
Abstract
Intratracheal administration of lipopolysaccharide (LPS) in animals is a commonly used model of acute lung injury, characterized by increased alveolar-capillary membrane permeability causing protein-rich edema, inflammation, deterioration of lung mechanical function and impaired gas exchange. Technetium-99-m-labeled diethylene-triamine pentaacetatic acid (99mTc-DTPA) scintigraphy is a non-invasive technique to assess lung epithelial permeability. We hypothesize that the longer the exposure and the higher the dose of LPS the greater the derangement of the various indices of lung injury. After 3, 6 and 24 h of 5 or 40 μg LPS intratracheally administration, 99mTc-DTPA was instilled in the lung. Images were acquired for 90 min with a γ-camera and the radiotracer clearance was estimated. In another subgroup, the mechanical properties of the respiratory system were estimated with the forced oscillation technique and static pressure-volume curves, 4.5, 7.5 and 25.5 h post-LPS (iso-times with the end of 99mTc-DTPA scintigraphy). Bronchoalveolar lavage (BAL) was performed and a lung injury score was estimated by histology. Lung myeloperoxidase (MPO) activity was measured. 99mTc-DTPA clearance increased in all LPS challenged groups compared with control. DTPA clearance presented a U-shape time course at the lower dose, while LPS had a declining effect over time at the larger dose. At 7.5 and 25.5 h post-LPS, tissue elasticity was increased and static compliance decreased at both doses. Total protein in the BAL fluid increased at both doses only at 4.5 h Total lung injury score and MPO activity were elevated in all LPS-treated groups. There is differential time- and dose-dependency of the various indices of lung injury after intratracheally LPS instillation in rats.
Introduction
Acute respiratory distress syndrome (ARDS) is a devastating clinical state with great morbidity and mortality, characterized by increased lung permeability causing protein rich edema, inflammation, deterioration of lung mechanical function and impaired gas exchange. 1 Lipopolysaccharide (LPS) is present at the outer membrane of Gram-negative bacteria and its intratracheal administration is a commonly used animal model of acute lung injury (ALI)/ARDS. 2
Technetium-99-m-labeled diethylene-triamine pentaacetatic acid (99mTc-DTPA; molecular weight 492 Da) is a small hydrophilic solute, whose clearance from the lungs, when inhaled or intratracheally instilled, is primarily limited by the epithelial integrity. 3 Therefore, the measurement of 99mTc-DTPA clearance from the lungs has been suggested as a useful, non-invasive technique for assessing the integrity and function of the alveolar-capillary barrier.4,5 In humans, 99mTc-DTPA clearance has been used as an index of lung permeability in various diseases states, including ARDS.6–10 In animals, the administration of 99mTc-DTPA is either given as an aerosol or instilled as a bolus into the tracheobronchial tree. 11 In several different animal models of endothelial and epithelial injury that result in pulmonary edema, including LPS-induced lung injury, 99mTc-DTPA exhibits accelerated clearance.11–18
An important functional consequence of ALI is the deterioration of lung mechanics, mainly due to the development of pulmonary edema, microatelectasis and cellular infiltration. 19 Assessment of lung mechanics is used to evaluate lung injury in animal models of ALI. 20 LPS-induced lung injury in animals has been found in numerous studies to decrease lung compliance, as assessed by various techniques, such as static pressure–volume (PV) curves 21 and the forced oscillation technique.22,23
The histological features of ARDS in humans (mainly in the acute phase) include the presence of interstitial and alveolar edema, with infiltration from inflammatory cells, especially neutrophils, intraalveolar hemorrhage and evidence of epithelial and endothelial injury. 24 Endotoxin-induced lung injury is a model of lung injury that reproduces many of the histological features of ARDS.2,25–27
Despite the plethora of studies employing LPS-induced lung injury, data are missing concerning the effects of different doses of intratracheally instilled LPS on lung permeability, as measured by 99mTc-DTPA clearance. The effect of time elapsed since LPS administration on 99mTc-DTPA clearance is also not established. Furthermore, it is not known how 99mTc-DTPA clearance correlates with other indices of lung injury, such as respiratory system mechanics and histology after different doses of LPS and time intervals of LPS administration. This is because the majority of studies on LPS-induced lung injury employ a single dose of LPS and time of assessment and are focusing only on some indices of lung injury, resulting in varying and sometimes conflicting results. We hypothesize that the longer the exposure and the higher the dose of LPS the greater the derangement of the various indices of lung injury would be.
To test our hypothesis, we have employed for the first time a high-resolution, small-animal imaging system (designed for small rodents) that permits for the non-invasive estimation of lung epithelial permeability by acquiring sequential gamma-ray images. LPS-induced lung injury was studied in previously healthy rats using different doses of LPS and time points of assessment. 99mTc-DTPA clearance was related to histology, measurement of bronchoalveolar lavage (BAL) fluid protein, lung myeloperoxidase (MPO) activity and lung mechanics, assessed by the forced oscillation technique and PV curves.
Materials and methods
Animals
Pathogen-free, adult (8–12 weeks old) female Wistar rats (Hellenic Pasteur Institute, Athens, Greece), weighing between 220 and 280 g, were used for these experiments. Food and water were administrated ad libitum. The light– dark phases of the animal facility were controlled by a 12-h cycle. All animal experiments were reviewed and approved by the Veterinary Services of the Prefecture of Athens and the Ethical Committee of Evangelismos Hospital. Care and handling were in accordance with the European Community guidelines for animal experimentation.
LPS administration
Animals were anesthetized with an intraperitoneal injection of ketamine (75 mg/kg) and xylazine (5 mg/kg) and placed in a supine position at 458. The trachea was exposed with a midline excision and a dose of LPS (Pseudomonas aeruginosa serotype 10; Sigma-Aldrich, Munich, Germany) diluted in 0.2 mL of sterile phosphate-buffered saline (PBS) was instilled into the trachea followed by a flush of 1 mL air. The excision was then sutured and the animals were left to recover from anesthesia. Two different doses of LPS were studied: 5 and 40 μg. Similar doses are commonly used in studies of LPS-induced lung injury and result in adequate inflammatory response in the lung and in increased alveolar capillary membrane permeability following intratracheal LPS administration in rats.28,29 Sham operated animals injected intratracheally with 0.2 mL of sterile PBS alone, served as control.
Lung clearance studies
99mTc-DTPA clearance measurements were started after 3, 6 and 24 h of LPS administration. The decision to study these time points was based on our primary interest in the time dependency of the acute LPS-induced lung injury, to test for techniques that could potentially provide early indications for the presence of lung dysfunction.
Tracer administration
Preparation of 99mTc-DTPA was performed not later than 30 min prior to administration using a standard kit (TechneScan® DTPA, Mallinckrodt Inc., Hazelwood, MI, USA). To verify the labeling procedure, the tracer was periodically sampled and its radiochemical purity was determined using descending paper chromatography. The rats were anesthetized with an intraperitoneal injection of ketamine (75 mg/kg) and xylazine (5 mg/kg). The animals were then tracheostomized (tracheal cannula, 14G, 1 cm length) and a single dose of 600μCi (2.2 MBq) 99mTc-DTPA diluted in 100 μL saline was administrated at end expiration through the tracheostomy, as an aerosol using a MicroSprayer aerosolizer (IA-1C; Penn-Century, Wyndmoor, PA, USA), attached to a high-pressure syringe (FMJ- 250; Penn-Century). This device is an aerosol generator consisting of a sub-miniaturized atomizer located in the tip of a 1.25 stainless steel tube, which is attached to a high-pressure syringe. This device previously showed improved delivery efficiency compared with aerosol inhalation 30 and did not cause adverse pharmacological, toxicological or immunological effects. Moreover, this device has been previously used in rodents (both rats 32 and mice33,34) and despite generating an aerosol with mass-median diameter greater than that used in clinical studies (16-22 /μm), it produces a diffuse (including lung periphery) and even distribution. 33
Immediately after 99mTc-DTPA administration, a 2-mL flush of air was given intratracheally to ensure the patency of the airway. The animals were then allowed to breathe spontaneously throughout the procedure.
Imaging system and image acquisition
The imaging system employed is a high-resolution, compact camera previously described. 35 Briefly, the system consists of three main parts: a gamma-ray scintillation camera, a parallel-hole collimator and support electronics. The camera is based on a pair of two square Hamamatsu (H8500, Hamamatsu Corporation, Hamamatsu City, Japan) flat-panel position-sensitive photomultiplier tubes (PSPMT). The two PSPMTs are optically coupled via an optical grease (RX-688 Optical Coupling Grease; Rexon Inc, Beachwood, OH, USA) to a NaI(Tl) crystal array (Bicron - Saint Gobain Crystals and Detectors, Nemours, France) with an active area of 98 × 48 mm. The pixel size is 1 × 1 mm with a pixel pitch of 1.2 mm. The array is viewed through a 3 mm glass window. The encapsulation is completed by an aluminum cover 50 μm thick. The imaging aperture is a 25-mm thick lead parallel-hole collimator with hexagonal holes 1.2 mm in diameter and 0.2 mm thick septum walls (Tecomet Precision Technologies, Wilmington, MA, USA). The camera system is enclosed in an 8-mm tungsten housing box. Each PSPMT provides four analog signals. A digital signal processing (DSP) board is dedicated for each PSPMT to digitize the analog signals (NI PCI-6110 National Instruments, Austin, TX, USA). Data acquisition, preprocessing and system calibration are carried out using custom software written in Kmax environment (Sparrow Corporation, Port Orange, FL, USA). The system achieves a spatial resolution of ~1.5 mm at the collimator face and degrades linearly with distance.
The spontaneously breathing, anesthetized rats were placed supine on the gamma camera. We collected 45 two-minute images, sequentially for a 90-min period. The time delay between delivery of the radiotracer and commencement of imaging was no more than 45 s. Supplemental doses of anesthesia were given as needed.
Image analysis
99mTc-DTPA clearance measurements were analyzed by manually drawing a region-of-interest (ROI) circumscribing both lungs on the first image (at time t = 2 min) and applying the same ROI on all 45 images to generate a retention– time curve. To test the distribution of the tracer, the pixel area of the initial ROI has been calculated for every animal and was normalized for total body weight. Indeed, for an animal to be included in the study, it had to exhibit relatively uniform distribution of the tracer and/or the tracer had to reach the lung periphery in the first image. Otherwise it was excluded from further analysis, even from the very beginning of the experiment. This was the case for one animal from control group, one animal from 5 μg LPS/24 h, two animals from 40 μg LPS/six hours and one animal from 40 μg LPS/three hours.
All retention data were corrected for radioactive decay and background counts. A closed-loop movie with overlaid ROIs was viewed to ensure no movement took place during the data acquisition. The retention data for each animal were log-transformed and linear or piecewise-linear functions were fitted to determine the time for lung activity of 99mTc-DTPA to reach 50% of the initial value. The clearance half-life, T1/2, was calculated from the slope of the regression line and was used as a marker of alveolar-capillary permeability, since lung clearance of instilled DTPA mainly occurs through the alveolar-capillary membrane to the blood and therefore reflects its integrity.
Lung mechanics measurements
In a different subgroup of animals, lung mechanics were assessed following 4.5, 7.5 and 25.5 h of LPS installation. Those time points were chosen so that a direct comparison can be made between the above subgroup of animals and the animals that underwent 90 min of imaging.
Following LPS administration, animals were anesthetized by intraperitoneal injection of ketamine (75 mg/kg) and xylazine (10 mg/kg), tracheostomized (tracheal cannula, 14G) and connected to a small animal ventilator (FlexiVent, Scireq Corp., Montreal, Canada). Animals were ventilated with a 7 mL/kg tidal volume and breathing frequency of 65 breaths/min. The end expiratory pressure was set to 3 cmH2O. Following one minute of ventilation, the animal was intraperitoneal injected with succinylcholine (8 mg/kg) to cease spontaneous breathing. Three minutes later, three forced oscillation perturbations were obtained with 30 s interval to estimate lung mechanics. Two static PV curves were also performed following one minute of ventilation after the last oscillation perturbation. Results from the repeated measurements in every animal were averaged. Prior to measurements (30 s) the lung volume history was once standardized by simply occluding the expiratory line of the ventilator until the airway opening pressure reached 30 cm H2O. During ventilation, heart rate was monitored to ensure adequate depth of anesthesia and temperature was monitored and kept at normal values (36–37°C) using a thermal probe and a thermal pad.
Forced oscillation technique
The forced oscillation perturbation consists of a pseudorandom waveform of low frequencies (0.5–19.75 Hz) applied for eight seconds with a peak-to-peak volume of 3 mL/kg. Pressure and volume data are recorded and the impedance of the respiratory system is calculated using the Fast Fourier transformation. Impedance (Z) is then fitted to constant phase model:
36
Zrs(f) =Rn + i2π fI + (G - iH)/(2πf)a, where Rn is the Newtonian resistance of the airways, i is the imaginary unit, f is the frequency, I is the inertance of the gas in the airways, G represents tissue viscance (viscous dissipation of energy). H represents tissue elasticity and α can be calculated through the equation a
Static PV curve
Static PV curves of the respiratory system were performed by gradually inflating and deflating the lungs with a total volume of 4.8 mL at seven steps each with a 0.2 s interval. Analysis of the static PV curve was performed by visually identifying lower and upper inflection points and estimating the static compliance of the respiratory system by the slope of the mid linear part of the expiratory limb of the PV curve. 39 Hysteresis (area between inspiratory and expiratory limb) was automatically calculated using the FlexiVent software.
Bronchoalveolar lavage
Following lung mechanics measurements, the animals were sacrificed by exsanguination (vena cava dissection) and the thoracic cavity was exposed. The left lung was temporarily ligated and the right lung was lavaged with three aliquots of 2 mL normal saline. Near 5.5 mL of BAL fluid were withdrawn and were immediately centrifuged (300 ×
Lung histology
Following BAL or 99mTc-DTPA scintigraphy, the right main bronchus was ligated and the left lung was fixed with 4% formaldehyde under 20 cm H2O pressure and removed. After 24 h the lung tissue was embedded in paraffin and cut in serial 5-μm sections. Sections were stained for hematoxylin and eosin. A lung injury score was determined based on the following histological features: (i) focal alveolar membrane thickening, (ii) capillary congestion, (iii) pulmonary edema, (iv) intra-alveolar hemorrhage, (v) interstitial and (vi) intra-alveolar neutrophil infiltration. Each feature was scored from 0 to 3 based on its absence (0 points) or presence to a mild (1 point), moderate (2 points) or severe degree (3 points). 38
Lung MPO activity assay
Following BAL, the right lung was immediately frozen in liquid nitrogen and stored at −80°C. Lung MPO activity was then estimated as an index of neutrophil infiltration. Lung sections were weighed and homogenized (~100mg in 1 mL) in buffer containing 50 mmol/L potassium phosphate (pH 6.0), 5 mmol/L EDTA and 0.5% hexadecyltrimethylammonium bromide. After incubation at 60°C for two hours, the homogenates were centrifuged at 12,000 ×
Statistical analysis
Statistical analysis was performed using the non-parametric Kruskal-Wallis analysis of variance (ANOVA), and when significant, the Mann-Whitney U test was used for between groups comparisons (Statistica software, StatSoft, Tulsa, OK, USA). A P < 0.05 was considered statistically significant. All data are presented as mean ± standard error of the mean (SEM).
Results
Lung 99mTc-DTPA clearance
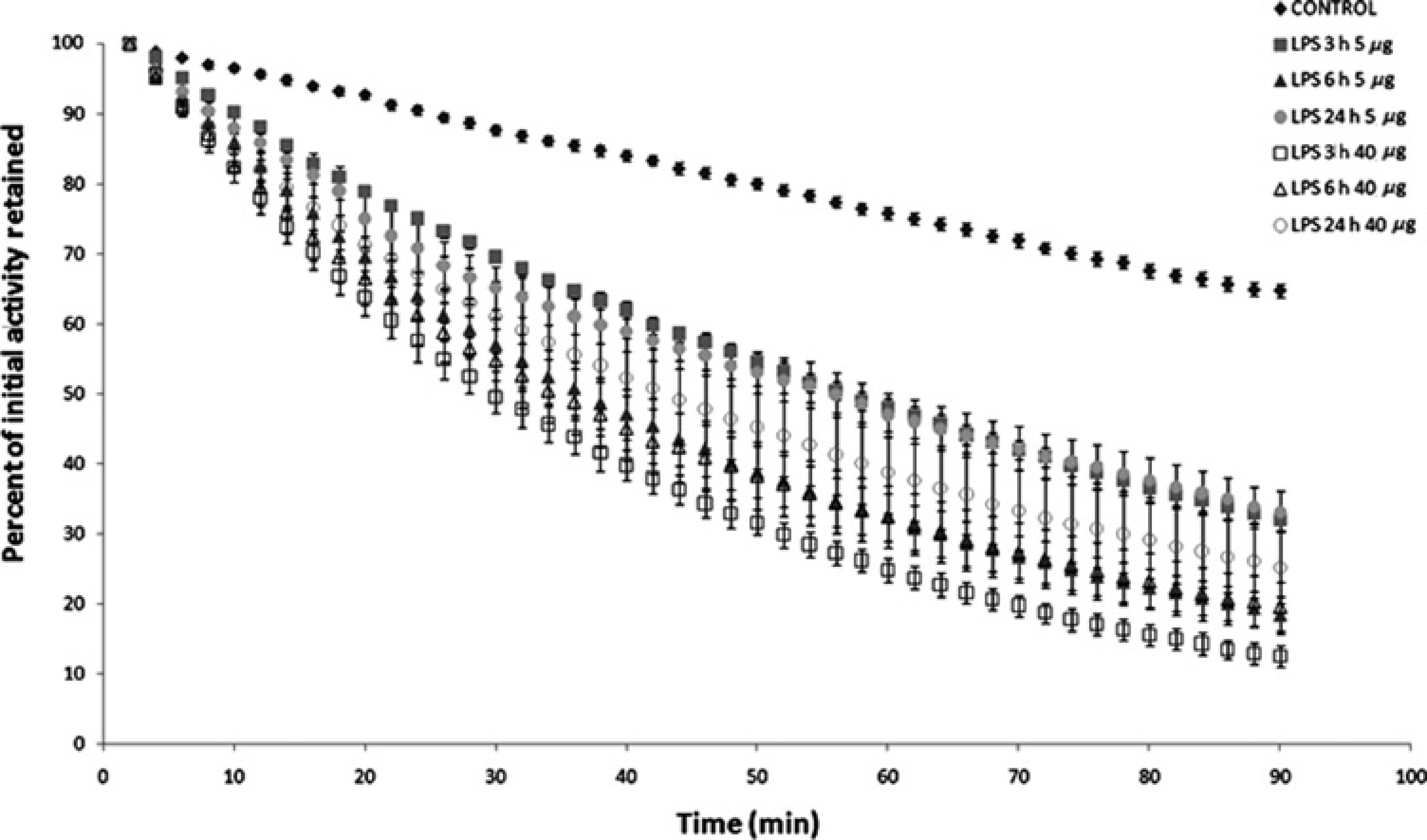
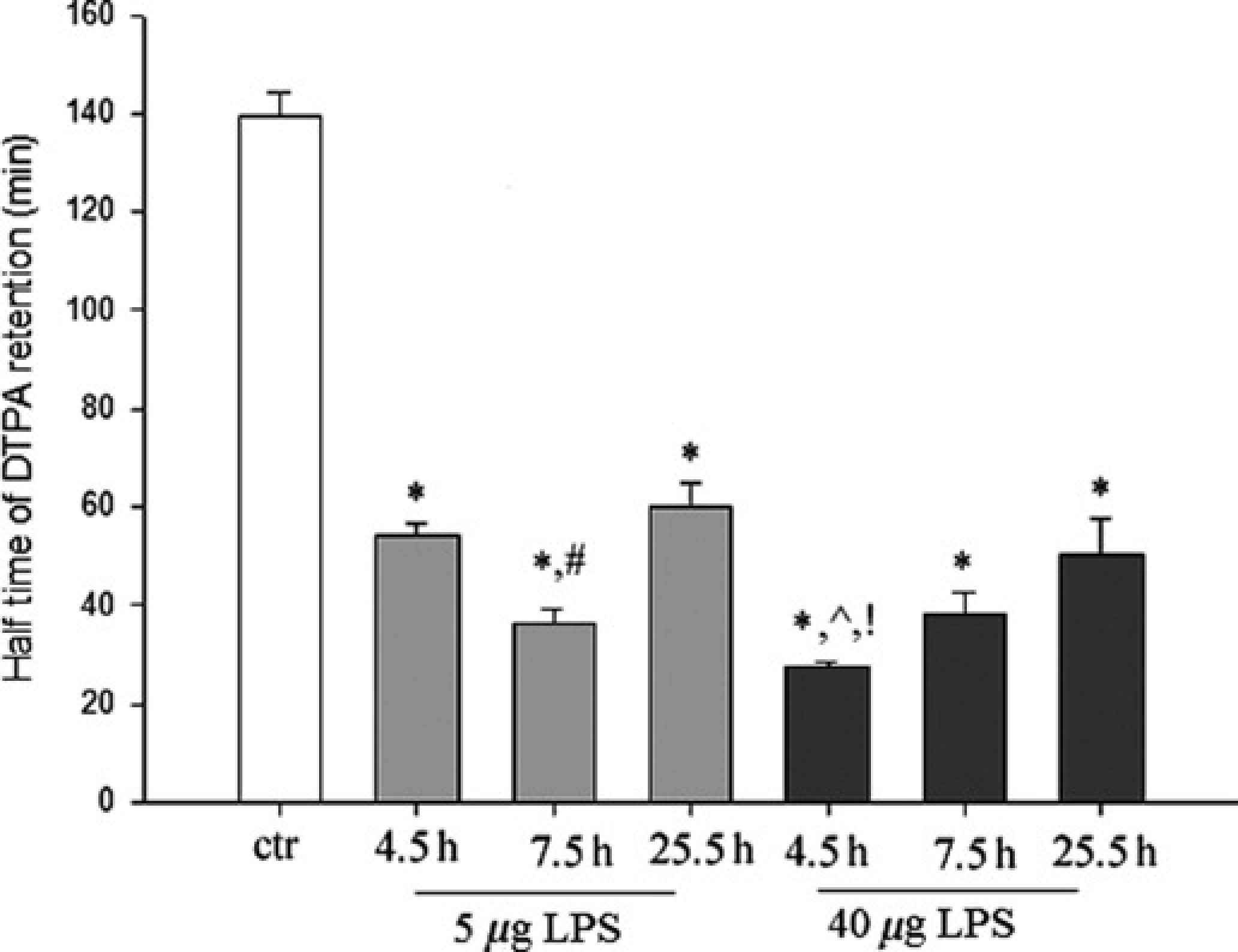
Sham operated animals that were studied after 3, 6 and 24 h presented no significant difference in all studied parameters and were pooled to one group (control). The distribution of the radiotracer (average area normalized for total body weight) presented no difference between experimental groups (Kruskal-Wallis ANOVA, P not significant (P = 0.21), Table 1). As illustrated in Figure 1 (data from representative animals), 99mTc-DTPA clearance from the lungs was significantly faster in all LPS challenged groups compared with the control group. This was reflected by a steeper retention curve (Figure 2) resulting in a shorter T1/2 (Figure 3). The differences between the mean T1/2 of LPS exposed and control rats in all doses and time-points were highly significant (P < 0.001) (Figure 3 and Table 1). Furthermore, the log-transformed retention of the tracer in all groups was well fitted with a linear function. The coefficient of determination (R2) of the linear fitting was above 0.97. This result suggests mono-exponential clearance of the tracer both for the control and the LPS challenged groups.
Gamma-ray images from a representative animal of each group at various times after intratracheal instillation of 99mTc-DTPA (technetium-99-m-labeled diethylene-triamine pentaacetatic acid). All images are displayed with the same color map and color scale. The color intensity represents the magnitude of deposited radiotracer. Note the increased clearance of the tracer in all lipopolysaccharide (LPS) groups compared with the sustained radioactivity of the control group. (A color version of this figure is available in the online journal) Average activity of the administrated 99m The half-life (T1/2) for 99mTc-DTPA clearance is depicted for the seven groups of rats. Lung clearance is significantly more rapid in the LPS group compared with the control group. A U-shape response to time is noticed for the lower dose, while a steadily decreasing over time effect of LPS on DTPA clearance is noticed for the higher dose. Data presented as mean ± 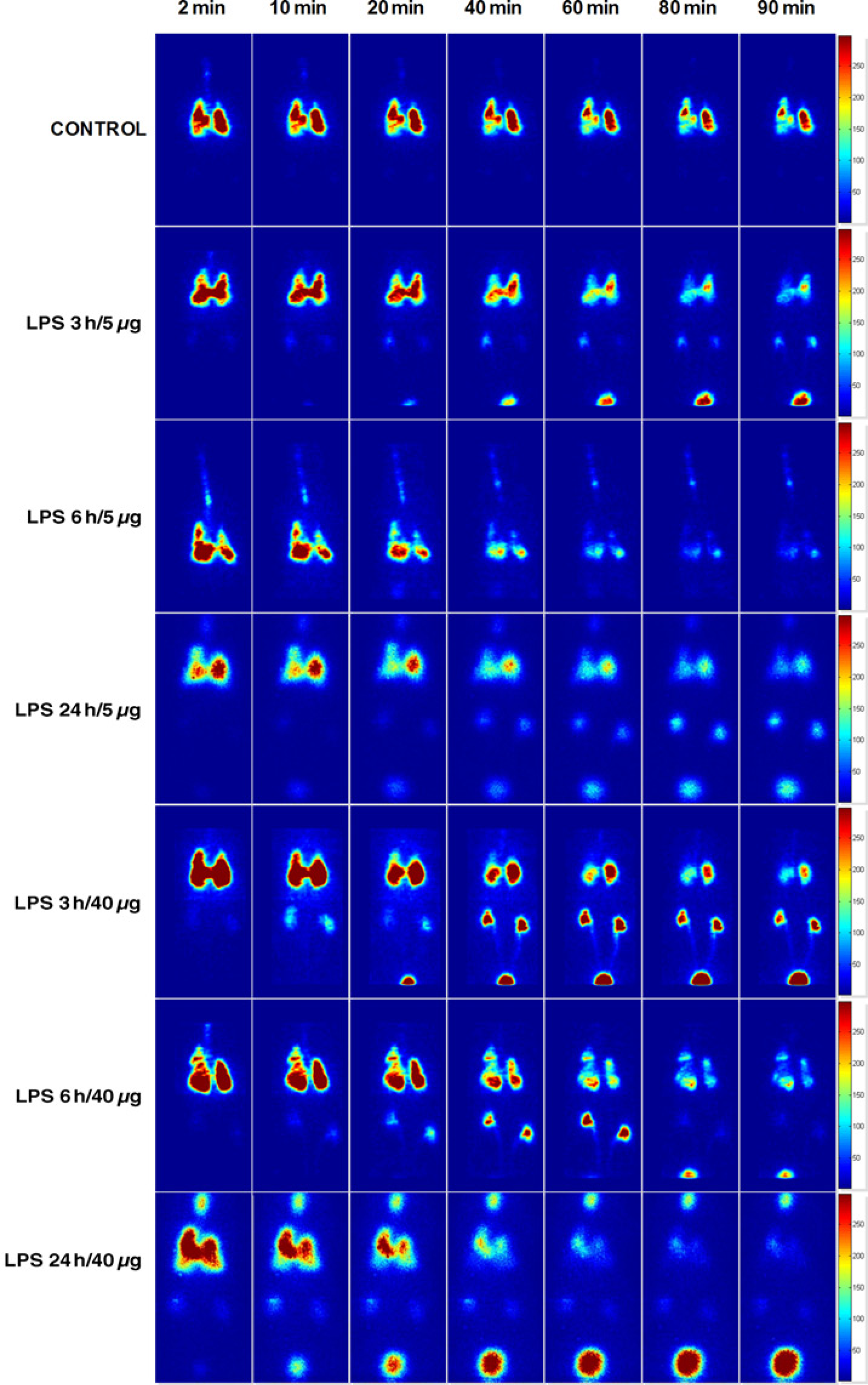
DTPA clearance and lung mechanics following LPS administration

Data presented as mean ± SEM. n
DTPA, diethylene-triamine pentaacetatic acid; LPS, lipopolysaccharide
P < 0.05 compared with control
P < 0.05 compared with other time points equal dose
P < 0.05 compared with 24(25.5) h, equal dose
P < 0.05 compared with other dose, equal time point
Three hours after LPS, the difference in T1/2 between the two doses of 5 and 40 μg was significant (P = 0.002), indicating a faster clearance half-life for the larger dose (Figure 3). On the other hand, 6 and 24 h after LPS there was no significant difference in the mean T1/2 between the two doses. Comparing time points at a specific dose, the mean T1/2 of the 5 μg group presented a U-shape, since clearance at six hours was significantly faster (P < 0.01) compared with 3 and 24 h In contrast, in the larger dose (40 μg) faster clearance of the radio-tracer was noticed early at three hours, decreasing at later time points (Figure 3).
Total protein in BAL fluid
LPS administration increased total protein in the BAL fluid only after 4.5 h both at 5 and 40 μg dose (P < 0.001, Figure 4). However, following 7.5 and 25.5 h protein concentrations in BAL fluid were not different from control values. Indeed, total protein in 4.5 h was significantly higher compared with other time points for the same dose of LPS (P < 0.05; Figure 4).

LPS administration increased total protein in the BAL fluid only at 4.5 h after LPS with both doses (5 and 40 μg), indicating increased permeability of the alveolar-capillary membrane. At 7.5 and 25.5 h after LPS, protein concentrations in BAL fluid were restored to control values. Data presented as mean ± SEM. *P < 0.05 compared with control, #P < 0.05 compared with other time point equal dose, n = 6-10 for different time points and dose. BAL, bronchoalveolar lavage; LPS, lipopolysaccharide
Mechanical parameters of the respiratory system
Constant phase model parameters
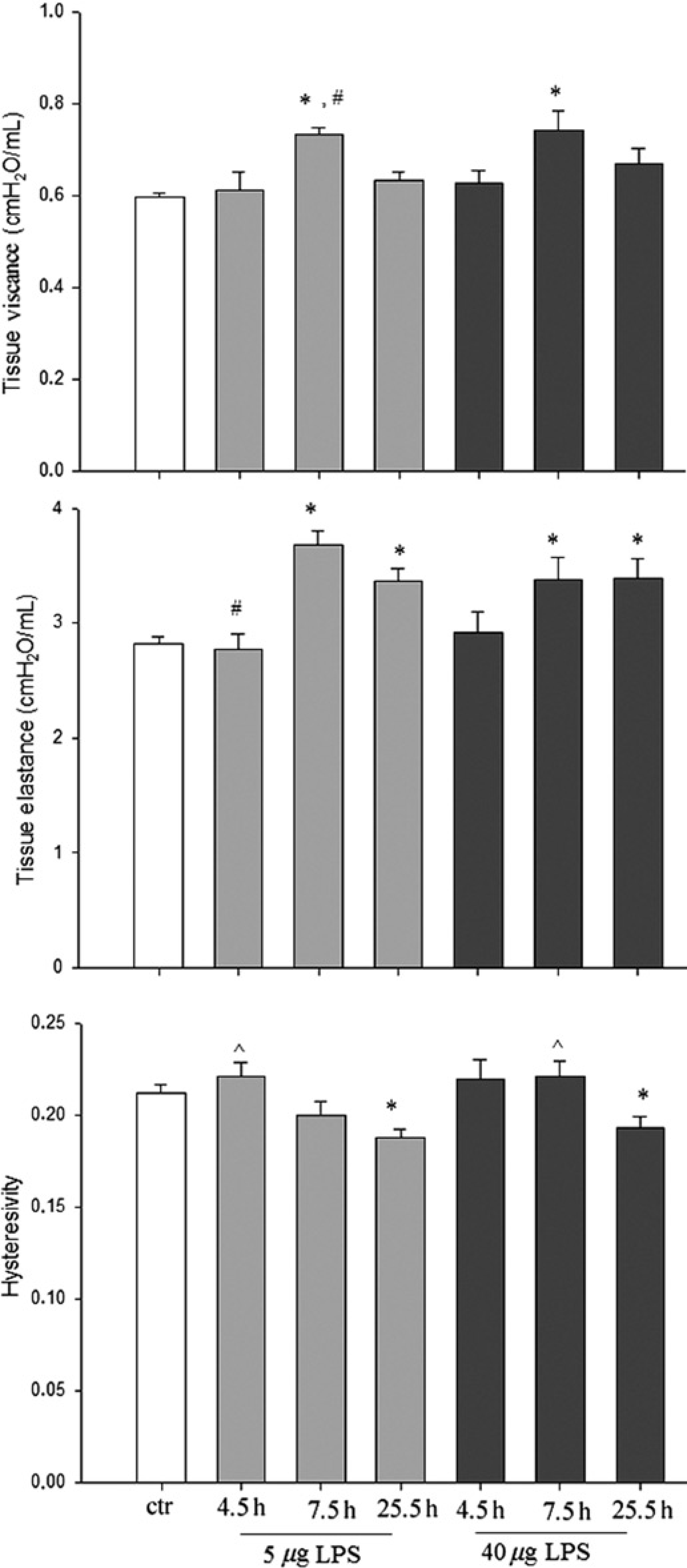
At 7.5 h, both 5 and 40 μg of LPS increased G, as measured with the forced oscillation technique (P < 0.001) (Figure 5 upper and Table 1). Interestingly, the increase in tissue vis-cance was not noticed at 25.5 h following LPS. Tissue ela-stance, an index of pulmonary injury, increased both after 7.5 and 25.5 h of LPS administration at both doses (Figure 5 middle). At 4.5 h after LPS neither tissue viscance nor elastance changed. As a result of the aforementioned changes in the parameters of the constant phase model, hysteresivity (n), the ratio of tissue viscance to tissue elastance decreased at the 25.5 h time point compared with control (P < 0.05; Figure 5 lower).
Mechanical parameters of the respiratory system following intratracheal
Static PV curve
After 7.5 and 25.5 h of LPS administration a downward shift of the static-PV curves was noticed for both 5 and 40 μg dose (Figures 6b and d, respectively). Thus, decreased compliance of the respiratory system was measured for both 5 μg (7.5 h P < 0.001, 25.5 h P = 0.001) and 40 μg (7.5 h P = 0.006, 25.5 h P 0.013) doses of LPS (Figure 5a). Static compliance was unaffected after 4.5 h of LPS administration. Hysteresis of the PV curve was also increased at 7.5 h following LPS instillation at both doses (P < 0.001 and P = 0.006; Figure 6c). On the other hand, after 4.5 of LPS no effect on PV curve hysteresis was observed. After 25.5 h of LPS administration, hysteresis was increased only at the larger dose (40 μg LPS, P = 0.047).
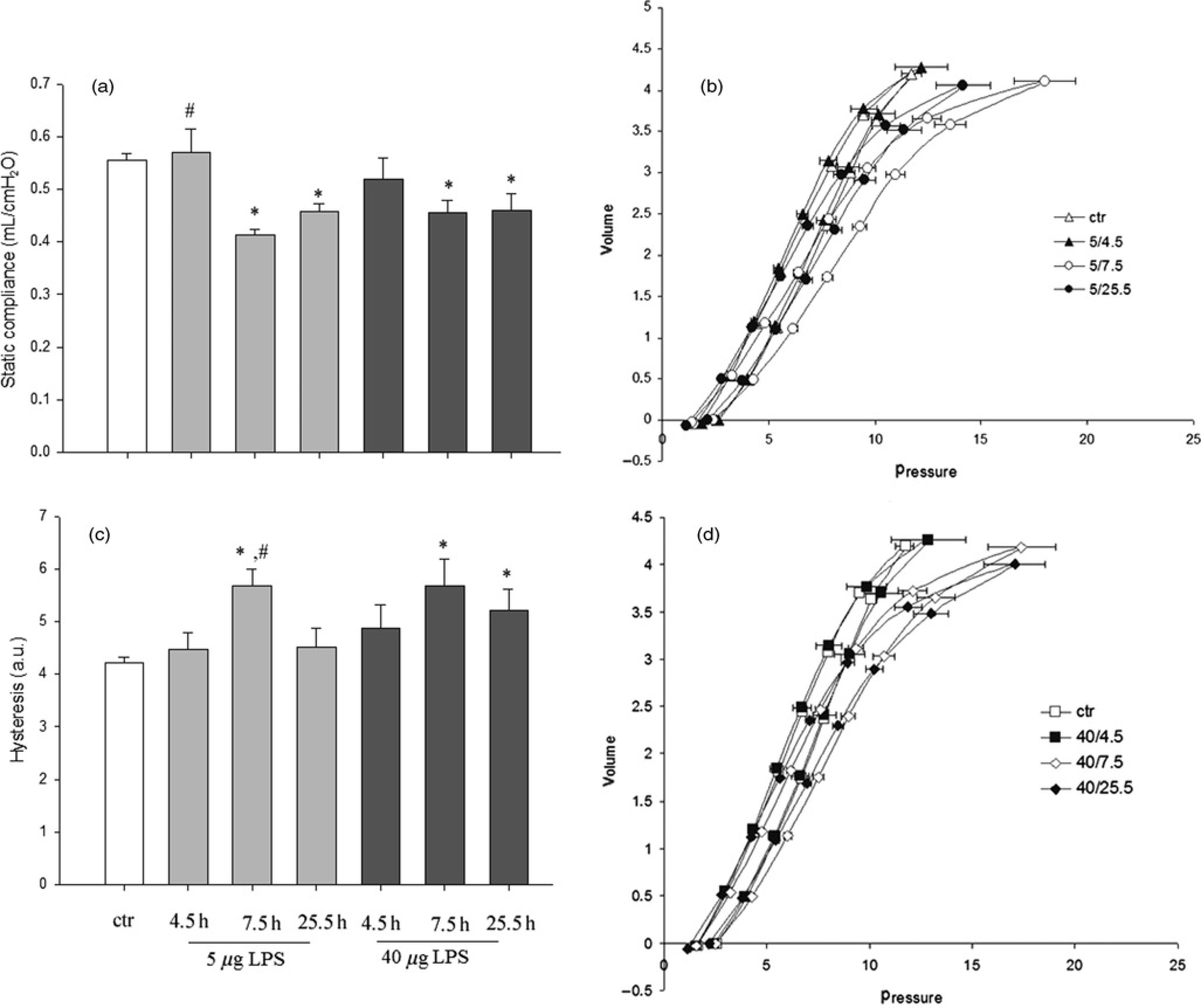
Mechanical parameters of the respiratory system measured by static pressure-volume curves. (a) LPS administration decreased the static compliance of the respiratory system after 7.5 and 25.5 h for both doses used, as indicated by the downward shift of the static pressure-volume curves (5 μg-(b), 40 μg-(d)). Hysteresis was increased only at the 7.5 h time point for the lower doses, while after 7.5 and 25.5 h for the higher dose (c). *P < 0.05 compared with control, #P < 0.05 compared with other time points equal dose, n = 6-10 for different time points and dose. LPS, lipopolysaccharide
Lung injury score
Total lung injury score was elevated after LPS administration at every time point and dose compared with control (Figure 7). Between LPS challenged groups, a significant increase of lung injury was found after 25.5 h of the higher dose compared with other time point of the same dose and compared with the same time point of the lower dose (P < 0.05). Regarding each parameter, focal thickening, capillary congestion, intra-alveolar hemorrhage and interstitial neutrophil infiltration score were increased in all LPS-treated groups (Figure 8). Pulmonary edema was only noticed at 4.5 and 7.5 h time point, while not observed at 25.5 h At the lowest dose, intra-alveolar neutrophil infilatration was noticed at all time points, while at the higher dose only at the 25.5 h time point. Both interstitial and intraalveolar neutrophil infiltration after 25.5 h of 40 μg LPS was significantly increased compared with the lower dose (at the 25.5 h).
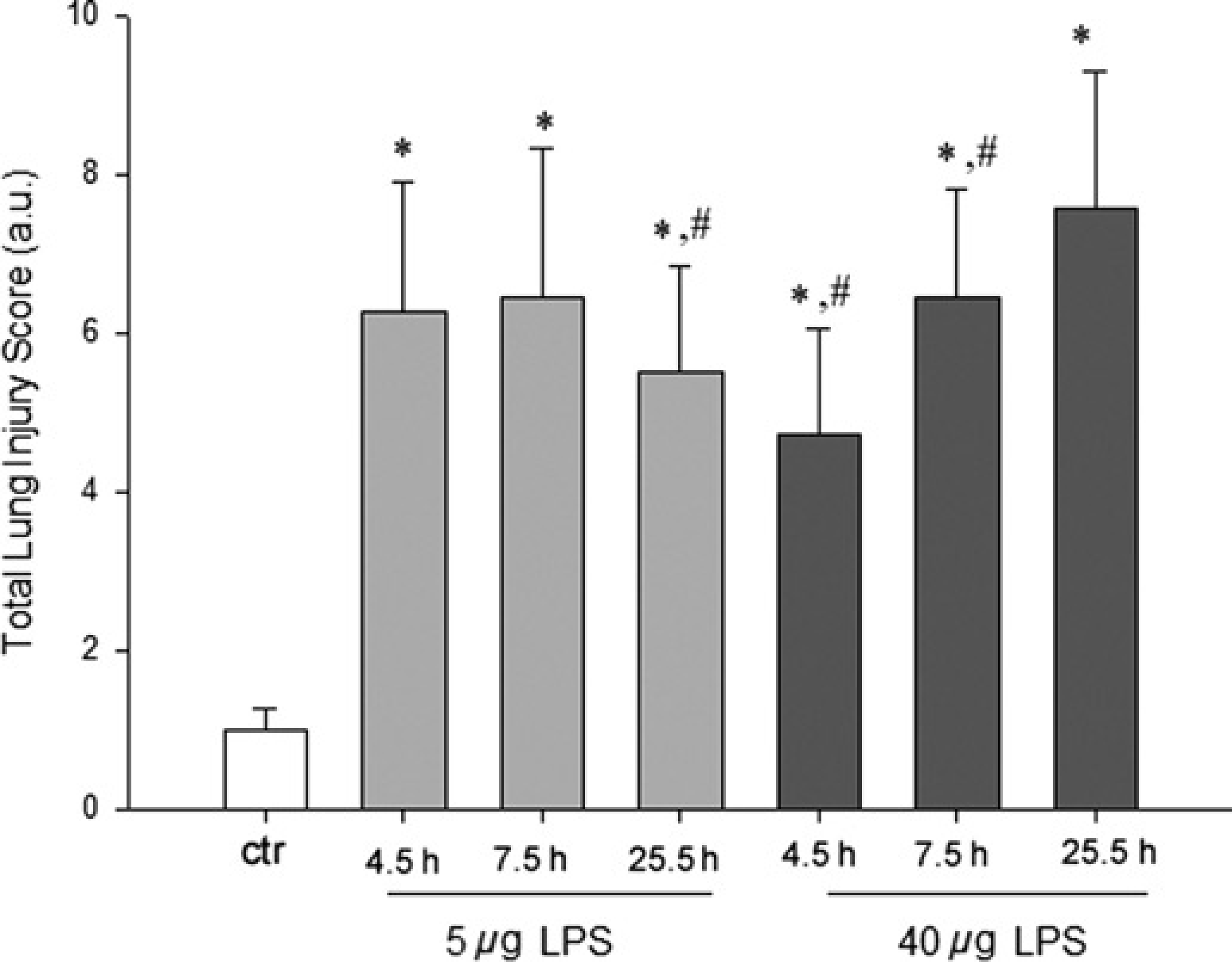
Total lung Injury score was elevated following
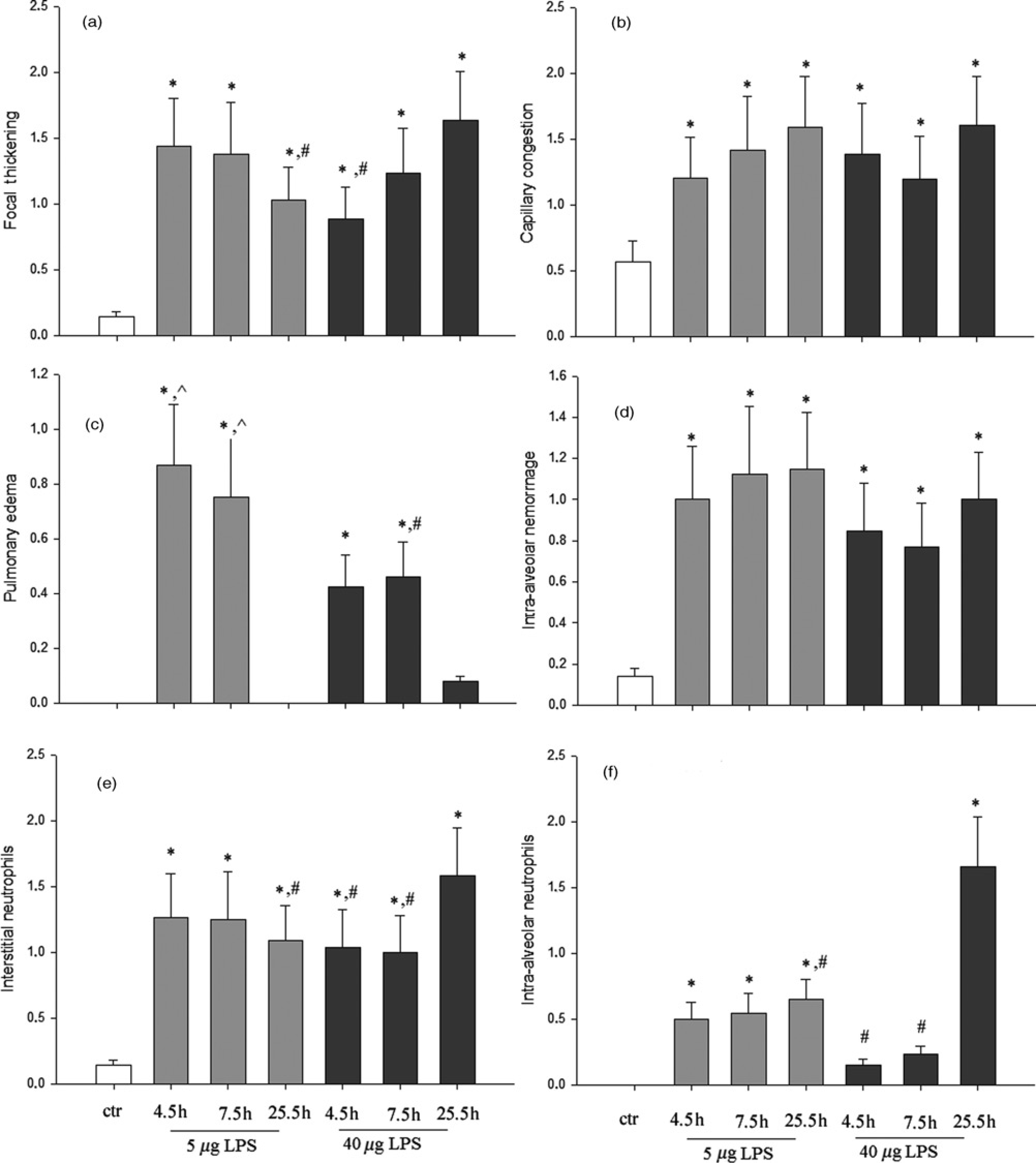
Differential presentation of the histological features contributing to total lung injury score. Focal thickening of the alveolar membrane (a), capillary congestion (b), intra-alveolar hemorrhage (d) and interstitial neutrophil infiltration (e) increased in all
Lung MPO activity assay
In accordance with the results obtained by pathology showing neutrophil infiltration in the lungs following LPS administration, MPO activity was also increased at all time points (P < 0.001) Interestingly, at the larger dose (40 μg) MPO activity was significantly higher after 25.5 h of LPS, compared with 7.5 h (P = 0.03) (Figure 9).
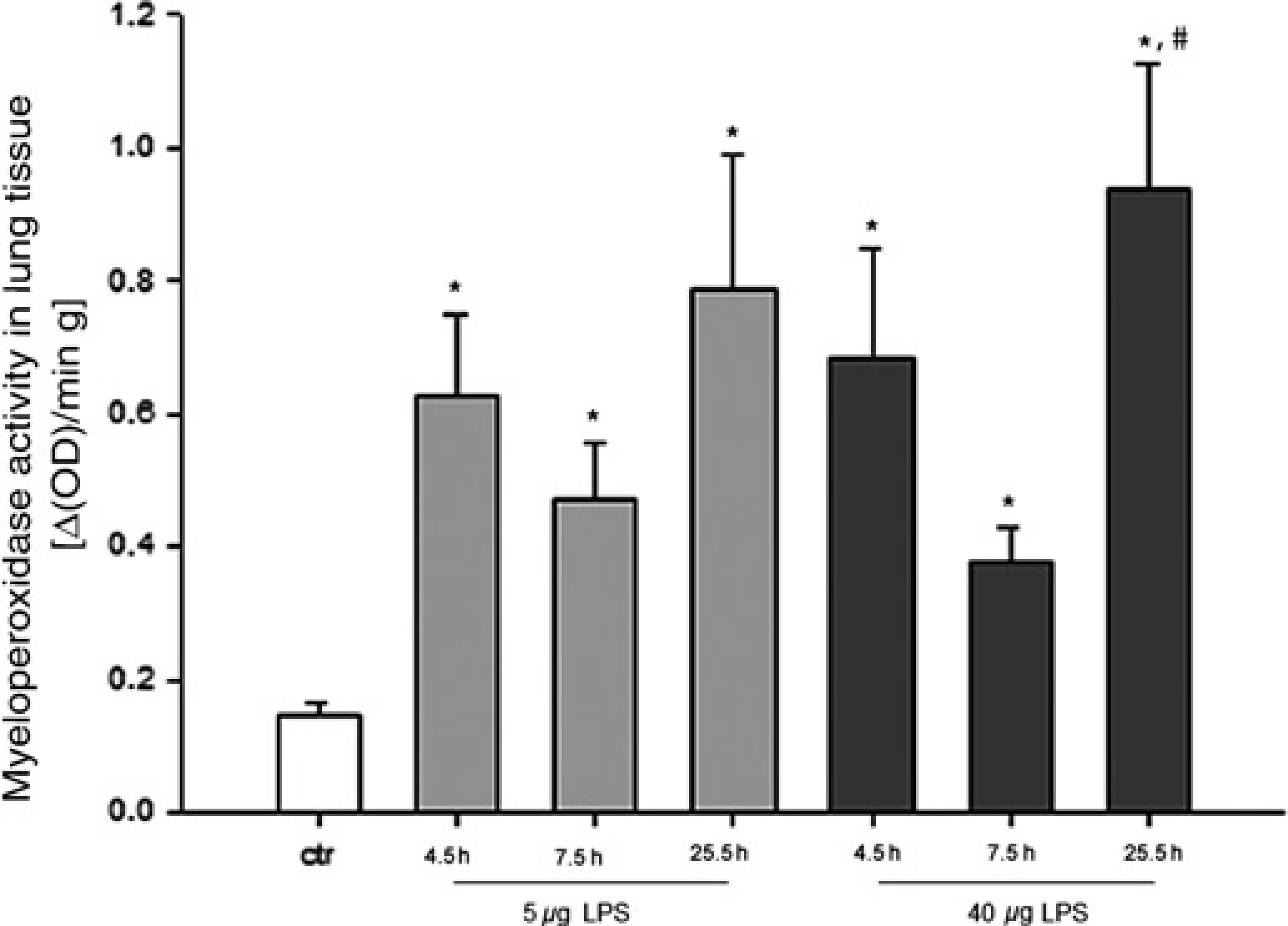
Lung myeloperoxidase activity, an index of neutrophil infiltration, was elevated following
Discussion
The major findings of our study are: (1) LPS intratracheal administration resulted in increased DTPA clearance in all studied groups. The time course of the increase in DTPA clearance was different between the two doses: in the lowest dose a U-shape response was observed, while for the larger dose higher clearance was noticed at the earliest time point (3 h) after which clearance decreased with time. Dependency of DTPA clearance on the different doses of LPS was only observed at three hours after LPS but not later. (2) Total protein in the BAL fluid was only elevated at the earliest time point in both doses but not afterwards. (3) Tissue elasticity was increased at 7.5 and 25.5 h of LPS administration, but not at the earliest time point (4.5 h). (4) The histological lung injury score was increased in all treated groups with the higher score observed at the larger dose and latest time point, mainly due to the increase of the intra-alveolar neutrorphil infiltration. (5) MPO activity was increased in all treated groups. Thus, our study shows that there is a differential time- and dose-dependency of the various indices of lung injury after intra-tracheal LPS instillation in rats.
Lung permeability (99mTc-DTPA clearance and BALf protein)
Lung clearance rate of the 99mTc-DTPA was significantly increased in all LPS-challenged groups, suggesting an increase in the alveolar-capillary permeability following LPS intratracheal instillation. Regarding the time effect after LPS exposure, 99mTc-DTPA clearance presented a U-shape time course at the lower LPS dose. In contrast, LPS had a linearly decreasing effect on 99mTc-DTPA clearance over time at the larger dose. Dose-dependency of the 99mTc-DTPA clearance was only observed early (only after 3 h after LPS exposure).
The pulmonary clearance rate of 99mTc-DTPA is a noninvasive technique for assessing lung permeability. The technique is based on the fact that 99mTc-DTPA is a small-molecule hydrophilic solute that once deposited in the lungs will passively diffuse through the epithelial and endothelial cell barrier.3, 40-43 The clearance of 99mTc-DTPA is primarily determined by the integrity of the epithelial element of the alveolar-capillary membrane barrier, 3 and is influenced to a lesser extent by other factors including lung volume, tracer deposition site (alveolar or bronchial), volume of the liquid layer of bronchial and alveolar surface, the presence and functional integrity of surfactant,44,45 and lymphatic and pulmonary blood flow.4,46
At 4.5 h after LPS, vascular leakage was also observed as indicated by the increased protein index of BAL fluid, which is in agreement with previous data. 29 This correlates well with the results from 99mTc-DTPA scintigraphy, where increased 99mTc-DTPA clearance was found three hours after LPS administration. Intratracheal administration of LPS in rats has been previously associated with increased permeability of the alveolar-capillary membrane in doses similar to ours28,29
Although protein concentrations were restored to control values after 7.5 and 25.5 h of LPS administration (that is in accordance with prior studies 47 ), 99mTc-DTPA clearance remained accelerated. Even though this discrepancy cannot be fully explained from this study, some speculations can be made. Firstly, 99mTc-DTPA is a small solute and its clearance is expected to be more sensitive marker of increased alveolar-capillary permeability than the much larger proteins. Indeed, moderate lung injury in sheep produced more pronounced clearance of 99mTc-DTPA from the lungs, compared with intratracheally instilled radiolabeled protein tracers. 16 Secondly, intratracheally instilled LPS could produce a more severe and prolonged effect in the epithelial barrier rather than the pulmonary endothelium. This could explain the accelerated 99mTc-DTPA clearance 6 and 24 h after LPS, which although a marker of overall alveolar-capillary permeability, is primarily influenced by the integrity of the pulmonary epithelial barrier. 3 In contrast, protein concentrations in BAL fluid are also dependent on vascular leakage. Pulmonary ARDS is considered to damage the alveolar epithelium more than the endo-thelium. 48 Accordingly, in LPS-induced lung injury in mice after intratracheal administration, electron microscopy revealed an extensive injury of alveolar epithelium, but an intact endothelium. 49
At 6 and 24 h post LPS dose-dependency was not observed. A potential mechanism which could contribute to the lack of 99mTc-DTPA clearance differences between the 5 and 40 μgs of LPS at six hours is as follows. Decreased alveolar fluid clearance has been noted in rats, at six but not at three hours following intratracheal administration of a high dose LPS (100 μg/kg). 50 Although the effect of lung water accumulation and alveolar clearance mechanisms on 99mTc-DTPA clearance is not known, decreased liquid clearance could increase the volume of the epithelial and alveolar liquid layer and consequently decrease the concentration of 99mTc-DTPA in alveolar fluid and/or enhance the tissue–fluid barrier (i.e. its resistance to diffusion into the pulmonary capillaries), thus decreasing its passive flux. 11 In support of this notion, induction of airway wall edema (through infusion of bradykinin) was associated with a decrease in 99mTc-DTPA clearance. 51 In contrast, lung permeability to instilled mannitol (a small solute) was mildly increased when alveolar fluid clearance was increased by over-expression of the Na,K-ATPase b1 subunit in rat lungs.51,52
However, the above cannot be the case for the lack of 99mTc-DTPA clearance differences at the 24 h time point, since alveolar fluid clearance is known to increase after 24 h of intratracheal LPS administration in rats.47,50 Interestingly, an increase of the alveolar membrance thickness was found by histology at 25.5 h of LPS at the larger dose (compared with the lower). Thus, it stands to speculate that thickening of the barrier could partly explain the lack of dose dependence at the 25.5 h time point.
Another factor that could influence the results is the effect of the distribution of the LPS-induced lung injury on 99mTc-DTPA delivery and deposition in the lung. Lung injury is known to cause diffuse alveolar flooding and micro-atelectasis at the most injured lung sites 1 and this could prevent 99mTc-DTPA delivery to the most injured lung regions. However, no difference was observed in the initial distribution in the lungs of the radiotracer in our experiment. Moreover, the absence of gross differences in the lung injury score between the different LPS-treated groups in our study suggests that differential initial distribution of the radiotracer in the lung was not the cause of significant differences in 99mTc-DTPA clearance measurements.
Lung histology and MPO activity
Lung histology revealed the presence of lung injury in all LPS treated groups. An increased lung injury score was observed for the larger dose at 25.5 h compared with the lower dose and to other time points of the same dose. This was mainly due to the increased intra-alveolar neutro-phil infiltration. These findings are in accordance with prior studies showing increased neutrophil infiltration at 24 h post LPS exposure in rodents, compared with earlier time points. 53 MPO activity, a marker of overall (both intra-alveolar and interstitial) lung infiltration of neutro-phils, was increased at both doses and all time points, revealing that LPS treatment in our experiment resulted in neutrophil influx in all treated groups. Taking in account that MPO activity was underestimated in our experiment (due to performing BAL that reduces the number of intra-alveolar neutrophils), it stands to conclude that both doses of LPS have led to even greater increase in neutrophil lung infiltration than actually reported. Since MPO activity was similar between different doses at three hours post-LPS, dose dependency at that time point in DTPA clearance cannot be attributed to different neutrophil infiltration. Moreover, the increase in intra-alveolar neutrophil infiltration at 25.5 h of the larger dose was not associated with an increase in DTPA clearance. Thus, our results suggest that post-LPS exposure, the mechanism of DTPA clearance acceleration is independent or at least only partially mediated from intra-alveolar neutrophil infiltration. In support of our findings, it was previously shown in rats that at four and eight hours post-LPS, increased permeability was independent from neutrophil recruitment. 29 LPS could increase lung permeability by directly affecting the lung epithelium54,55 and/or through activation of alveolar macrophages. 56
Regarding the other parameters of lung injury, it is worth noting that pulmonary edema was noticed at the 4.5 and 7.5 h time points. This correlated well with the observation that faster DTPA clearance rates and protein influx were documented at the early time points (3 and 6 h, respectively for the two doses of LPS), since increased alveolar-capillary membrane permeability is expected to be associated with increased alveolar fluid accumulation and pulmonary edema.
Respiratory system mechanics
In our experiment, changes in the mechanical parameters of the respiratory system, consistent with the presence of lung injury, i.e. decrease of respiratory system compliance 57 and/ or increase of tissue elasticity (H parameter of the constant phase model),38,58,59 were noticed after 7.5 and 25.5 h of LPS at both doses, but not after 4.5 h. Thus, deterioration of lung mechanics was delayed compared with the increase in lung permeability assessed by 99mTc-DTPA scintigraphy and lung BAL fluid protein. This suggests that the increase of lung permeability precedes the changes in mechanical lung function assessed by lung mechanics measurements. This is reasonable since lung mechanical changes reflect the cumulative effects of increased permeability and cellularity over time and tissue elasticity can only be increased after increased permeability and cell infiltration have affected mechanical lung function.
The time course of derangement of mechanical lung function after LPS administration is controversial. Our results are in accordance with previous studies showing increased tissue elastance 24 h after intratracheal LPS instillation both in rats 60 and mice, 61– 63 but not at earlier time points (i.e. 4 hours after LPS). 64 Nevertheless, it should be acknowledged that LPS has been found to deteriorate mechanical lung function early after LPS administration (e.g. 2 65 or 4 h 66 following intratracheal LPS instillation). These conflicting results can possibly be explained by the larger doses used in the aforementioned studies (15 and 1 mg/kg of LPS, respectively, 65,66 compared with ~20 and 160 μg/kg in our study). Even at 24 h after LPS administration, altered lung tissue mechanics have not been always documented.14,37 This can probably be attributed to the different experimental settings, such as the different route of LPS administration (nasal instillation 37 ).
An interesting finding of our study was the decrease of hysteresivity after 25.5 h of LPS. Changes in hysteresivity are attributed to tissue rheological properties (e.g. changes in parenchymal connective tissue) 67 and/or to appearance of regional heterogeneities in the lung. 68 In the literature, lung injury has been associated with increased, 69 decreased 38 and/or unchanged hysteresivity. 37 The physiological and/or anatomical interpretation of hysteresivity is not clearly established, and the design of our study does not allow us to clarify the mechanism of decreased hysteresivity after 25.5 h of LPS.
Implications
The induction of lung injury from LPS isolated from P. aeruginosa in experimental settings is clinically relevant, since this microbe is one of the most common causes of severe pneumonia in hospitalized patients, especially those under mechanical ventilation in intensive care units and those who are immunocompromised. LPS is one of the major molecules of the Gram negative bacterial outer membrane that mediate immune responses to bacterial infections, together with other components of bacteria, such as exotoxins. 70
To our knowledge, this is the first study examining in detail the time course and dose-dependency of various indices of lung injury after LPS exposure such as DTPA clearance, BAL fluid protein, lung mechanics (assessed by the force oscillation technique and static PV curves) and histology in spontaneously breathing animals. In the literature different doses of LPS and time points of assessment are used, creating varying and sometimes conflicting pheno-types of LPS-induced lung injury regarding the inflammatory and/or physiological effects of LPS on the respiratory system (lung permeability and mechanics). Our study was designed with the aim of reconciling these conflicting results and putting them into better perspective. Moreover, the detailed description of the time course and the dose-dependency of alterations of the various indices of lung injury in the LPS model would enable the design of future experiments testing specific pathophy-siological aspects of the LPS-induced lung injury at appropriate time points. For example, a therapeutical intervention targeting epithelial permeability should be studied early after LPS administration, in contrast to lung mechanical parameters that should be measured at later time points.
Measuring lung permeability by the non-invasive DTPA scintrigraphy technique, as in our experiment, is important, since most of the other techniques of assessing alveolar epithelial permeability are invasive and are performed post mortem. 3 In vivo, non-invasive imaging in animal studies has proven to be a useful tool in biomedical research, enabling longitudinal studies on the progress of a disease and/or studies with therapeutical interventions, using animals as their own control. Thus, this technique enables monitoring of lung permeability (in contrast to other invasive methods) in studies focusing both on the acute states of lung injury and on lung injury resolution and repair.
Our study has shown for the first time the effect of different doses of LPS in the pulmonary clearance of 99mTc-DTPA. The time-dependent effect of LPS in the pulmonary clearance of 99mTc-DTPA has been previously studied by Brown and co-workers, 14 yet with several important differences from our study. These investigators studied a different animal species (rabbit) with much shorter time frame (4-8 h). Interestingly, in contrast to our study, Brown et al. could not detect any change in either histologic indices of inflammation or lung mechanical parameters at any time point after LPS exposure, suggesting that in their model the lung injury was mild at best. More importantly, in our study we used spontaneously breathing animals, while in the study of Brown and co-workers the animals were mechanically ventilated under positive end-expiratory pressure, which by increasing lung volume may increase lung clearance rates71-75 and thus the results obtained. Furthermore, in the study of Brown and co-workers, 99mTc-DTPA clearance rates were determined using a gamma counter probe. In contrast, in our study 99mTc-DTPA imaging was performed using a high-resolution dedicated small-animal camera with 2 mm spatial resolution. This is very important for the accuracy of the results obtained. Indeed, most of the 99mTc-DTPA clearance animal studies performed in the past were using clinical cameras or counting probes. Clinical gamma cameras (designed for use in humans) have spatial resolution of 1-2 cm which is far from appropriate for the small rodent lung. Even worse, counting probes just measure incident gamma rays. The advantage of our imaging system becomes apparent in the ROI selection considering the size of a rat's lung. Our imaging system could be used in the future to study regional heterogeneity of injury in the various models of lung injury in rodents. In general, the use of techniques adapted to the size of small rodents allows for better insight into the mechanisms of disease, as has been proven for other indices of lung injury (e.g. obtaining lung mechanics by the use of small animal ventilators 76 ).
In conclusion, the major finding of our study is that there is differential time- and dose-dependency of the various indices of lung injury after LPS intratracheal instillation. Thus, the comparison of results of studies using different doses of LPS and time points of assessment should be made with caution, since variations in either! the LPS dose or in the time of assessment after LPS exposure can lead to significant differences in the results and thus the conclusions drawn.
Footnotes
Acknowledgements
The authors thank Paris Maurokefalos, Penelope Bouziotis, Maria Papachristou and Zoi Kollia for their technical assistance with the radiotracers and animal handling. The authors have no conflict of interest to declare. This work was supported by the GlaxoSmithKline Greek Research Scholarship Program in Respiratory Medicine under the auspices of the Hellenic Thoracic Society and the Thorax Foundation, Athens, Greece. Part of the cost of the animals was a generous gift of ELPEN pharmaceutical company, Pikermi, Attiki, Greece.