowledgements
The authors thank R Davies for help with the English version. This study was supported by the Spanish Ministry of Innovation and Science (Grant SAF2009-12294) and by the Carlos III Health Institute of the Spanish Ministry of Health and Consumer Affairs (Red de Investigación Renal, REDinREN RD06/0016/0017 and RD07/0016/2008). FEDER ‘Una manera de hacer Europa’.