
Abstract
Background.
The design and protocol of sensory re-education programmes has not changed over the last decades – a fact that may appear surprising when considering the enormous advances in neuroscience, cognitive science and brain imaging techniques that have increased our understanding of brain plasticity. A multitude of intrinsic and extrinsic factors influence the functional outcome after a nerve repair. Timing of when the sensory relearning is begun is one of them.
Methods.
Here we present a case following median nerve repair, where sensory re-education was introduced in the second week following surgery, i.e. long before any signs of nerve regeneration in the hand and fingers (Phase 1 sensory relearning). The aim was to activate and maintain the cortical hand representation areas for median nerve innervated parts of the hand. Mirror training and a new method with auditory input that substitute temporary missing sensory input were used. For evaluation, the Model Instrument for Outcome after Nerve Repair was utilized.
Results.
There was an improvement in overall score especially in the sensory domain of the Model Instrument for Outcome after Nerve Repair over the 25 months and this exceeded the upper limit of the 95% reference interval for an adult population.
Conclusions.
The excellent outcome in this case adds to other studies indicating that very early introduction of sensory relearning can greatly enhance the outcome following nerve repair.
Introduction
Nerve regeneration after a peripheral nerve transection and repair involves complex biological processes where the outcome depends on a multitude of biological and environmental factors such as survival of nerve cells, axonal regeneration rate, extent of axonal misdirection, type of injury, type of nerve, level of the lesion, age of the patient and adherence with training. There are good reasons to look for explanatory factors in the central nervous system in addition to the cellular and biochemical events, which are associated with degeneration, and regeneration in the peripheral nervous system. 1 A major problem in adults is the reorganization of the hand representation, which occurs as a result of rapid cortical changes within hours following the nerve transection as well as axonal misdirection. 2 Although protective sensibility is often achieved following nerve repair, tactile discriminative functions seldom recover – a direct result of the cortical remapping. After the nerve transection and repair, there is a disappearance of the cortical hand representation, which is followed by a rapid expansion, within hours, of the adjacent cortical hand territories. 3
In primate experiments, specific territories for each finger have shown a completely changed pattern, 2 which means the hand speaks a new and distorted language to the brain, which in turn requires a process of relearning. These central events, which are an expression of the brain's capacity for rapid plasticity, play a predominant role in sensory relearning programmes of today. Advances in neuroscience and cognitive sciences have also opened up new possibilities for the future to improve the outcome after nerve repair. 4
The timing for onset of sensory relearning may be of critical importance. Following repair of major nerve trunks, there is an initial period (Phase 1) lasting several months when no regenerating fibres have reached the fingertips and which lacks sensibility. Activation of the cortical hand representation in Phase 1 might be effective for maintaining the cortical hand map. Recent research4–6 has shown that there are several strategies for activating the cortical areas for perception, which might be very useful in the immediate period after a nerve repair. In Phase 1, principles have been presented aiming to maintain the cortical hand representation by using the brain's capacity for sensory imagery, cortical visuo-tactile and audio-tactile interaction.4–6 Phase 1 is followed by Phase 2, which represents re-innervation of the hand. External modulation such as selective temporary cutaneous anaesthesia of the forearm of the injured hand has been reported 7 and has been shown to improve hand sensibility. This method allows expansion of the nerve-injured cortical hand representation, thus enhancing the effects of sensory relearning. 7
Both phases require a specific treatment strategy, and based on previous research, there are good reasons to initiate sensory relearning very early, during the first postoperative days (Phase 1) in order to preserve the cortical hand representation. 4
Here we describe a single case participating in a sensory relearning programme initiated within the first weeks after a peripheral nerve repair using mirror training and a novel audio-tactile interaction tool. The results were evaluated using the Model Instrument for Outcome after Nerve Repair. 8
The patient
Mrs M was a 33-year-old married lady with three children (4 years, 3 years and 18 months old) at the time of the injury, and verbal consent was given for this case to be written and published without identifying information.
Her occupation involved home duties and care of children. She was actively involved in sports, such as playing netball. Mrs M lived 400 km, which is a driving distance of four hours, from the treating hospital in Adelaide, Australia.
Mrs M lacerated her right wrist (dominant hand) in early 2006 during a fall through a window while she was making her bed. The wrist laceration involved 100% division of the median nerve and 10% laceration of flexor carpi ulnaris (FCU). Surgery was performed on the same day as the injury occurred. The median nerve was repaired with 8/0 nylon with excellent alignment. FCU was not repaired. Plaster of Paris was applied in theatre and stayed in situ until she returned as an outpatient. Thirteen days after surgery, sutures were removed and a dorsal wrist splint was made blocking extension at zero degrees with all digits free to move.
Training in Phase 1
The sensory relearning involved:
Visuo-tactile interaction using mirror therapy
Treatment with the use of mirrors was first described by Ramachandran et al. 9 for the prevention and treatment of phantom pain. It gives an illusion of function in a missing or non-functioning hand. The method was based on the concept that the central representation of phantoms and body image can change rapidly, and has been described in the treatment of phantom pain and stroke. 10 A mirror was placed vertically in front of the patient thus reflecting the non-injured hand in the place of the injured hand. The injured arm was positioned behind the mirror, and when touching or moving the non-injured hand it looked – through an illusive effect in the mirror – like a functioning hand. 6
Based on the mirror concept, different surfaces/textures, which could be observed in the mirror, were placed on table. The nerve-injured hand was hidden behind the mirror. The uninjured hand touched, rubbed or stroked different surfaces or textures while looking at the image in the mirror. In addition to traditional range of motion exercises of the nerve-injured hand Mrs M performed hand exercises with the uninjured hand while looking at the image in the mirror.
The written information for mirror therapy was as follows:
Place your hands on either side of the mirror with your un-injured hand so you can see it in the mirror. By looking at the image of your normal hand in the mirror it makes your brain believe that you are looking at/moving/touching your injured hand.
Touch an object with your un-injured hand or fingers and look in the mirror at the same time. Your brain will be told that you are touching with your injured hand/fingers.
Move your uninjured hand/fingers and look in the mirror at the same time. Your brain will be told that you are moving your injured hand/fingers.
The Sensor Glove has been described by Rosén and Lundborg 11 and Lundborg et al. 12 to maintain the cortical hand representation in Phase 1 after a nerve repair. There is multi- and cross-modal activity of the brain based on multisensory neurons that receive more than one type of sensory signals. It has been demonstrated that we are able to extract information from one sensory modality and use it in another by using polymodal association areas.13, 14 In the Sensor Glove System, microphones are mounted dorsally at fingertip level or in a glove connected to earphones – via a miniature stereo processor. With this system the patient can ‘listen’ to what the hand feels. Thus, auditory stimuli substitutes for absent tactile stimuli – specific and typical friction sounds are associated with touching of various textures. However, the Sensor Glove System was commercially unavailable; therefore, to apply the concept a novel audio-tactile interaction tool was used. Two dowels were made out of thermoplastic material with fabrics/textures glued on. In the Sensor Glove, the sound elicited when touching different textures is amplified electronically to earphones. Instead of amplifying the sound, Mrs M was instructed to move the dowels on the finger close to the ear and to listen carefully to the different sounds elicited by different materials (Figure 1). To determine which fabrics/textures to use the therapist tested, together with the patient, if the friction sound could be detected and differentiated while rubbing with Velcro® hook and loop, one at a time, on the non-sensate and dry distal phalanx of thumb, index and middle finger. At this stage, it was difficult to hear the differences between similar textures such as Velcro® (Total Patient Care, North Ryde, NSW, Australia) loop and Fleezyweb™ (Clifford Hallam Healthcare, Pooraka, SA, Australia) on any of the involved digits.

Audio-tactile interaction using detection of friction sound produced by rubbing two different fabric covered dowels made of thermoplastic material
The written information for detection of friction sound was as follows:
At first use two fabrics with very different textures;
Look and listen when you move one injured finger at a time over the surface (or move fabric over the injured finger);
Do the same with the second fabric;
When you are able to hear the difference between the textures, close your eyes, move each finger over the textures one at the time and listen to the sound. See if you can identify the surface by the sound it makes;
Later when you can identify these two surfaces, add one or two more textures, which produce different sounds. Do the same task as above with all the three to four textures.
After the practice session, we recommended the patient to perform the programme at home for five to 10 minutes, two to three times daily in a quiet room.
Hearing, vision and taste have been suggested to help the connections in the somatosensory cortex. 15 Recommendations were made to use other senses such as smell and taste during the day, for example: connect the touch of a fruit when you hold it, peel it and eat it with the smell, the colour, the sound and the taste.
Range of motion exercises and activities of daily living
Mrs M was instructed to do five repetitions of each exercise every waking hour: (1) active range of motion exercise of all joints in the arm and hand; (2) passive abduction of the thumb; and (3) to keep her hand elevated while the hand was swollen.
At this early point in the rehabilitation, Mrs M was advised to limit her use of hand in daily tasks and to prevent injuries as her hand lacked protective sensation in median nerve distribution. ‘Care of the hand with poor feeling’ was explained and written information provided.
After removal of the wrist splint
At six weeks, the dorsal wrist extension block splint was removed and active range of movement exercises of the wrist was commenced.
Mrs M lacked palmar abduction and opposition of her right thumb, and sensibility and sweat in the median nerve distribution.
The Phase 1 sensory relearning was reinforced and encouraged. More details and examples on care of the hand with poor feeling were given as she now was allowed to use her hand in daily activities. To place her thumb in a better functional position, a functional ‘opposition’ strap 16 was made to fit her right thumb with the recommendation to wear it intermittently in daily activities. Precautions and care of the strap were explained.
At 10 weeks, Mrs M found that she could detect a cold apple in her hand. Thumb opposition/abduction was 2+/5 on Manual Muscle Testing (MMT). Tinel's sign was positive at the level of thumb metacarpophalangeal joint. The Phase 1 sensory relearning was reinforced and encouraged. The treating doctor agreed to her returning to playing netball.
Training in Phase 2
At four months, Mrs M reported she used her hand with difficulty in small manipulative tasks such as changing a child's nappy, tying shoelaces and buttoning children's clothes/pyjamas. She perceived holding a sewing needle as sharp. In cold weather, the area of the median nerve distribution was felt to be more numb than in warm weather. The four items in the Cold Sensitivity Severity Scale (1 = not at all and 5 = extreme cold) 17 gave a total score of eight indicating mild impairment. Mrs M was informed that cold sensitivity was likely to decrease with time as the median nerve regenerated. As a coping strategy she was advised to purchase warm gloves from a department store, or if she wished our department could make a sheepskin mitten, and to put the glove on before going out in a cold environment. Other suggestions were to: use holders for cold drinks, wear a glove when taking things out of the freezer, use the unaffected hand or armpit for warmth, and move the hand. Written information ‘How to keep the hand warm’ was provided.
Assessment was undertaken using the Model Instrument for Outcome after Nerve Repair. 8 It is a scoring system that encompasses separate sensory, motor and pain/discomfort domains that are calculated into a ‘total score’ from raw data. The protocol and manual are available at www.hand.mas.lu.se. See Appendix A which shows specific tests that are included as well as the scoring key.
The total score, in our case at four months, showed a score at the upper level of 95% individual prediction interval (Figure 2).
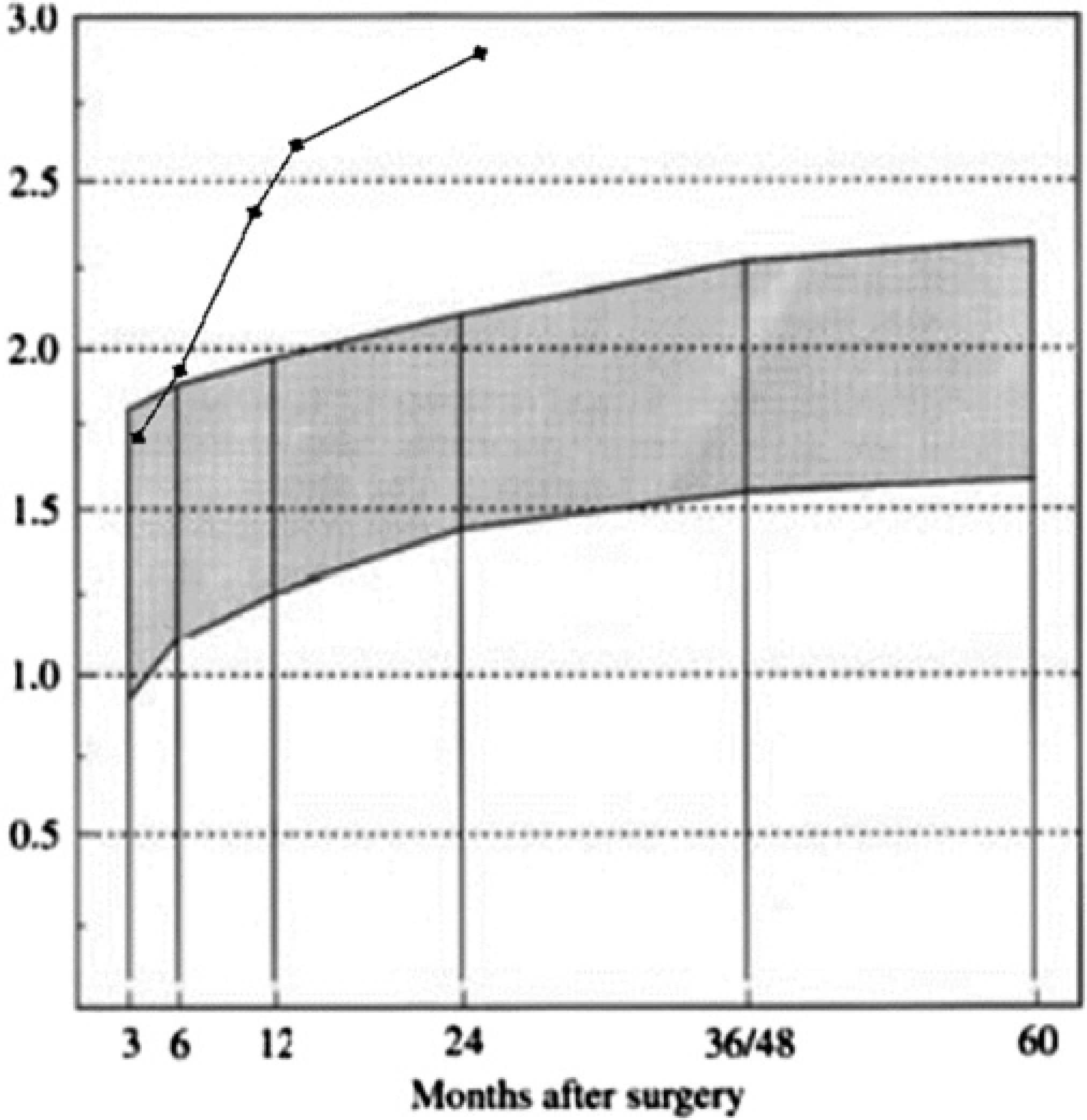
Mrs M's recovery of hand function during the first two years after median nerve repair. All assessments performed by the first author except by E Ames at 14 months. The solid line on the reference graph is Mrs M's score over time. Estimated predicted values for ‘total score’ after repair of the median or ulnar nerve in the distal forearm or at the wrist in adults. The shaded area represents the 95% individual prediction interval. 8 The protocol and manual are available online at www.hand.mas.lu.se
Semmes Weinstein monofilament assessment indicated diminished protective sensation on the distal phalanx of both index and middle fingers and diminished perception of light touch on the distal phalanx of the thumb. Therefore, the classical sensory relearning programme was initiated according to principles described by Wynn-Parry and Salter 18 and Dellon, 19 and written information was provided. After the practice session, it was recommended for Mrs M to perform the programme at home for 5–10 minutes, 2–3 times daily.
At five months, Mrs M reported improvement in hand function in tasks mentioned at four months. She found that netball playing had helped in reducing sensitivity to touch and knocks. Cold sensitivity remained as it was in winter and therefore to cope she wore a warm finger glove indoors as well as outdoors.
MMT for palmar abduction was 3/5. Patient education and prescription of exercises for palmar abduction, function and pinch strength were provided.
At six months, Mrs M reported she used her hand more easily in activities such as putting on earrings. Cold sensitivity remained.
Functional recovery can be seen in Figure 2 and Appendix A. Shape and texture identification (STI) improved. Upgrading of sensory home programme involved: discriminate edges, holes and width of clothes pegs, rolling a pen with soft edges transversely on the finger from the area of normal sensation to the area of reduced sensation.
At 10 months, STI showed a lower score compared with previous assessment, but Sollerman's grip test had a higher score, which meant improved fine motor skill and muscle function of her thumb. She had no indication of cold sensitivity or hyperaesthesia (Appendix A).
Mrs M was advised to train fine motor skill and sensory discrimination by manipulating small objects starting with larger and working towards smaller items such as coins, screw nuts and bolts, safety pins and paper clips. It was also suggested to identify these objects with constant touch and to identify objects in a rice bucket.
At 14 months, Mrs M reported she was able to locate larger objects within a rice bucket, but was unable to identify the objects found by shape and texture. She observed that she was unable to detect if clothes on the washing line were damp or dry with her injured hand.
The tests in the sensory domain were still fluctuating compared with 10 months after the median nerve repair. However, at this assessment, static 2-point discrimination on index finger had improved to 15 mm from greater than 15 mm at previous assessments (Appendix A).
At 25 months, Mrs M requested a follow-up assessment. Results can be seen in Appendix A.
Patient commitment
Mrs M was a highly motivated lady who followed our instructions with few hand therapy appointments. Her interest and commitment was also demonstrated by her request of a follow-up assessment after two years. The early and good median nerve recovery may not be only attributed to surgery and early (Phase 1) sensory relearning programme but also to her ability to use her hand in daily tasks, which involved bilateral manipulation of small objects as she cared for her young children. Mrs M, however, attributes the good recovery to the early relearning programme.
Follow-up was carried out at intervals of 2–4 months up to 14 months postoperatively. Due to the distance for this patient to travel, this occurred less frequently after six months. Generally, we rely on patients performing their programme at home as travel distances can be hundreds of kilometres, which was the case for this patient.
Discussion
Initiating sensory relearning before any innervation has occurred distally (Phase 1) has been demonstrated with this case and reported in the literature.5, 20 This is in line with our experience of other patients who have followed the Phase 1 relearning programme as they have demonstrated the same trend of recovery as Mrs M using the above-described methods.
The recommendation for initiating sensory re-education has traditionally been when there was sign of nerve regeneration in the palm and fingers at approximately three months for a nerve repaired at the wrist level.18, 19 In this case, sensory relearning started on day 13. We attempt to introduce sensory relearning before discharge from the hospital. However, at the present time there is no evidence available to suggest that commencing on day 1 after the peripheral nerve repair will result in a better outcome than commencing on day 13.
Visuo-tactile interaction using mirror therapy as previously described was performed as a home programme with minimal input from the therapists at the hospital. Touching the healthy hand gives an illusion of touching the nerve-injured hand. In these training sessions, a clinical observation is that the patient often gets a perception of the tactile stimuli in the nerve-injured non-sensate hand by the combined mirror illusion and the true touch of the healthy hand.
We have observed that some people have difficulty understanding the image they see in the mirror is the injured hand. Supervised training at the first session is recommended, and some may require more therapy visits during the first few weeks after the nerve repair. In one instance, mirror therapy was excluded for a patient diagnosed with epilepsy as a precaution and in agreement with the patient.
Audio-tactile interaction using detection of friction sound was performed with the novel method of different textures on dowels. It appears, as demonstrated by this case, that dowel textures used as a substitute for the Sensor Glove System, which is not manufactured and commercially available, are a cheap and easy method of training audio-tactile interaction without compromising audio feedback. It should be noted that the sound created from rubbing the dowel texture is more distinct and louder on a finger with sweat than on a finger lacking sweat. Therefore, distraction in the room such as the sound of an air-conditioner can make it impossible to hear the friction sound while rubbing a dowel texture on a finger lacking sweat.
Of the three domains – sensory innervation, motor innervation and pain/discomfort – tactile gnosis as part of the sensory innervation showed the poorest recovery. The median nerve – as in the present case – is over 90% a sensory nerve, which can explain this outcome. This is an area of relearning, which could be much improved to optimize the final outcome.
It appears that activation of the cortical hand representation as described in this case might be effective for maintaining the cortical hand map following a major nerve trauma. There are several alternative strategies to activate the cortical areas for perception that might be useful in the very early period after a peripheral nerve repair (Phase 1). The focus is on maintaining the cortical hand representation by using the brain's capacity for sensory imagery as well as cortical visuo-tactile and audio-tactile interaction.
Phase 1 starts immediately after the nerve injury and lasts until there is some sensibility present in the hand. The sensory relearning in this early phase, in combination with training of the mobility of the hand, is aimed at activating and maintaining the hand map in the brain to make the sensory relearning easier once the axons have re-grown. This is achieved by giving the brain an illusion of sensibility in the hand.
The use of vision to guide the re-training of sensation is the basis for classic sensory relearning, but there is a continuous interplay between all senses. 14
Visuo-tactile interaction is an alternative way of feeding the sensory cortex with relevant tactile input during Phase 1. A few observations have been reported on sensory imagery with involvement of primary sensory cortical areas, which is a hypothetical alternative in Phase 1 after a nerve repair. Just thinking about stroking the dorsum of the hand activates sensory cortex. 21 In this preparation of the sensory cortex in Phase 1 when the sensibility is diminished or completely lost, the patient can try to imagine touch on the hand.
Activation of motor neurons – ‘mirror neurons’ in the premotor cortex by the mere observation of hand motor actions is a well-known phenomenon, which is believed to play a fundamental role in both action and imitation.22–26 Mirror neuron areas are also involved in understanding the intention of actions. 27 Reading or listening to action words, related to hand movements activate hand representational areas in the motor cortex, 28 and hypothetically reading or listening to ‘sensory’ words or watching ‘sensory’ pictures would relate to activity in the somatosensory cortex. There are ways to activate the somatosensory cortex for example by observing a body part being touched. We have, in pilot experiments, demonstrated a visuo-tactile cortical interaction during observation of tactile stimulation on the hand. 29 The patient's observation of his/her hand being touched is one component of early sensory training – first day after surgery – which might activate the cortical hand area due to visuo-tactile interaction.
Whatever method is chosen in Phase 1 after the nerve repair, there are good reasons to start sensory relearning much earlier than we do with the aim of minimizing the reorganization process in the somatosensory cortex, which is induced by the nerve injury. The patient must be comfortable with the exercises, and the patient's understanding of the purpose of such a training in Phase 1 is of utmost importance.
Conclusion
The case, an adult with a median nerve transection at the wrist level, commenced sensory relearning on day 13 after nerve repair. The programme involved visuo-tactile interaction using mirror therapy and audio-tactile interaction using detection of friction sound using the department-made dowel textures. The recovery for Mrs M was in line with other studies where Phase 1 sensory relearning had been initiated before any re-innervation had occurred in the palm and fingers.
The data from this case support that sensory relearning should start before any re-innervation in the palm and fingers has occurred, using visuo-tactile interaction with mirror therapy and audio-tactile interaction using detection of friction sound.
Footnotes
Acknowledgements:
We acknowledge the patient allowing us to use her as a case study and Erica Ames, Senior Occupational Therapist, for assessment, treatment, taking the photos to illustrate the audio-tactile interaction and her contribution to the manuscript.
Appendix