
Abstract
The purpose of this research was to consider why absenteeism in Health and Social Care is so high and to suggest proactive changes in organization activity to address this. The research took a multimethod approach with a quantitative emphasis; there were three parts: (i) quantitative survey questionnaire; (ii) analysis of absenteeism and related secondary data; and (iii) qualitative data from other questions in survey and discussion groups. The quantitative emphasis in the research is appropriate, given the gap identified in the literature. Perceived limitations are that the study considers just one part of the overall system. The research indicates that managers underestimate staff absence levels and almost half believe absenteeism cannot reduce. Professional managers were more negative and over half of nurse managers believed that absence could not reduce. Unless there is a systematic systemic change in organizations, which changes managers' attitudes and understanding of absence with a consequent change in activity across the absence continuum, there is no prospect of a sustained reduction in absence levels. Manager impact and role in absence management are poorly covered in research, so this research helps inform those gaps.
Introduction
There is voluminous literature on absence with practitioners focusing on prescriptive quick-fix solutions and academics focusing at individual level. 1–4 Neither pays much attention to managerial control strategies or avoidance of absence. 5 Managerial jobs and behaviour are relatively unexplored. 6 Much of it is methodologically unsound 7,8 and cannot be considered best practice.
This research was conducted in two ‘legacy’ Trusts of a health and social care (HSC) Trust in Northern Ireland (NI). This paper begins by addressing some of the gaps in the absence literature and considers why absenteeism is so high in HSC in NI. The research method which incorporates surveys, discussion and some secondary data with a quantitative emphasis is then explained. Specific research questions focused on: what are managers' roles, attitudes and approaches to absence of their staff? Are there patterns in attitudes and actions of managers who share the same characteristics? What are the roles, attitude and approaches of Occupational Health Service (OHS) when dealing with absent staff? How do managers and OHS compare with and view each other? Where and how could improvements be made? The findings and discussion assist the understanding of absence management and points the way to improvements through change management. A key area of interest for the authors was providing an insight into changing current practice by assessing the contribution of managers and OHS to absence management, and to recommend areas for further research.
Literature
Analysis of literature
Although the literature around workforce absence is voluminous it has significant gaps. These include the management of absence generally and interlinkages between key stakeholders, with little attention being paid to wider issues, such as the linkage between managerial jobs, behaviour, organizational context 6,9 and inter-relationships between line management, HR and OHS. 10,11 Relatively little attention is paid to cultural aspects of absenteeism, a powerful indicator of absence behaviour. 1,3,12 Some types of absence are researched more than others and effectiveness of ‘solutions’ is poorly covered. 5,7 Reports about rehabilitation initiatives are scarce and are concentrated in practitioner journals, 13–16 and 80% percent of people still absent after six months have not returned to work in 12 months. 17
Practitioners mainly adopt an advocacy approach, unsupported by evaluative evidence and with no sound basis for learning or replication, or support for currently recommended best practice. 5,7 Less than one per cent of published articles in most journals reach minimum standards of scientific soundness 8 and authors focus mainly on individual level outcomes based on absence as a decisional choice. 2,3 Much of the literature focuses on controlling short-term absence, 18 with neither practitioners nor academics paying much attention to avoiding and managing absence stemming from genuine illness. 5
Costs of absence
A significant body of opinion believes that up to 20% of absence is not genuine 3,8,12,19–24 and identifies failure to support rehabilitative early returns to work. Few authors offer an opposing view. 25
The literature identifies significant costs arising from absence: sickness absence costs the economy £12bn per year 17 absenteeism is significantly higher for public than private for sector workers 26 and higher again in NI; 27 the public sector accounts for 29% of total UK employment but 36% of total absence 28 ; 70% of £76 billion NHS funding is directed at staffing 29 and one per cent of absence, based on five per cent levels, costs a minimum of £32.4 million per annum. NI HSC staffing costs are over £1.5 billion 31 and absence levels in NI in the HSC sector are generally higher than GB, 31–34 though care has to be taken with comparisons, as reporting mechanisms are different. 35 Less than half of organizations cost absence 24 and they simply throw money at the problem. 36 Managers are more concerned about their reputation and credibility than about the financial impact of absence. 9
Government interventions
The literature gives many examples of Government interventions over the years 29,34,37–40 but effort is fragmented and at times there is a loss of momentum. Organizations address absence when it is a problem and when it reduces, it is shifted down the priority list; 20 with only one-third of organizations including absence management as an element in line managers' appraisal/performance targets. 24 Awareness levels about government directives are low 41 and targets are not always translated into action. 38 Furthermore there is no evidence that reductions are sustained and absence levels are characterized by ‘yoyo-ing’ from year to year. 24
Absence control
Solutions are offered though, mainly in the practitioner press and there is concern that the sustainability of reductions and financial incentives for attendance could signal that managers have abdicated responsibility for managing absence. 9 The discretionary behaviour of employees is conditioned by how managers, particularly those with frontline contact, behave and there is a strong relationship between cohesion in teams and quality of care and fewer problems with absence. 42 There is evidence that the Knowledge and Skills Framework, with its built-in annual appraisal, actually reduces absenteeism 29 and appreciative inquiry led to a significant fall in absence, possibly through a sense of individual scrutiny. 43 Failure to account for normative effects may explain the inconsistent success of reward-based absence-control programmes 1 and the ‘Hawthorne Experiments’ highlighted that improvements occurred if staff felt they belonged and were recognized. 45
NHS dimension
The NHS has the highest absenteeism levels across all sectors 24 and a one per cent reduction could release £34.2 million per annum. Few authors attempt to explain high levels of NHS absence and reasons given are not unique to the NHS. Health staff do face particular work-related risk factors with musculo-skeletal disorders accounting for three-quarters of nurse work-related illness 37 and 40% of all sickness absence in the NHS relates to manual handling accidents. 15 Overall the most common health problems causing absence overall are upper back pain, depression and anxiety. 46 There is a strong link between poor ergonomics awareness and an increase in chronic backache 21 and a cultural shift is needed to put responsibility for personal health back with the employee. 46
Change
Improvement requires change but this will be difficult though not impossible. Ideas differ about how to implement change but there is significant agreement that many change initiatives fail. 45,48 Neither performance targets, modernization, nor massive increases in funding have delivered the transformation the government wanted to see in the NHS. 49 Professional allegiances and cultural differences are recognized as major blocks to change 26,43–44,50–52 and a perception that changes were financially driven led sympathetic stakeholders to distrust the process, 53 but many organizations trust financial incentives as the solution to every problem, including problems caused by financial incentives in the first place. 54
Methodology
At the time of study, the HSC system in NI was undergoing immense structural and service change, most notably in reductions in the number of provider and commissioning organizations and reductions in the level of financial resources available through government funding. Eighteen Health and Social Services (HSS) Trusts were being reduced to five HSC Trusts 55 with the purpose of reducing bureaucracy in order to achieve cost savings. The two Trusts in this study were included in six Trusts contracting into one. Reducing managerial overheads 56 was a specific goal. This meant that many of the target group for this survey were directly affected by the changes, with many at risk of losing their jobs. Care was taken to distance the researchers from the participants to minimize concerns that responses could be fed into the management of the changes and selection of managers for redundancy. The return rate compares well with other managerial studies.
The research emphasis was quantitative and survey questionnaires were the primary means of obtaining information on which to base conclusions (full ethics committee approval was granted). The research covered two ‘legacy’ Trusts, HSST1 and HSST2, that merged with others into the newly formed HSCT1. One of the authors was earlier employed as HR Director in one of those Trusts. The study concentrated on managers, OHS and their roles, relationships and perceptions of absence. The research questions were: what are managers' roles, attitudes and approaches to absence of their staff? Are there patterns in attitudes and actions of managers who share the same characteristics? What are the roles, attitude and approaches of OHS when dealing with absent staff? How do managers and OHS compare with and view each other? Where and how could improvements be made?
There were three parts to data collection: (i) quantitative survey questionnaires; (ii) analysis of absenteeism and related secondary data; and (iii) qualitative data from ‘other’ questions in survey and discussion groups. Bias, confidentiality and potential problems were considered and efforts made to reduce impact. The research community supports the quantitative approach 57 and it fits with NHS culture. 53,58
Questionnaires were structured to elicit information about respondents' views of OHS, management, their inter-relationships, roles and sickness absence. They were piloted prior to issue. The mode of administration was self-completion. Reminders were used to improve response rates and responses were entered into an Access database. Question ordering placed general questions before specific questions. 59 ‘Other’ response sections were used to give insight into responses generally and provide qualitative information, which would assist follow-up discussions thus supplementing the quantitative approach. The first section of the questionnaire covered respondents' managerial backgrounds, gender, age and working contexts so that patterns linked to different characteristics could be considered. Questions were asked about absence levels, their reduction and the existence of an ‘absence culture’. Respondents who indicated interest in follow-up were personally contacted and asked if they wanted individual or group feedback. All opted for group feedback though it was concerning to note that many were worried about their area ‘looking bad’. This may indicate a ‘blame culture’. Discussion groups were used to test understanding of concepts and questions, including the concept of absence. Respondents confirmed that their meaning of absence included short and long-term absences, ensuring construct validity. 60 Using qualitative data from discussion, complemented strengths, reduced weaknesses and enhanced robustness. 61 There were similarities in the qualitative data to findings from the quantitative data, which reinforced inferences and helped solidify conclusions. Secondary data were obtained from the DHSSPS about absence levels in HSST1 and HSST2 and about managerial oversight of moving and handling in HSST1.
The research targeted the full complement of managers in HSST1 and HSST2 (189 and 105 respectively, 294 total) and there was a 27% return rate giving sufficient sample size for inferences to be made about the general manager population. Introductory letters were used to explain the purpose of the questionnaire and to give assurances about confidentiality. 62 Groups were smaller in some of the subanalysis and care has to be taken in generalizing these results; the biggest of the subgroups was nurse managers, which numbered 25, the smallest was HR managers at five individuals. AHP and support managers fell between the two. The OHS response rate was 45% (40 OHS staff were targeted) with responses received from medical, nursing and physiotherapy professionals.
Respondents' ages were generally representative of the target population though slightly below for males in the target population. Findings for professional groupings, women and managers aged 41–50 are most representative. A partial triangulation 63 of results was possible, which increases confidence in the results. 40
Findings
The findings support the view that managers are more aligned to their teams than to their organization; 43,52 this alignment occurs despite high actual absenteeism detailed in Tables 1 and 2.
Absence levels in HSST1
(1) Highest average percentage regionally for professional and technical staff; and (2) lowest average percentage regionally for ancillary and general staff
Absence levels in HSST2
(1) Highest percentage regionally for days lost for nursing; and (2) highest percentage regionally for ancillary and general staff
There was an overall rise in absenteeism from September 2005 to March 2007, with fluctuations across different groupings. Levels are consistently high for ancillary and general nursing and social care staff. Reductions in the reporting period after particularly high levels, may indicate management action. Managerial attention and absenteeism fluctuate. 20,24
The research indicates that managers underestimate levels of sickness despite receiving regular absence reports, with 75.4% indicating this as average or below average despite it being above average. This reflects staff views. 1,3,64,65
Overall 76.7% of managers indicated a responsibility to manage absence with a worrying 53.4% overall indicating they were inactive. Greater differences appeared in professional groupings with AHPs (77.8%), nursing (60%) and social care (53.3%) having a majority reporting no activity. In discussion, managers felt this was because action was not needed. Return-to-work interviews were the most commonly identified direct staff absence responsibility (95.9%) echoing the literature. Return-to-work interviews, the most effective intervention, are used by 85% of organizations. 24 Other responsibilities are highlighted in Table 3.
Manager absence responsibilities
Surprisingly 23.3% of respondents did not report a responsibility for disciplining staff for poor attendance, reflecting the literature. Public sector organizations are unlikely to use discipline. 66 Managers are reluctant to discipline. 9,67
Just over half (57.5%) of managerial respondents replied that absence could reduce contrasting strongly with OHS respondents (88.9%) (see Table 4).
Managers and OHS views
There are differentials between professional groupings with nursing showing as the only grouping with a majority believing absence cannot be lowered. Fifty-six per cent of nurse managers said ‘no’ and 44% said ‘yes’. The figures for AHPs and Social Care managers were the same with 33.3% saying ‘no’ and 66.6% saying ‘yes’. Disturbingly, of the five HR respondents, three indicated a belief that absence levels cannot reduce, mirroring nurse managers. Managers became more negative about reducing absence levels, as they got older. In discussion, this was considered to result from managers ‘being worn down’ by previous experiences. Support managers were stronger about abuse occurring than professional managers, with one professional commenting: ‘we are supposed to be caring’. Other comments were that staff were loath to take sick leave and that staff pushed themselves too hard so managers ‘could not get staff to take sick leave’. The literature 1–4,12,24,26 indicates that absence levels can be reduced. Support managers were strongest in saying there was a culture promoting absence, whilst AHPs were strongest in saying there were reasons other than sickness and social care in saying that staff extended breaks.
Almost 90% of OHS respondents believed absence could reduce and were more likely to highlight culture (68.8% compared with 34.2% of managers). OHS views align with the evidence. 1,4,12,68,69 Other research indicates that more than 90% of public sector respondents believe absence could reduce. 24 OHS strongly supported rehabilitative returns to work. The literature 15,18,70,71 indicates this is an important role for OHS but the management of long-term absentees returning to work is little explored. 18 There was an overwhelming response from ‘no’ respondents that absence related to illness. Respondents were asked about activity (see Table 5).
Manager action to prevent absences
*Respondents ticked more that one action
It is noticeable that the most common response deals with offering help and that tougher action, such as challenging individuals, appears lower down the list. This links to literature about managers avoiding challenges and only giving positive messages. 53,67 Activity was then linked to time (see Table 6).
Responsibility and time actually taken
*Dealing with absence
The identification of a responsibility for disciplining staff for poor attendance shows 23.3% of respondents as not having any responsibility, while activity indicates 53.4% not spending any time on discipline: a jump of 30.1%. Professionals are less likely to discipline staff for poor attendance than support services managers, possibly due to a shared professional ethos. 9 Discipline is an important control. 15,24,29 In total, 94.5% identified a responsibility to refer staff to OHS but 20.6% indicated no activity: a jump of 15.1%. If conducting return-to-work interviews and counselling staff for poor attendance are taken as proxies for dealing with absence, 23.3% indicate no activity while 95.9% and 90.4% indicate such a responsibility: a jump ranging between 19.2% and 13.7%. These raw differences are significant and the inference that managers are not taking action across the continuum, even when they are aware they have a responsibility, is concerning. The ‘no’ group reported higher levels of inactivity but inactivity was not exclusive to this group. Differences also appear for professional groups, age and gender: with professional managers, older and female managers showing most negativity. Follow-up discussion cast no light on this inactivity. Results support research indicating manager avoidance but there are no direct comparisons for the detail.
Policies are considered a cornerstone of absence management 7,15,24,29 and an overwhelming 90.4% of manager respondents in this survey indicated they referred to a managing absence policy. A majority of OHS respondents used the managing absence policy. Over half (60.3%) of manager respondents indicated that they set a specific goal in their own objectives with 39.7% indicating they did not. Objectives are important in managing absence. 3,7,15,24 Respondents were asked if they set a specific goal for managing absence and there are differences across the four largest managerial groups of respondents. A majority indicated they did so with AHPs (89%) and Support Services (70%) most likely to do so (see Figure 1).
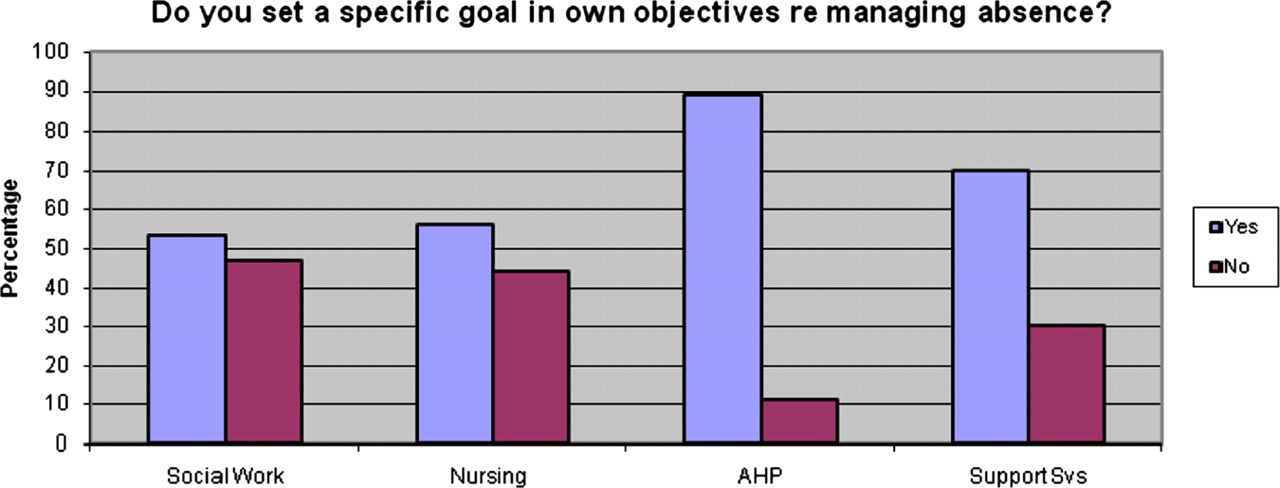
Practice in setting objectives by managerial group
Men (66.7%) were more likely to set objectives than women (58.2%) and there were age differences, with those over 51 (72.7%) most likely to set objectives. Yet managers over 51 were more negative and inactive.
There was an interesting differential between raising the importance of attendance with staff groups or individually (see Table 7).
Discussing attendance by group
Nurse and AHP managers were most likely to raise the importance of attendance with groups of staff but reported the greatest drop in dealing with staff as individuals. Social care and support services reported lower levels of activity. The low base of activity in raising the issue for social care (66.7%), support services (60%) and managers under 40 (58.3%) is concerning. Greater differences occurred when age and gender were taken into account (see Table 8).
Discussing attendance by age/gender
Professionals, managers over 51 and women are less likely to deal with staff individually. OHS report higher levels of individual communication with 13 out of 18 indicating they would say if absence levels are unusually high. Evidence indicates that managers avoid the more difficult parts of their roles. 38,67,72
Table 9 provides a summary of the findings in direct relation to the research questions.
Key points from surveys – research questions
OHS, Occupational Health Service
Discussion
This research provides a disturbing insight into absence management, the single biggest cause of lost productivity. 9 Academics focus on individual absence and practitioners focus on solutions, with policies, objective setting, return-to-work interviews and flexible working all highlighted 24 yet the public sector, which has the highest levels of absence, uses these. Is practitioner literature correct? Are these approaches ineffective or is it the way managers apply them?
Manager respondents underestimated absence levels despite receiving reports about staff absence, echoing the literature, 1,3,9,64 and almost half believe absenteeism cannot reduce. Professional managers are more negative with nursing having a majority reporting that absence cannot reduce. In striking contrast a majority of OHS respondents perceived absence levels to be average or above and 88.9% believed they could reduce. There is no OHS comparison in the literature for this finding. Unlike managerial attitudes OHS' views fit well with 90% of public sector respondents believing absence could reduce. 24 Such a disparity in views in the face of evidence may be a cultural issue and indicates significant inaccuracies in manager criticism of OHS, and may indicate managers avoiding taking responsibility. The differences in professional manager attitudes highlight a need to find out about their attitudes and activity.
Discussion with support managers about ‘reasons changing but levels remaining constant’, points to staff having an ‘acceptable absence level’ culture. There is solid research evidence that highly cohesive groups are especially effective in developing and enforcing norms. 69 Care professionals did not highlight culture as significant in responses. Nursing is reported as having high levels of absence. 1,4,73 If nursing culture gives ‘permission’ for absence it would explain why nurse absenteeism is high and why the HSC has such a high level of absence. Allegiance to a profession may weaken professional management and reduce contribution to achievement of organizational goals, including managing absence. Change is needed to ensure that managers accept that reductions are possible.
A majority of respondents reported managing absence responsibilities, using the absence policy and setting objectives. If objectives were achieved, absence levels should go down, 10,27,74 but absence data shows otherwise. 31–34 This research indicates managers set absence objectives even when they do not believe in an outcome. Setting objectives and referring to the policy may be activity to ‘be seen to be’ acting. Almost 96% of managers reported conducting return-to-work interviews but attitudes uncovered in this research must undermine their effectiveness. The added value of this activity in HSC has to be questioned where almost half (42.5%) of managers believe absence cannot reduce. Employers do not follow their policies. 20 Understanding managers, their beliefs and how this translates into practice is critical in developing sustainable approaches to the management of absence.
Long-term sickness was raised in discussion and in the responses, yet little evidence was presented to indicate managers pro-actively sought to reduce time off, rather, the attitude was ‘nothing can be done about this’. Unsurprisingly OHS was stronger on rehabilitative returns to work. The literature gives strong support for OHS intervention in rehabilitative returns to work. 1,4,12,17,24,68–71 In discussions, managers were hesitant about rehabilitative returns to work. This included fears that abusers would take more time off, cost implications and a need for support systems. There may be links between underestimating staff absence levels, believing absence cannot reduce and consequent managerial activity, all of which may be further controlled by sub-cultures within the service.
OHS contribution may be underestimated 70 and this research shows low levels of manager usage. Managers had least awareness of the OHS preventative role. Manager criticism of OHS reflects the little available literature 70 and may be a defence of managerial inaction. Is OHS being used as a scapegoat for managerial failure to reduce absence levels? Managers using OHS as an alternative to action are criticized. 36 This research suggests OHS could be less criticized and better utilized.
Failure to manage absence may indicate wider managerial failings, as a fundamental failure in one area may mean similar failures in other areas. There are nursing staff shortages, 73 yet getting staff into work does not appear to be addressed rigorously. Costs are significant and a reduction of one per cent in absence levels could release in excess of £34 million to the NHS per annum. Change is needed but a critical mass 75 and commitment may be lacking. 76 The NHS is a monopoly and for many staff, particularly care professionals, this is their only experience of work. If experience is narrow then managers who rely on direct experience to plan change 48 may not see a problem with absenteeism, as this is what they have always known. Professional attitudes/territorialism causes difficulties 9,15,44,46,49,50,77 and indicators were rarely used to stimulate improvement. 78 The Department still relies heavily on the Circular newsletter as a means of effecting change but this does not fit with increasing complexity and sheer volume of information. 41 Changes directed at specific elements of absence may not work as one-dimensional change interventions are likely to generate short-term results and heighten instability. 57 This research indicates a need for systemic change on all dimensions because of the complexity in managing attendance. Improved understanding of absence is not the end of the journey. Overtime and labour turnover, like absence, affect productivity and further research is needed into managerial counter-productive behaviours as failures in absence may be reflected elsewhere. Wider changes and a total systems approach 50 may improve management generally.
Conclusion
This research provides an insight into absence management in HSC through investigating the roles of managers and OHS. It finds misalignment of managers to organizational objectives for absenteeism reduction through managerial negativity and inactivity, particularly in care professionals combined with inaccurate criticism and poor utilization of OHS. It shows that OHS is more aligned to the wider public sector managerial group than HSC managers, with OHS voicing frustration at endless appointments with little consequent managerial action. Absence merits rigorous attention as it affects quality of care, wastes manager and OHS time and bleeds resources away from core services. It is a persistent festering sore that is the single biggest cause of lost productivity. This means that a systemic change programme is needed for fundamental improvement, otherwise the HSC will continue at the top of the league of high absenteeism.
The internal focus of the NHS may contribute to a culture where managers do not see absence reduction as practicable or core to their roles. This would be one explanation for the disparity between manager responses in this survey and the wider pool of public sector managers. 24 The research shows higher levels of negativity among professional managers, with nurse managers being most negative. Nursing culture may have a significant negative impact on absenteeism and its control. The influence of professional culture within and outside the organization should not be underestimated. There is solid research evidence that highly cohesive groups are especially effective in developing and enforcing norms. 69 Nursing cohesion may be working against the organization since nursing culture is alienated from it 1 and one consequence of this may be high absenteeism. Cultural aspects of NHS management merit further examination, particularly in relation to professional attitudes. This is needed in order to recognize the strength of the professions as separate groupings within HSC and the consequent development of subcultures, which in turn affect the meaning of absence, the subsequent level of absence and its control. One of the most challenging research tasks is the examination of organization culture across occupations. 74
The main contribution of this research is that it adds to the body of knowledge about the management of absence, which may be of value to those working in the HSC/NHS and the wider public sector. It identifies a number of significant gaps and considers an under researched area. The research recommends future investigation through the collection of a larger set of survey data and that any replication is supplemented by detailed case study material that enables fuller exploration of the dynamic interplay between managers, OHS and staff.