
Abstract
Background.
Surgery on musicians must be entered into cautiously and should be the only treatment option indicated after trialling all other appropriate ones. There are four main principles that must be carefully considered when operating on musicians: the exact location of incisions, anatomic repair and reconstruction, adjustment of any anticipated anatomic compromise to the musician's specific musical needs and the need for an early return to limited playing. The purpose of this case review was to identify which instrument and what medical condition require the most time for the musician to fully return to playing. This in turn can assist in realistic goal setting with individual patients according to these two categories.
Methods.
A retrospective review of a single surgeon's case series of 130 professional musicians was undertaken. Data regarding their medical condition, instrument played, length of time off the instrument following surgery and the time taken to return to full normal professional playing were recorded and analysed.
Results.
A total of 97.7 percent of the patients returned to full time playing and there was a 2.3% ‘failure’ rate. The results indicate that piano players appear to initially take the most time to return to their instrument and string players take the most time to fully rehabilitate. Trauma appears to be the most difficult condition from which to initially recover however, nerve decompressions (with the exception of carpal tunnel releases) take the most time to fully rehabilitate. The most common medical condition requiring surgical intervention was nerve compressions and the piano was the most common instrument played in the series.
Conclusions.
This case series highlights the importance of early return to playing and utilizing the musical instrument as a therapeutic tool in the rehabilitation programme of musicians.
Introduction
Musicians’ hands are vital to their musical performance. Musicians often have to perform to the limit of their abilities physically, emotionally and spiritually. They utilize rapid, complex, coordinated movements. Sometimes they are required to play in less than ideal environments and usually they do not have a medical team to support them in the way sports medicine supports sports people. Musicians can be required to play long tours with poor facilities. Noise, drug and alcohol levels and pressures can be high. They frequently injure themselves or acquire injuries that can lead to difficulties or an inability to play their instrument.
Wynn Parry 1 made a detailed analysis of 1046 musicians he has personally seen at the British Association for Performing Arts Medicine clinics. Clear-cut pathologies in which a specific diagnosis could be made were evident in just over 48% of this group. Of the structural disorders four broad categories were evident: old injuries (22%), tenosynovitis (12%), hypermobility (9%) and focal hand dystonia (5%). In the remaining 52% few physical signs could be found, and the symptoms were seen as being very general and due to performance-related issues such as incorrect practice/technique when playing their instrument.
The potential implications of surgery are serious for a musician, whose hands are their livelihood, and thus respect for their hand and career must be paramount. Accurate diagnosis, analysis of needs, the and extent of disability and precision in planning all need to be carefully considered in order to ensure optimal outcome from surgery. In the area of acute trauma, techniques that will permit early return to function, such as rigid fixation of fractures and early rehabilitation, are often advantageous. Other conditions such as carpal/cubital tunnel syndrome, which has been electrodiagnostically documented and has not responded to activity modification or non-operative interventions and ligamentous injuries leading to instability, can be considered appropriate surgical conditions in the musician's hand. 2
Surgery on musicians must be entered into cautiously. Either all other treatment options should have been trialled first, or surgery must be the only appropriate treatment indicated. Importantly, the interface (relationship between the musician's body and the instrument) must be assessed and altered as necessary, prior to surgery, for most conditions. Frequently utilizing splints, or strengthening particular muscles in order to facilitate proprioceptive awareness and maintenance of more neutral joint positions is adequate intervention when treating musicians and surgery can be avoided. 3 Particular attention must be paid to technique if the patient is hypermobile, with education, adaptive devices for the instrument and exercises to strengthen the muscles of the hand and wrist being implemented. 4 Surgery is often seen as the last treatment option available to a musician.
Winspur 5 reports that of the musicians presenting with recognizable orthopaedic or rheumatological conditions in the upper limb, 4–6% will be candidates for surgery. Non-surgical treatment should always be tried first and it should not be forgotten that in some situations adjustment or modification of the instrument or playing technique (the interface) may solve the problem rather than surgery.
Winspur 6 outlines four areas that must be identified and specifically addressed when planning surgery on a musician's hand:
The incisions must avoid critical tactile areas;
Repair and reconstruction should be anatomical whenever possible;
Adjustment must be considered for any anatomic compromise to the musician's specific musical needs;
The surgery should allow for an early return to limited playing of the musical instrument.
If surgery is performed on a musician, then a graded return to play program is integral. This is a structured protocol, and is essential to ensure safe return to playing and to monitor symptoms as the return to play occurs. It is critical that the treating clinical team be fully educated in both the psychological and practical aspects of guiding patients through the difficult and often treacherous stages of resuming full musical activities so as to avoid the despair that can accompany setbacks, treatment failure or career abandonment. To get musician's back to their preinjury performance level can take a long time. A graded return to play programme provides an outline as to how this can be achieved. A gentle encouraging approach by the treating medical professional is often necessary to keep the musician in good spirits and to facilitate a gentle pace of return to play. The return to play schedule can and should be modified to suit each individual player. The progression is three dimensional: gradually increasing duration, tempo and technical difficulty of the material. 7
The purpose of this retrospective case review was to identify which instrument and what medical condition require the most time for the musician to fully return to playing. This in turn can assist in realistic goal setting with individual patients according to the above two categories.
Methods
A retrospective review of 130 professional musicians who were operated on by a single surgeon was undertaken. Details regarding the instrument played, diagnosis, surgical procedure, time off the instrument following surgery and time taken to return to part- and full-time playing were recorded for all patients by the treating hand therapist.
To be included in the series, the musician had to be a ‘professional’. The term ‘professional’ was defined as ‘a musician who earns their living entirely or predominately from playing one or more musical instruments, or a music student who is in their final year of full time studies’. These parameters were chosen, as it meant there was a measurable endpoint, i.e. the point at which the musician returns to playing/work at the same level or income as prior to the injury/surgery.
All other appropriate treatment options had been trialled with the 130 patients, and surgery was viewed as the only treatment that could assist them to return to playing/performing.
A single surgeon operated on all the cases, and there were two principal hand therapists, both at Clinical Specialist level, who provided the postoperative therapy and collected data. This information has been gathered over the last 26 years of the surgeon's clinical practice.
Results
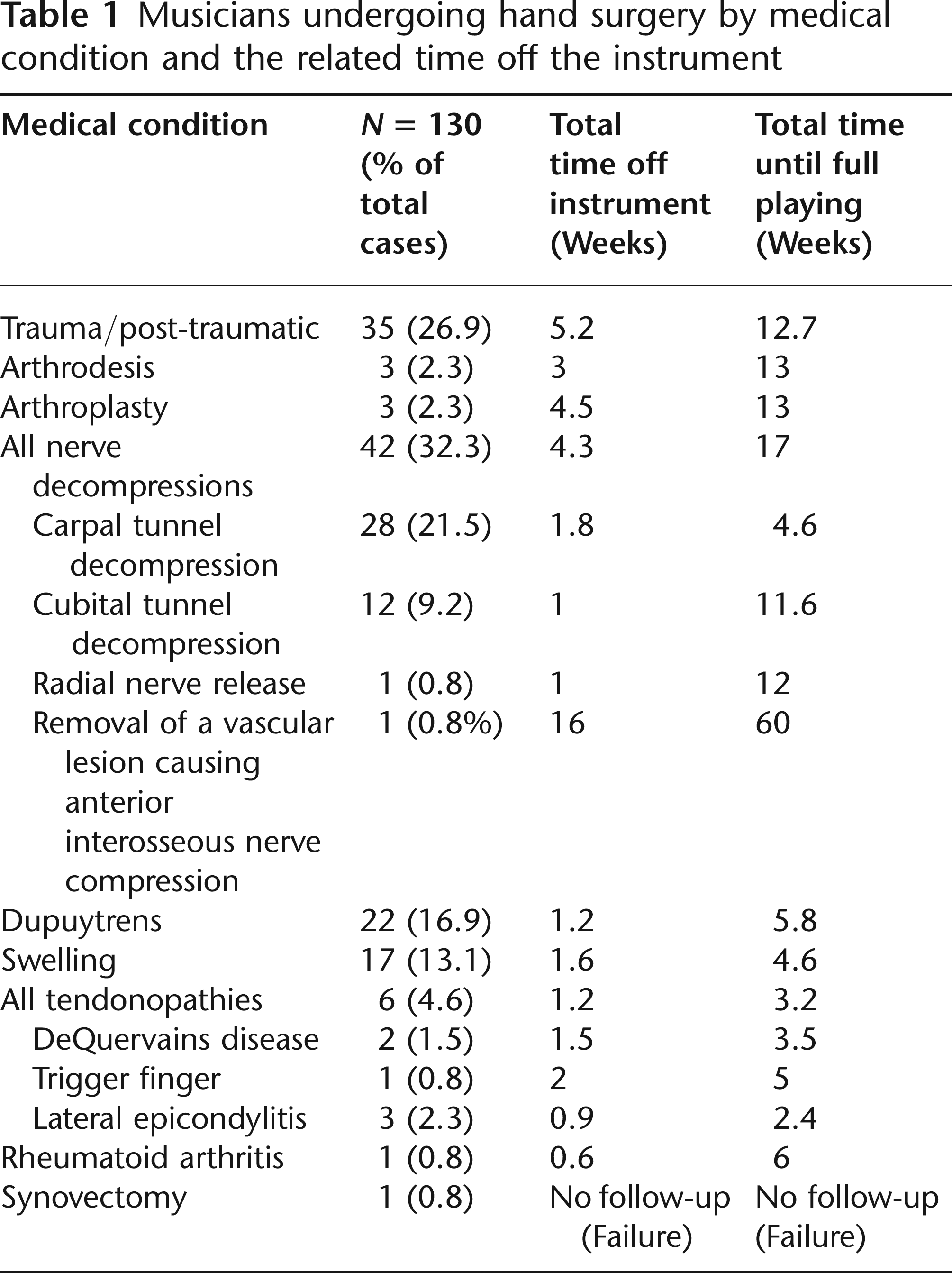
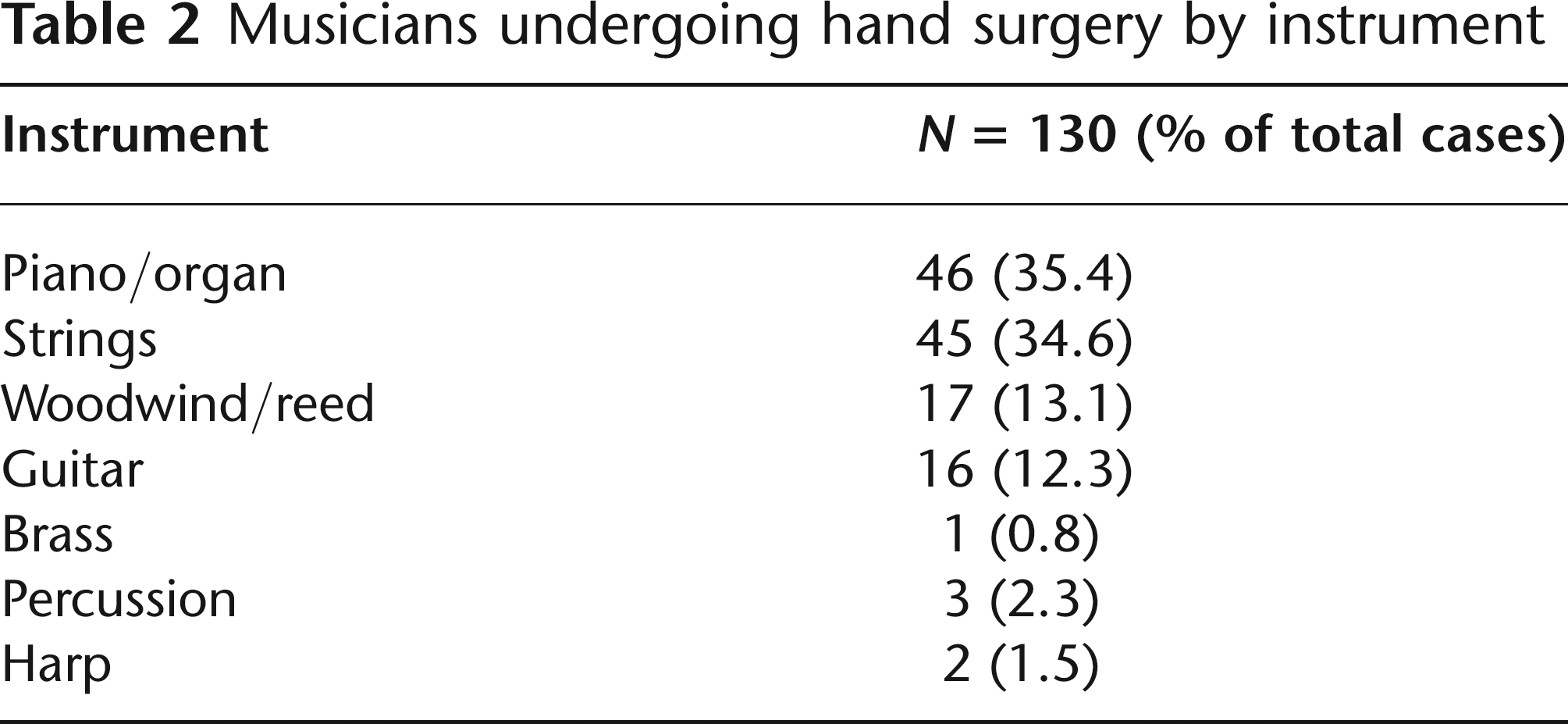
Table 1 outlines the musicians undergoing hand surgery according to medical condition and the related time off the instrument. Table 2 presents musicians undergoing hand surgery by instrument. Figure 1 shows time off the instrument by instrument.
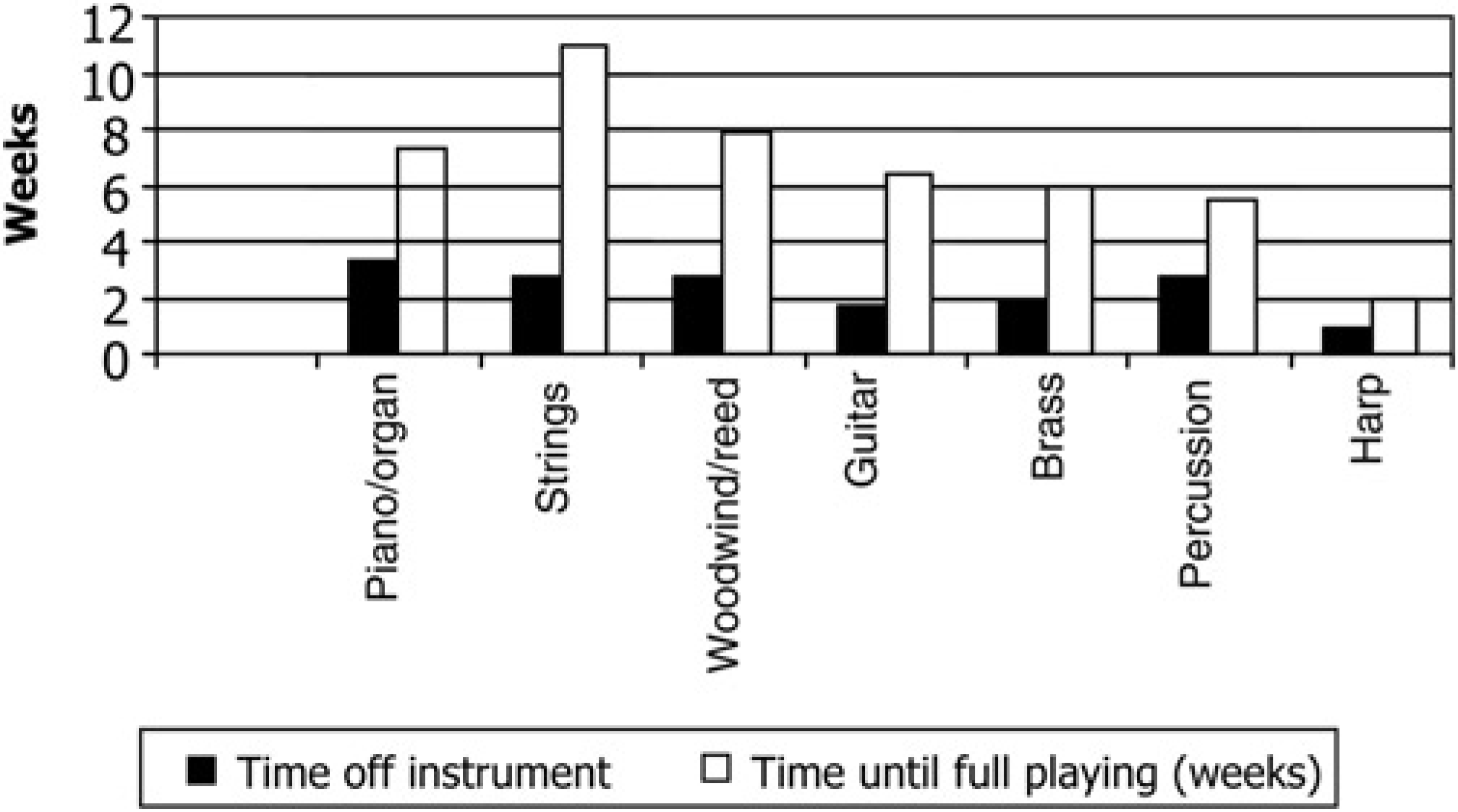
Time off each instrument (in weeks)
Musicians undergoing hand surgery by medical condition and the related time off the instrument
Musicians undergoing hand surgery by instrument
Of the 130 patients, 127 (97.7%) returned to full-time professional work or were able to complete their final year music college examinations.
Piano players appear to take the longest time to initially return to their instrument (3.3 weeks), while string players appear to take the most time to fully rehabilitate (11 weeks), i.e. return to full playing on their instrument. Of the 130 patients, 46 (35.4%) musicians undergoing hand surgery played the piano or organ as their primary instrument.
Trauma appears to be the most difficult condition from which to initially recover, with patients taking an average of 5.2 weeks to return to part-time playing. Full return to playing took the nerve release group an average of 17 weeks, the arthrodesis and arthroplasty groups 13 weeks and the trauma group 12.7 weeks. The most common medical condition requiring surgery in the series was nerve compressions 42/130 (32.3%).
There were three patients (2.3%) who were deemed as not successful, in that they did not return to their prior professional performance level. The first presented with abnormal nerve conduction studies, but despite having a carpal tunnel release required spinal surgery due to multilevel cervical disc disease. This patient was able to return to teaching but not performing at a professional level after spinal surgery. The second was a young pianist who had a hypermobile thumb, and while she was lost to follow-up, early surgical results following a synovectomy appeared to be unsatisfactory. The third presented with a hypermobile distal radial ulnar joint and did not return to full-time professional performance levels, but rather teaches the instrument, due to a recurrent dislocating extensor carpi ulnaris.
Discussion
The purpose of this series was to assess how long it took performers to get back to playing their particular instrument related to the medical condition and relevant surgery that they underwent. This in turn is thought to be useful as it will guide the patient and treating multidisciplinary team into realistic expectations with regard to the time taken to rehabilitate fully from specific medical conditions and the instrument played.
The frequency of musicians suffering co-incidental trauma is higher than demonstrated in this series because of the tertiary nature of the surgeon's practice. Coincidental trauma will normally represent over 50% of the surgery performed on this patient group.
The frequency of piano and string players represents the popularity of these instruments rather than a vulnerability of the players.
‘Time off the instrument’ means no playing of the instrument at all; this may be due to the fact that biologically it is not feasible to play or the wounds are still open. The period of ‘time off the instrument’ is kept to a minimum, and then there is a graded return to play programme that is initiated. Initially, this may start as ‘air playing’ where, for example, the musician holds the bow but does not place it on the instrument and mimics the action of playing rather than actually making any sound. This may be followed by light non-acoustic sessions, where only part force is exerted, or the instrument has the string tension altered or the material that the strings are fabricated from altered in order to decrease friction and increase the ease of return to some level of playing. Timed short sessions are commenced. These can be gradually increased in intensity and difficulty of repertoire, and eventually longer more difficult repertoires can be incorporated prior to the eventual ‘full playing’ on the instrument with normal repertoire (Appendix A). 8
Return to play schedule
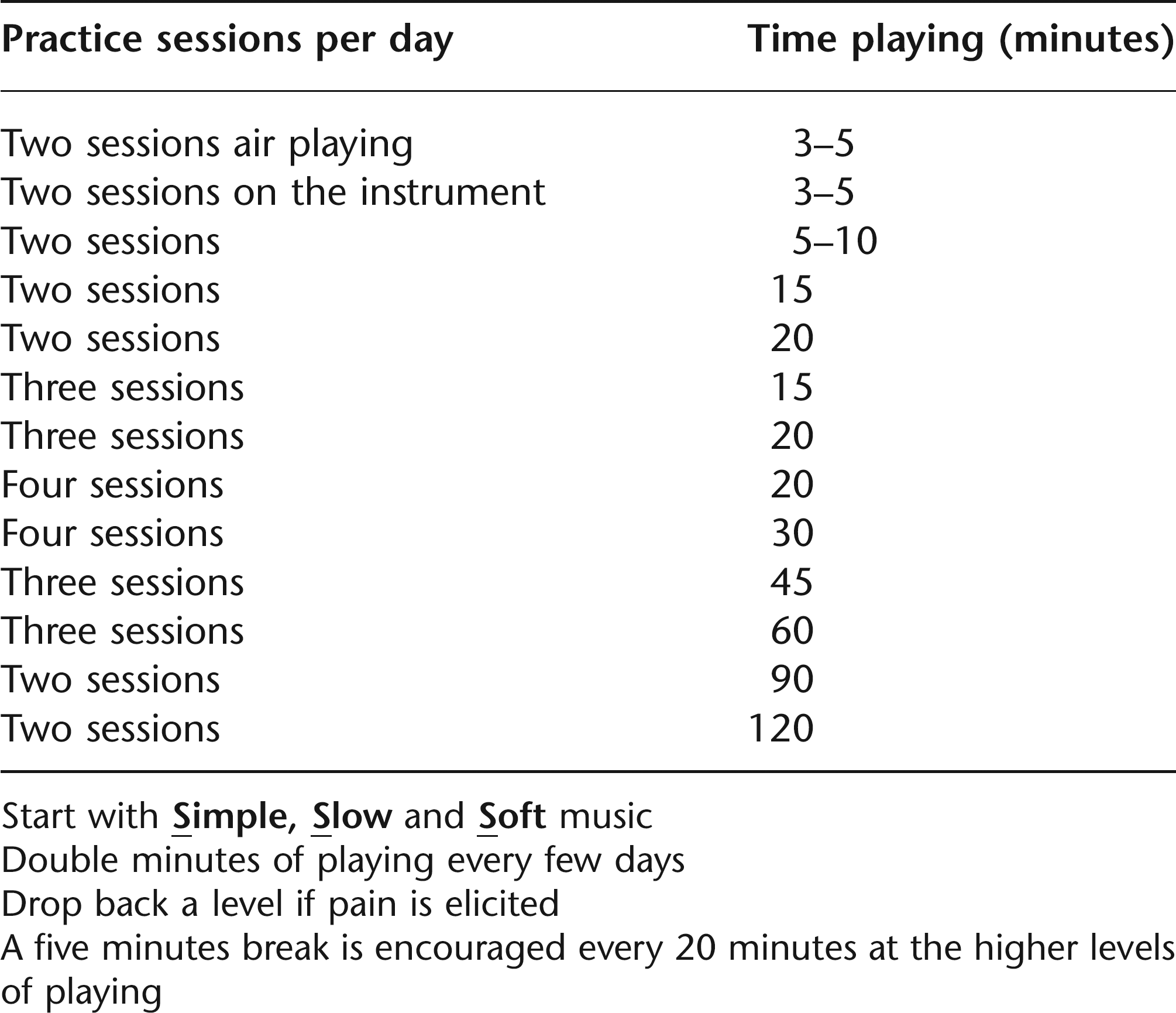
Start with
Double minutes of playing every few days
Drop back a level if pain is elicited
A five minutes break is encouraged every 20 minutes at the higher levels of playing
The movements required for a musician to play the piano are extreme. They are required to utilize repetitive full opposition of the thumb and considerable abduction and adduction of each finger, and thus it is no surprise that this patient group takes the longest time to initially return to the instrument. The general physical demands of an orchestral string player are also high, as they are required to play for long periods of time and frequently do not have many breaks during concerti or symphonies in which to rest or stretch, and the string grouping is the one that takes the longest time to fully return to playing their instrument following surgery.
Illustrative case
Mrs X had a 35-year history of rheumatoid arthritis, and amazingly still continued to play the piano and teach. She was finding it increasingly difficult due to severe ulnar deviation at the metacarpal phalangeal joint (MCPJ) level of her left ring finger. This was compromising the movement of both this finger and the adjacent small finger. A cross-intrinsic transfer with synovectomy was performed. The patient started light piano playing four days after surgery. Six days following surgery a dynamic MCPJ extension splint with radial pull was fabricated for the patient for use during the day, while continuing to increase playing the piano in a formal controlled and measured fashion. At night the patient rested in a splint with an ulnar border to protect the left ring finger's ulnar collateral ligament. Twenty-five days following surgery the patient stated: ‘I had wanted to get rid of the horrible lump on my finger, and any advance improvement in piano playing was to be a bonus! I have been amazed with the results, as I have not been able to play like this for 20 years, and I did not think this improvement was possible. My finger is articulating as it hasn't for 20 years, articulation is crisp, and my husband has commented that he can hear a difference. My arm does ache, as does my finger, but the playing is good; I am playing four 20 minute sessions per day already!’
Conclusions
There appear to be some important points that must be considered when working with musicians who may require surgical intervention. All other treatment options must be trialled first, where appropriate, prior to surgery being performed. Surgery must only be considered when the condition interferes with the musician playing their instrument. Surgery must be strongly indicated and the pros and cons of the surgery must be discussed clearly with each patient with respect to lifestyle, level of performance and demands of their instrument. The musical instrument must be utilized as the rehabilitative tool in order to gain confidence levels, range of motion, desensitization, strength and psychological support during the rehabilitation phase, and thus strong surgical techniques that can withstand early return to play must be implemented when appropriate and indicated. A specialized, multidisciplinary and instrument-focused approach is absolutely necessary when rehabilitating musicians. 8 Other therapeutic devices such as splints can assist patients who are hypermobile or require retraining as to what is an ergonomically correct way of holding the instrument (Figure 2). 3

(a) Left hand of violin player, displaying hyperextension of the index finger metacarpal phalangeal joint (b) Conservative management of the hypermobile metacarpal phalangeal joint utilizing an Orfilight™ dorsal blocking splint, which is a modification of a splint designed by Butler and Svens 9 (c) Side view of dorsal blocking splint, showing that the palmar aspect of the affected left index finger is able to articulate freely with the neck of the instrument
It was found in this series that nerve decompressions, with the exception of carpal tunnel releases, require the longest time to rehabilitate. Piano players appear to take the longest time to initially return to their instrument, while string players appear to take the most time to fully rehabilitate on their instrument.
This large series demonstrates that appropriate surgical intervention will not end a musician's career, provided it is performed properly, for the correct reasons and with postoperative instrument-focused hand therapy available.