
Abstract
Th e purpose of this study is to examine how and when service quality and satisfaction simultaneously influence purchase intentions. The study tries to explore and clarify the relationship between service quality and satisfaction, and to examine whether satisfaction simultaneously moderates and mediates the relationship between perceived service quality and purchase intentions. A field survey was conducted for the outpatients of 12 regional hospitals in Taiwan. The findings show that the effects of different dimensions of service quality on purchase intentions are not equal across satisfied and unsatisfied patients. This study provides empirical evidence that show how the dual roles of the moderator and mediator manipulated together by satisfaction, work to affect purchase intentions in hospital settings. In addition, the relationships between service quality and satisfaction are also clarified.
Introduction
Purchase intention is an important index to assess effects of service quality. 1 Many studies have proved that service quality and satisfaction are both antecedents of purchase intentions, 2–4 but the relationships among the three constructs are multifaceted: direct effects, mediating effects or moderating effects. 1,5
How satisfaction affects the influence of service quality on purchase intentions is an interesting issue. Empirical evidence shows that service quality has positive and direct influence on both customer satisfaction and purchase intentions, whereas there is also much evidence that customer satisfaction mediates the relationship between service quality and purchase intentions. 4,6,7 As to the moderating effect, some studies 1,5,8 show the existence of the moderating effect is still uncertain. If satisfaction indeed moderates the influence of service quality on purchase intentions, it may play the moderator and mediator at the same time. Therefore, the effects of service quality and satisfaction on purchase intentions should be assessed simultaneously; the effects of service quality on purchase intentions may be not equal across satisfied and unsatisfied customers.
This study depicts how customers perceive their accepted quality, form their satisfaction levels and generate their purchase intentions in the context of Taiwan's competitive healthcare system. Health-care services exhibit a unique characteristic of power imbalance between service recipients (patients) and service providers (doctors): doctors have significant influence on patients' wellbeing, but patients have relatively limited ability to evaluate the functional value of such services. This imbalance affects the ability of the service recipients to evaluate the quality of health-care services they receive in such service encounters. 9 Based on the settings, the study tries to explore and clarify the relationship between service quality and satisfaction, and to examine whether satisfaction simultaneously moderates and mediates the relationship between perceived service quality and purchase intentions.
The framework of this study is first to review the literature that supports the development of the three constructs, followed by the theoretical support for hypotheses. Next, the survey instrument and data collection are described. Once the reliability and validity of the three constructs are documented, the processed hypotheses are examined. The paper ends with a discussion of the results and implications.
Literature review
The background of Taiwan's health care services
Since the 2008 presidential election in the USA renewed the debate about health insurance coverage, the health-care system in Taiwan has attracted worldwide attention because of its relatively low expenses and short waiting times. 10 In addition, Taiwan-style service making is invading China because of Taiwan's earlier efforts to internationally invest in education and development in the medical area. From a comparative standpoint, Taiwan's health-care quality ranks third in Asia and, therefore, its experiences provide China with a model to strengthen its medical resources and enhance quality. 11
Taiwan launched a National Health Insurance (NHI) programme in 1995, offering a comprehensive, unified, universal and low-payment health insurance programme to all citizens. The whole systems of health-care providers are divided into four levels by the number of beds and health-care proficiency: academic medical centres (the highest level: minimum 500 beds), regional hospital (the middle level: minimum 250 beds) and district hospital (the lowest level: minimum 20 beds), and physician clinics and dental clinics. Since Taiwan has a market-driven health-care delivery system with a mix of public, non-profit and private hospitals, competition between hospitals is quite fierce. 12 All academic medical centres and the majority of regional hospitals usually obtain patient preference. 12
On the other hand, the payment systems of the NHI programme are primarily based on the fee-for-service model, which means most health-care costs are covered by the NHI programme and the financial barrier of getting health-care service is very low. Unlike the managed care models in the USA or other Western countries, the absence of a referral system and the completely free choice of providers in Taiwan have provided great incentives for patients to go ‘doctor shopping’. 4 Moreover, most patients like to purchase health-care services from hospitals rather than from family doctors or clinics, even for minor illnesses. Given the facts, the competition among hospitals becomes very stiff after introducing the NHI programme. How to attract new patients as well as keep old ones, is important for hospital managers.
Service quality
Service quality is defined as how well the service meets or exceeds the customers' expectations on a consistent basis. 13 In health-care settings, many studies have suggested that patients' service quality perception is a key determinant of a health-care organization's success, due to its influence on achieving patients' satisfaction and favourable purchase intentions to hospitals. 4 Service quality is posited as a multidimensional construct, and the number and nature of the dimensions varied, depending on the service context. 14 Service Quality Gaps Model and the SERVQUAL scale proposed by Parasuraman et al. 13,15 are widely accepted tools for evaluating service quality. In health-care settings, the two tools are also frequently used to assess service quality in a number of service categories such as hospitals, independent dental offices, AIDS service agencies, services provided by physicians and nurses, and so on. 16
Satisfaction
Satisfaction reflects the degree to which a customer believes that a service provider evokes his positive feelings, 17 and many studies have suggested that service quality and satisfaction are distinct constructs. 4 A main view on this issue is that service quality represents a cognitive judgement, whereas satisfaction is an affective evaluation, which emerges as a response to a single or prolonged set of cognitive service encounters. 6,18 Therefore, a consumer is thought to make a cognitive appraisal of previous shopping experience, which leads to an affective evaluation reflected by satisfaction. 6
Distinguishing service quality from satisfaction suggests a causal order, that positions service quality as an antecedent to satisfaction. 17,18 Goldstein and Schweikhart 19 even argued that service quality is an indicator of satisfaction levels. There is also empirical evidence supporting this causal linkage shown in health-care settings. 20,21
The relationships among service quality, satisfaction and behavioural intention
The consumer decision-making for purchase is a complex and comprehensive process, and consumers not only evaluate received service quality but also respond to the satisfaction level felt by the accepted services. 6 Past studies have found that the influences of service quality and satisfaction on purchase intentions, take on different forms: direct effects, mediating effects or moderating effects. 1
As to the direct effects, both service quality and satisfaction themselves have positive influences on purchase intentions. 1–3,7,22 In health-care settings, much evidence also shows the direct relationship exists. 4,23
Between service quality and purchase intentions, customer satisfaction has been proven as a mediator.
1
A mediator represents ‘the generative mechanism through which the focal independent variable is able to influence the dependent variable of interest’.
24
Since service quality is a cognitive judgement, it will change as the shopping context changes. Relatively, customers' affective responses (i.e. satisfaction) to the most recent service encounter have greater influence on future loyalty intentions.
25
In this case, service providers must satisfy customers with every service encounter because previous cases of satisfaction get discounted in the event of a dissatisfying encounter.
5
Therefore, this study proposes the following hypothesis: H1: Satisfaction mediates the influence of perceived service quality on purchase intentions and service quality becomes a non-significant or less significant predictor of purchase intentions.
Unlike the mediating effect, the moderating effect of satisfaction between service quality and purchase intentions is still uncertain. Taylor and Baker 26 find that satisfaction moderates the relationship of perceived service quality and purchase intentions in three service sectors (communication, traffic service and entertainment) but not in the health-care service. In 1997, they tried to verify the moderator role of satisfaction again, in both for-profit and not-for-profit hospital settings. 27 Although the results support the growing view that satisfaction is more closely related to consumer behaviours than quality perceptions, there is still no significant moderating effect on the two types of hospital settings. Bou-Llusar et al.'s 1 findings show that satisfaction acts as a mediator on the relationships between quality perception and purchase intentions, but there is no significant moderating effect in the ceramic industry. Lin 8 discusses the existence of the moderating effect in the banking service industry, and the findings revealed that satisfaction moderated the relationship between service quality and purchase intentions.
The uncertain existence of the moderating effect is because of ignoring the non-linear relationship form. Regardless of the effect, forms of perceived service quality on purchase intentions are direct or indirect, such relationships among the three constructs are assumed to be linear. 26 There should be non-linear relationship between service quality and satisfaction because of the concept of ‘the zone of tolerance’. 7,26,28,29 Also, there should be non-linear relationship between satisfaction and purchase intentions based on the ‘concept of customer delight’. 30 Some studies found that satisfaction moderates the relationship between service quality and loyalty intentions. 1 Therefore, this study also considers the moderator played by satisfaction.
A moderator is the one which ‘systematically modifies either the form and/or strength of the relationship between a predictor and a criterion variable’.
31
For service providers, a moderating relationship means that the degree of satisfaction/dissatisfaction with the recent service encounter would change the perceived extent to which prior service quality remain a good predictor of customer intentions.
5
Mittal et al.
32
find that both overall satisfaction and re-purchase intentions are affected asymmetrically by quality dimension-level performance and disconfirmation. Negative performance/disconfirmation on a quality dimension has a greater impact than positive performance/disconfirmation. Pollack
29
provide evidence for the existence of non-linear relationships between some service-quality attributes and satisfaction, and they also identified two types of non-linear patterns. Falk et al.
28
detect positive and asymmetric effects of functional-utilitarian quality attributes on customer satisfaction, and negative asymmetric effects of hedonic quality characteristics exhibit on customer satisfaction. Based on the above discussions, we hypothesize that: H2: The slope of the influence of service quality on positive purchase intentions, like advocacy, would become more positive with a satisfying feeling and become less positive with a dissatisfying service encounter.
Based on the above discussion, satisfaction has possibility to be a mediator and moderator simultaneously. Whereas mediators establish ‘how’ or ‘why’ one variable predicts or causes outcome variables, moderators address ‘when’ or ‘for whom’ predictors are strongly related to outcomes.
33
There is no study to consider the dual roles played by satisfaction. If satisfaction plays dual roles, the relationships among service quality, satisfaction and purchase intentions will become quite complex. This study seeks to empirically explore if satisfaction plays dual roles between service quality and purchase intentions. As such, this study tries to empirically propose the following general proposition: P1: Satisfaction plays dual roles between service quality and purchase intentions.
Methods
Measures
Perceived service quality is to evaluate how well patients perceive their received outpatient services. The tool to evaluate perceived service quality was developed based on original SERVQUAL, 15 and other revised SERVQUALs. 4,34 Using the same items in this battery, the translation and back-translation process was used, and the wording of some items was customized to the outpatient services. One preliminary questionnaire was evaluated by three health-care service experts, who were asked to serve as expert judges to appraise the face validity. Some vocabulary revisions were also made during the iterations. The purpose of this process is to achieve cultural equivalence among diverse populations while applying a different cultural questionnaire in a research study. Seven-point Likert scales (1 = strongly disagree, 7 = strongly agree) were used to measure all items (see Appendix A).
Patient satisfaction was assessed, with two items based on patients' affective responses to the overall experiences of receiving outpatient services. 4 They were: (1) ‘The overall feelings about the health-care service in this hospital are better than what I expected.’ and (2) ‘Overall, I satisfied the services provided by this hospital’.
Purchase intention is to measure how likely patients would be, to want to buy more health-care services in this hospital. 7 The five items modified from Zeithaml et al.'s 7 scale were used to measure the extent: (1) ‘If I need medical service in the future, I will consider this hospital as my first choice,’ (2) ‘If I need medical service in the future, I will go to this hospital more frequently,’ (3) ‘If I feel sick in the next few years, I will go to this hospital less frequently (r).’ All the items of patient satisfaction and purchase intentions were measured on seven-point Likert scales (1 = strongly disagree and 7 = strongly agree).
Finally, past studies conducted in Taiwan showed patient characteristics such as gender, 35 age, 36 education, 35–37 personal average monthly income 35,37 and frequency of going to hospital 37 are relevant to shopping for health-care services. These demographic variables were considered as control variables.
After generating the questionnaire, a pilot test was conducted with 20 outpatients selected from a regional hospital. Minor changes to the questionnaire were made accordingly for appropriateness of wording, content and structure. Such feedback was helpful in refining the quality of the measures.
Sampling
A field survey in Taiwan uses a multistage sampling method. Firstly, the outpatients of 12 regional hospitals (the second-ranking level), which distribute in different districts across Taiwan and have similar scale, were selected. Since the intermediate area of health-care services has not been analysed in detail and it becomes increasingly important, 9 this study tries to explore more about how perceived service quality and satisfaction influence purchase intentions for this area of health-care services.
Secondly, each hospital was despatched 100 questionnaires and the data were collected through convenience sampling. Convenience sampling is deemed appropriate because the purpose of this study is not to provide point and interval estimates of the variables, but to explore the relationships among the variables. 38 Trained personnel randomly selected subjects from the area where outpatients waited to collect their medicine, which is the last stage of the whole outpatient service.
Over a month period, a total of 664 completed responses are received from 1200 interviewed subjects and an acceptable response rate of 55.33% is achieved. The respondents are composed of slightly more women (59.3%) than men (40.7%). Their ages mainly lie between 21 and 40 years old (55.4%), their education level mainly lays at college level (61.8%) and their personal average monthly incomes are largely less than NT 50,000 (70.6%). As to the frequency of going to hospital, 59.5% of subjects go to hospital more than five times and the frequencies are from two to five for 29.9% of the subjects. These frequencies show that our subjects are qualified to evaluate service quality of these hospitals and hence their responses are able to raise the reliability of this study.
Analysis and results
Measurement analysis
In accordance with the research context over the dimensionality of service quality, exploratory factor analysis was used to examining the 22-item SERVQUAL scale. To make the extracted factors more interpretable, the varimax rotation method was performed and the number of factors was determined based on the eigenvalue criterion (λ > 1). Results of a factor analysis, using principal component factoring, presented four dimensions. After a closer examination of the loading on the factors, a name was given to each factor according to the content of the variables making the greatest contribution to each of the dimensions. The four dimensions are named as reliability, responsiveness, assurance and empathy (see Appendix A). To further improve the distinction between factors, items that had factor loadings greater than 0.4 on two or more factors were removed from the measurement. Following purification, two items (SQ17 and SQ20) were dropped. In all, four factors explain 68.84% of the variance.
Discriminant validity (i.e. discriminability of the four service quality dimensions) was checked by computing a 95% confidence interval for each of the estimated correlations among the four dimensions of service quality. 39 The associated confidence interval is 0.07–0.64 and none of the intervals include unity (i.e. 1.00). No case is the correlation between any scale and another as high as its alpha coefficient (see Table 1). Each pair-wise combination of perceived service quality and each outcome construct (e.g. satisfaction and purchase intentions) meets the discriminant validity standards.
Evidence of reliability and discriminant validity for three constructs
Note: Diagonal entries are Cronbach's alpha coefficients, others are correlation coefficients
*P < 0.05
Further, a confirmatory factor analysis, which included all constructs in the model, provided evidence supporting the measurement properties of the dimensions. Although the χ 2 values of the CFA models of the four dimensions are 524.3 (df = 236, P < 0.05), the comparative fit index, goodness-of-fit index and root mean square residual are 0.93, 0.91 and 0.03, respectively. The model's fit as indicated by these estimates is deemed satisfied.
Hierarchical regression analysis
To test the hypotheses, constituent variables were generated for all constructs by obtaining the average rating of the respective items and then the Hierarchical regression analysis was used. The constituent variables were mean-centred before creating the interaction terms to eliminate multicollinearity. 40 Both full and restricted models were developed, and the hypothesized interaction and main effects were examined by comparing of the full- and restricted-regression models. The whole procedure included Model A (in which, dependent variable is patient satisfaction) and Model B (in which, dependent variable is purchase intentions). In Model A, the control variables, four factors of service quality perception and satisfaction were put in. In Model B, an initial regression was run with the control variables and main variables (i.e. four factors of perceived service quality) in the first step, the mediator (satisfaction) added in the second step, and finally the moderator (the hypothesized interactions) added in the last step. The results of a series of hierarchical models are reported in Table 2. The variance inflation factors are well below the cut-off of 10, which suggests that multicollinearity is not a problem. 41
The results of hierarchical regression models
Note: b means the unstandardized coefficient
*P < 0.05
Main effects
In Table 2, the results shown in Model A (R 2 = 43.3%, P < 0.001) and step 1 of Model B (R 2 = 52.35%, P < 0.001) show that the regression model is supported. The coefficients of control variables show that frequency of going to hospital has significant effects on satisfaction (b = 0.13, P = 0.02) and purchase intentions (b = 0.25, P < 0.001). Subjects who usually go to hospital have higher satisfaction and more favourable purchase intentions to hospitals than those who occasionally go to hospital. In addition, all the four dimensions of perceived service quality have positive effects on purchase intentions. Therefore, perceived service quality itself does indeed have a positive influence on purchase intentions.
Mediating effects
Procedures suggested by Baron and Kenny 24 were followed, to assess whether satisfaction mediates the effects of perceived service quality on subjects' purchase intentions. The results, which are presented in Model A and the first two steps of Model B, indicate that reliability, assurance and empathy affect both satisfaction (the mediator) and purchase intentions (the dependent variable). Satisfaction (the mediator) also affects purchase intentions (the dependent variable). These conditions mean that a mediating effect may exist.
Furthermore, when satisfaction (the mediator) was added into Model B as the covariate, the effects of reliability, assurance and empathy on purchase intentions were reduced. As shown in the step 2 of Model B, there is no significant effect (at the P < 0.05 level) of empathy on purchase intentions, once the effect of satisfaction is considered (b Emp = 0.06 → 0.01, P = 0.00 → 0.52). Satisfaction completely mediates the effect of empathy on purchase intentions. 42 The effects of reliability and assurance in the step 1 of Model B are less than in the step 2 of Model B. The b coefficient of reliability is reduced from 0.37 to 0.16 (Sobel test t = 7.12, P < 0.001); the b coefficient of assurance is reduced from 0.33 to 0.17 (Sobel test t = 6.12, P < 0.001). Therefore, satisfaction plays as a partial mediator between reliability/assurance and purchase intentions. 42
Summarily, satisfaction partially mediates the effects of the two dimensions of service quality perception (i.e. reliability and assurance) on purchase intentions and fully mediates the effect of empathy on purchase intentions. However, it does not mediate the relationship between responsiveness and purchase intentions based on the conditions recommended by Baron and Kenny. 24 Therefore H1 is partially supported with three service quality dimensions (i.e. reliability, assurance, and empathy).
Moderating effects
As to the verification of H2, the analysis began by estimating the influence of service quality perception and satisfaction on purchase intentions (the step 2 of Model B). The addition of the interaction terms to the main effects model, increases R 2 by 1.6% (ΔF = 7.08, P < 0.001) in the step 3. Therefore, there should be moderating effects. To assist in the interpretation of interaction, subgroup regression lines were graphed using the mean ± 1 standard deviation. 40 In this procedure, the regression equation was algebraically restructured to express the regression of the criterion variable on the predictor variable at various levels of the moderator variables (see Figure 1).
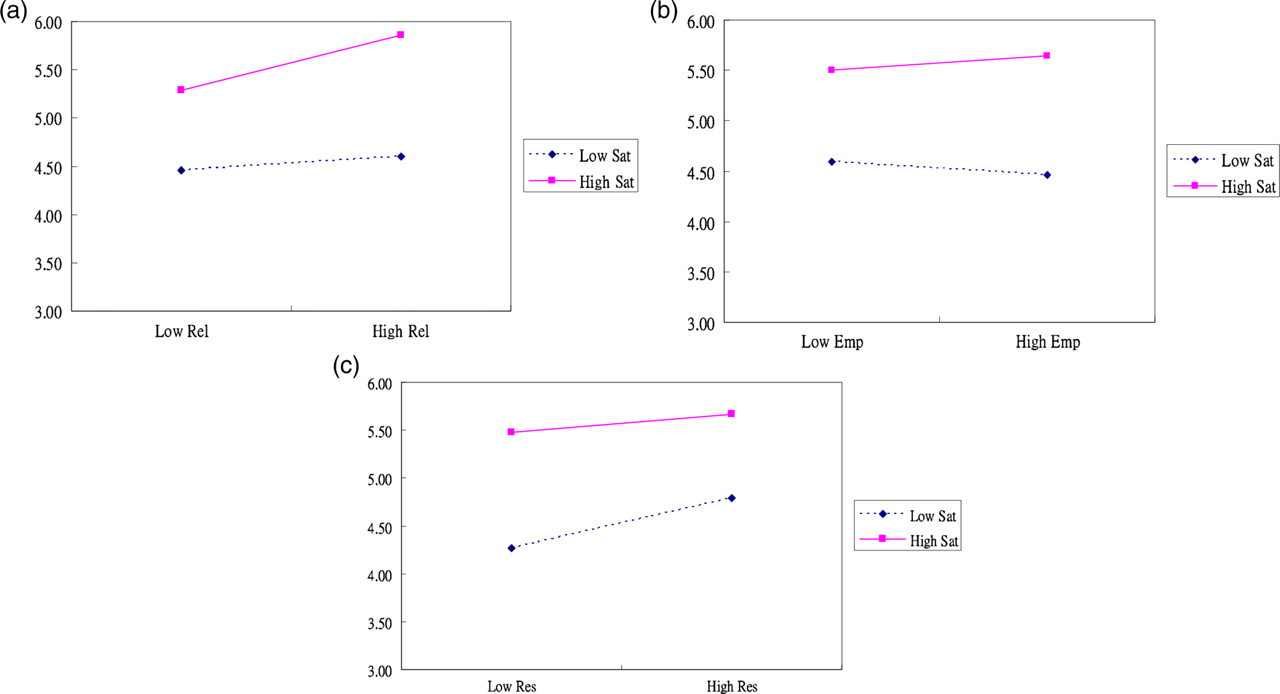
Interactions of service quality perception and satisfaction. (a) Interactions of reliability and satisfaction. (b) Interactions of empathy and satisfaction. (c) Interactions of responsiveness and satisfaction
According to the result of the step 3 in Model B shown in Table 2, satisfaction positively moderates the relationship between reliability and purchase intentions (b Rel×Sat = 0.11, P < 0.05) and the relationship between empathy and purchase intentions (b Emp×Sat = 0.07, P < 0.05). These patterns indicate an enhancing interaction, but forms of the two moderating effects are different. Based on Sharma et al.'s 31 classification of moderators, satisfaction plays as a ‘quasimoderator’ between reliability and purchase intentions, but as a ‘pure moderator’ between empathy and purchase intentions, since empathy is not significantly related to purchase intentions but has interaction with satisfaction.
Figure 1a shows that under the high-satisfaction situation, the higher level of reliability the subjects perceived, the more favourable purchase intentions the subjects presented. By contract, the level of perceived reliability relatively has few effects on purchase intentions under the low-satisfaction situation. In Figure 1b, subjects with high satisfaction are more likely to perceive empathy and do well for hospitals than those with low satisfaction. Further, although the relationship between empathy and purchase intentions is positive for high satisfied subjects, the relationship is negative for low satisfied patients. The positive moderating effect means that satisfaction is likely to enhance purchase intentions when reliability/empathy is high. This means satisfaction has more powerful influence than reliability/empathy on purchase intentions. With high satisfaction, subjects experiencing higher levels of reliability/empathy perception have higher purchase intentions than those with low satisfaction.
Alternatively, there is a negative moderating effect on purchase intentions from satisfaction and responsiveness (b Res×Sat = −0.08, P < 0.05). Since the estimates of the predictors are both positive (b Res = 0.17 and b Sat = 0.52) and the moderating effect is negative, the pattern indicates an antagonistic interaction and thus a compensatory effect of the predictors on the dependent variable. 43 In other words, the greater the satisfaction is, the smaller the effect of responsiveness on purchase intentions is. Figure 1c showed that although both responsiveness and satisfaction have positive effect on purchase intentions, purchase intentions is more strongly affected by responsiveness perception for low satisfied subjects than for high satisfied subjects.
Finally, satisfaction is positively related to assurance (Pearson correlation = 0.57, P < 0.001) but does not interact with assurance (b Ass×Sat = −0.03, P = 0.27). Satisfaction is not referred to as a moderator variable between responsiveness and purchase intentions. 31 It could be concluded that H2 is partially supported with three service quality dimensions (i.e. reliability, responsiveness and empathy).
The dual roles played by satisfaction
Based on the verification of H1 and H2, it is obvious that satisfaction indeed plays dual roles and therefore P1 is supported. Figure 2 summarizes the dual roles played by satisfaction between service quality and purchase intentions. Based on Sharma et al.'s 31 classification of moderators and Sobel 42 's categorization of mediators, there are four conclusions. Firstly, satisfaction plays both a partial mediator and a ‘quasimoderator’ between reliability and purchase intentions. Secondly, satisfaction only plays a ‘quasimoderator’ since both the interaction term and the main effects are significant, and it negatively moderates the influence of responsiveness on purchase intentions. Thirdly, satisfaction only plays a partial mediator between assurance and purchase intentions. Finally, satisfaction fully mediates the influence of empathy on purchase intentions. This full mediation effect makes satisfaction work as a ‘pure moderator’ between empathy and purchase intentions, since empathy is not related to purchase intentions but has interaction with satisfaction.

Relationships among service quality, satisfaction and purchase intentions
Discussion
The study demonstrates that perceived quality and satisfaction impact on purchase intentions collectively and that their effects should be assessed simultaneously. Moreover, the result also provides an empirical support for the proposition that satisfaction plays the dual roles between service quality and purchase intentions. These findings imply that the effects of perceived service quality on purchase intentions are not equal across satisfied and unsatisfied patients. Linear and non-linear relationships exist at the same time for the effects of service quality and satisfaction on purchase intentions.
It is important to discuss how and when service quality and satisfaction simultaneously influence purchase intentions.
Firstly, satisfaction plays a partial mediator as well as a quasimoderator between reliability and purchase intentions. It means that reliability is a less significant predictor of consumers' purchase intentions than satisfaction, 24 and satisfaction is able to strengthen the effect of reliability. 44 In other words, high satisfied patients with higher levels of reliability perception are more likely to have positive purchase intentions to health-care services.
Secondly, satisfaction only plays a quasimoderator and negatively moderates the influence of responsiveness on purchase intentions. It means both responsiveness and satisfaction have significant effects on purchase intentions, but the effect of responsiveness will be modified by satisfaction. The greater the influence of satisfaction on purchase intentions is, the less is the effect of responsiveness on purchase intentions is. Therefore, an unsatisfied patient will feel a hospital less responsive to his requirements than a satisfied one even while the hospital provide the same level of service quality.
Thirdly, satisfaction plays a generative mechanism through which assurance partially affects purchase intentions. Although both assurance and satisfaction have positive influences on purchase intentions, a part of influence of assurance on purchase intentions must go through satisfaction. In other words, a satisfied patient will also feel assurance for purchasing health-care service from a hospital.
Finally, since satisfaction plays a full mediator and pure moderator between empathy and purchase intentions, satisfaction replaces the effect of empathy 44 and empathy must affect purchase intentions fully through satisfaction. An unsatisfied patient also does not believe the hospital is empathic.
Management implications
This paper provides ways for health-care providers and managers to realize how and when service quality and satisfaction simultaneously affect purchase intentions. Based on the findings, some management implications are proposed.
Firstly, service providers should empathize more on customers' emotional feelings than on their cognitive judgement. It has been found that ‘tremendously satisfied’ or ‘delighted’ customers are much more likely to show beneficial purchase intentions to service providers than those who are merely ‘satisfied’. 5 Since customer satisfaction partially reflects price/quality trade-offs, and personal and situational factors, 25 service providers need to improve customers' perceived value while promoting service quality. Adequate marketing activities, which help patients perceive the promised service quality, are helpful to delight patients.
Secondly, not all of the service quality dimensions get the same perception. Under a severely competitive environment, emphasizing reliability is relatively more useful but empathy is less helpful. Since reliable service quality is linked to the level of the perceived risk that patients may expect in a service encounter, raising patients' perceptions of reliability serve as an indicator of the level of satisfaction. 9 In Taiwan, the NHI programme is bound to the hospital accreditation system, which requires hospitals to maintain enough capacity (such as the amounts of human resources, equipments, hospital beds, and so on) of caring patients. These requirements provide the basic reliability (i.e. visible cues) that each patients could have enough health-care resources. Therefore, to benefit customers' perceptions of price/quality trade-offs, service providers could find out which tangible elements are helpful to increase patients' perceived reliability and then present these elements through diversified channels.
Finally, hospital executives should develop customer-oriented strategies at the post-purchase stage of the consumer's decision process. That is, marketing activities should be designed to increase customer satisfaction. In Taiwan, hospital executives' backgrounds are mainly from the medical area, so they usually lack management-related sense and information related to patients' expectations. Hospital executives should pay close attention to the service encounter incidents. For instance, contact patients to check their medicine usage, remind them about matters that may need attention, help patients to make next appointment, familiarize them with other departments or health-care services to form shared care and so on. In such, sufficient relationship focus and adequate service recovery could make patients know that the hospital really concern about what they want.
Footnotes
An Appendix is available for this article at