
Abstract
Objective
The purpose of this case report was to evaluate the effectiveness of the ‘technique for extensor tendon acceleration’ (TETA) in improving an active extensor lag at the metacarpophalangeal (MCP) and proximal interphalangeal (PIP) joints after a surgically repaired, stable metacarpal fracture (MCF). The TETA was used in combination with scar mobilization, exercise and splinting with an injured soldier who sustained an MCF while on active duty.
Methods
This case report is about a soldier injured during the Iraq War who used the TETA, in combination with other treatments, as a means for resolving an extensor lag in a stable fourth digit MCF. The pre- and post-TETA outcome measure was range of motion (ROM). The ROM was taken before initiation of the TETA and two weeks after its initiation.
Results
After two weeks of performing the TETA in combination with other treatments, the soldier demonstrated a measurable improvement in the extensor lags at both the MCP and PIP joints. The soldier's fourth digit total active motion improved by 55° while the MCP joint extensor lag improved by 10° and the PIP joint extensor lag improved by 20°.
Conclusion
This case report demonstrated a potential benefit for using the TETA in conjunction with other treatments in overcoming an active extensor lag after a stable MCF. These results are case specific and may not be generalized to a larger population until future research studies can be conducted.
Introduction
Most metacarpal fractures (MCF) occur in men between the ages of 10 and 29 years usually from a motor vehicle accident, sports-related injury or by striking a solid object. 1 According to Gonzalez et al. 2 MCFs sustained during military operations can occur from high-velocity gunshot injuries. These hand injuries can cause massive bone and soft tissue loss that can lead to metacarpal shortening, instability and loss of function. 2
An extensor lag is a complication that can occur after an MCF. An extensor lag is an inability to actively extend the metacarpophalangeal (MCP) and/or proximal interphalangeal (PIP) joint fully. An extensor lag can occur for many reasons. Some of those reasons may include but are not limited to: adhesions formed between the extensor mechanism and the fracture site which can result in loss of extensor glide at the PIP joint; 3 bone loss/metacarpal shortening and subsequent extensor tendon lengthening as seen in oblique MCFs resulting in an extensor lag at the MCP joint; 4 metacarpal angulation of over 15° as seen in metacarpal neck fractures resulting in MCP extensor lags; 4 soft tissue injury to the intrinsic muscles of the hand resulting in weakness, muscle imbalance and extensor lag; 4 and scar retraction and extensor tendon adhesion resulting in extensor lags at the PIP and/or MCP joints. 5
Method
A 19-year-old male soldier serving in an infantry division in the Iraq War sustained an MCF as a result of a roadside bomb that hit the infantry's convoy. The injuries sustained were caused by high-velocity imbedded shrapnel to the right side of the soldier's body and included injuries to the ankle, hip, shoulder and hand. The soldier's hand injury was an open fracture to the fourth metacarpal (Figure 1). The soldier had surgery to repair the injury that included internal fixation towards the proximal portion of the metacarpal and a bone graft at the distal end of the metacarpal. The soldier in this case was treated with two small screws for proximal metacarpal alignment and stability, but because of bone loss at the distal metacarpal end, bone grafted from the soldier's hip was used to improve the bone's contour and decrease the chance of shortening of the metacarpal. During the soldier's surgical fixation, an extraction of the shrapnel was also performed. Due to the nature of the injury, the soldier did suffer concomitant soft tissue injuries from bomb detonation but according to the surgical report, an extensor tendon repair was not required.

Scan of right fourth metacarpal fracture s/p internal fixation, bone graft, imbedded shrapnel
The soldier was allowed four weeks of convalescent leave with required attendance at an outpatient hand therapy centre for continuation of his rehabilitation. The therapist (a civilian certified hand therapist) was contacted by the soldier's military certified hand therapist and was given details about his case. The soldier presented to therapy with an order for scar mobilization, aggressive range of motion (ROM) and strengthening.
At the initial evaluation, the therapist's visual observation was that the soldier had an active extensor lag at the right fourth MCP and PIP joints and he had an overall lack of active finger flexion. The soldier presented with a sizeable scar to the dorsum of his right hand. The scar was a combination of where shrapnel entered the hand and where surgery was performed. The therapist noted that when the soldier attempted active finger flexion and extension the dorsal hand scar was immobile, appeared adhered to the underlying tissues, and was restricting active movement.
The soldier reported that he was casted for two weeks after surgery. After two weeks, he was instructed to perform active ROM (AROM) exercises, of which the soldier reported compliance.
The therapist and soldier developed a four-week treatment programme to address ROM deficits and scar immobility. The treatment programme includes standard components often found effective in reducing scar tissue adhesion and improving ROM. These components are as follows:
multidirectional scar massage with lotion Dycem® (Sammons Preston, St Paul, MN, USA) placed directly over the scar to downwardly stretch the scar while the soldier performed active finger flexion exercises Cica-CareTM silicone gel sheets (Sammons Preston) for night wear to apply pressure in order to decrease collagen synthesis scar pump (Sammons Preston) to pull the adhered scar tissue away from the underlying tissue AROM exercises tendon gliding passive ROM (PROM) exercises Hand Helper II® (Sammons Preston) (i.e. Gripper) Sammons Preston Therapy Putty (Sammons Preston) upper extremity progressive resistive exercises night time finger extension splint.
The therapist treated the soldier with the aforementioned treatment programme for two weeks but did not observe a significant change in the extensor lag. At this time, the soldier's AROM of the right fourth digit was (extension/flexion): MCP joint: −30/35°; PIP joint: −35/95°; DIP (distal interphalangeal) joint: 0/60°; for a total active motion (TAM) of 125° (Figures 2 and 3). The soldier had full passive extension of the fourth digit MCP and PIP joints; however, he continued to display an active extensor lag at these joints. Due to the lack of progress, the therapist hypothesized that the active extensor lag at the MCP and PIP joints was caused primarily from the sizeable dorsal hand scar and extensor tendon adhesion. The therapist believed that the soldier did not have severely affected MCP or PIP joint restriction because he had full passive extension and near full passive flexion. As a result, the ‘technique for extensor tendon acceleration’ (TETA) by Brown et al. was incorporated into the soldier's treatment programme in order to try to improve the extensor lag.

Pre-TETA flexion of the fourth digit
Pre-TETA extension of the fourth digit
The goal of TETA is to achieve the maximum degree of tendon excursion with the specific purpose of overcoming extensor lag at the PIP and/or MCP joints. 6 The TETA is intended to work with patients who have sustained fractures of the proximal phalanx or metacarpal, have stable fixation and have an intact extensor tendon overlying the fixated fracture site. 6 The technique addresses the primary barriers to achieving extensor tendon excursion during the scar maturation phase; therefore, it is not considered as useful on scars that are already mature. 6 Ideally, the TETA should be initiated 48 hours postoperatively at one set of 20 repetitions each hour while the patient is awake. 6 The TETA was successful when used in conjunction with other hand therapy elements. 6
The technique for extensor tendon acceleration is divided into the following three stages:
stage one:
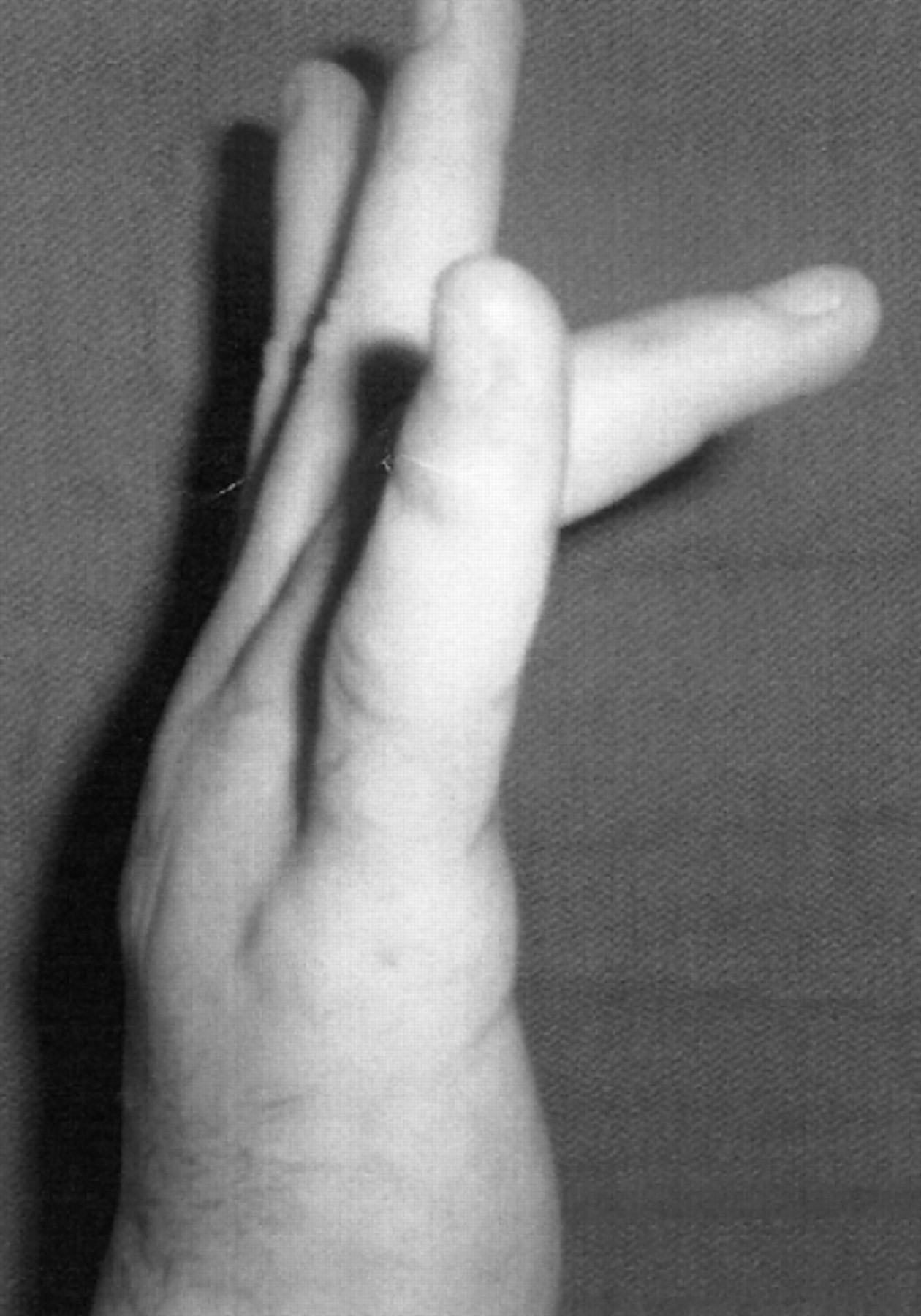
the injured digit is placed in full passive MCP flexion by the thumb of the injured hand the thumb maintains the flexed MCP joint while an isometric contraction is performed for three seconds with resistance on the proximal phalanx into extension (Figure 4) the TETA authors theorize the scar tissue is being re-aligned and lengthened at this point stage two:
the injured digit is released by the thumb rapidly the injured digit undergoes a maximum concentric contraction while moving the MCP joint into full active extension (Figure 5) the TETA authors theorize that the strong contraction from an isometric contraction to a concentric contraction is thought to create a velocity that will break scar adhesions and allow active pull-through of the adhered tendon stage three:
the joint is held in the final extended position for three seconds (Figure 6). Stage 1 TETA of metacarpophalangeal joint Stage 2 TETA of metacarpophalangeal joint Stage 3 TETA of metacarpophalangeal joint



The stages of TETA are performed as one set of 20 repetitions and repeated every waking hour. The TETA can be performed again with resistance on the middle phalanx and the final position focus is on PIP joint extension (Figures 7 –9).

Stage 1 TETA of proximal interphalangeal joint

Stage 2 TETA of proximal interphalangeal joint

Stage 3 TETA of proximal interphalangeal joint
Results
After two weeks of performing TETA, the soldier's right fourth digit ROM was as follows: MCP joint: −20/95°; PIP joint: −15/95°; DIP joint: 0/65° and TAM: 180°. When the therapist compared the pre-ROM and post-ROM measurements, the soldier's TAM had improved by 55° (Figures 10 and 11). In addition, the extensor lag at the MCP joint improved by 10° and the PIP joint extensor lag improved by 20°.

Post-TETA flexion of the fourth digit. (Note: pre-TETA pictures and post-TETA pictures are taken at different angles and may therefore not present an accurate portrayal of the actual changes that occurred in ROM.)

Post-TETA extension of the fourth digit. (Note: pre-TETA pictures and post-TETA pictures are taken at different angles and may therefore not present an accurate portrayal of the actual changes that occurred in ROM.)
Discussion
The aim of this report was to trial a novel technique with conventional techniques to overcome an extensor lag in an MCF. The technique for extensor tendon acceleration (TETA) was successfully implemented in combination with scar mobilization, exercise and splinting for improving an injured soldier's active extensor lag associated with a six-week old stable MCF.
Even though improvement was observed, there could be an argument that a 10° improvement at the MCP joint and a 20° improvement at the PIP joint are not substantial. According to Brown et al. 6 the technique is not considered effective on scars that are already mature. The TETA authors report that both the extensor tendon and the surrounding immature scar tissue are viscoelastic. 6 The protocol takes advantage of the viscoelastic nature of both structures to create the effect of differential excursion; then, it breaks the immature link between the two tissues. 6
A limitation to the report may be that TETA implementation did not start until six weeks after the MCF was stabilized, which does not follow the recommendation of initiating TETA. The therapist realized that the likelihood of fully overcoming the extensor lag, if it was fully due to scar adhesions, was decreased secondary to the maturity of the scar tissue. If there had been more time with the soldier, there may have been a greater outcome in the extensor lag at the MCP and PIP joints. However, the results may demonstrate that the TETA is less effective on mature adhesions than on new, not yet formed adhesions, thus supporting the requirements set forth by the authors of the technique. 6
Another limitation of this report is whether or not the therapist should have emphasized extension exercises only instead of performing both flexion and extension exercises. According to Freeland et al. 3 in order to improve an extensor lag at the PIP joint, one should avoid stretching the joint into flexion. As the PIP joint flexes, the central slip stretches distal to the scar adhesion. 3 This may improve PIP joint flexion; however, the extensor lag still remains. 3 The therapist did have the soldier perform both finger flexion and extension exercises, which may have been counterproductive to the overall goal of improving the soldier's extensor lag.
A final limitation to the report is the fact that the soldier sustained extensive soft tissue damage as a result of imbedded shrapnel, which included bone loss that required a graft. Perhaps the serious nature of the injury may not have lent itself to full recovery of the extensor lag. The soldier may have sustained bone shortening, tendon lengthening and muscle (interossei) damage that would have limited full recovery of the extensor lag. 4
Conclusions
The authors of the case report are aware that four weeks of treatment may not be enough time to accurately assess the benefits of all of the treatment components utilized. The report provides therapists with information about another technique that could potentially be used in conjunction with other treatments in effectively treating stable MCF and proximal phalanx fractures that present with an active extensor lag at the MCP and PIP joints. Since these results are case specific, perhaps future research studies could determine if the TETA alone would be an appropriate component of a rehabilitation protocol for patients with stable MCF and proximal phalanx fractures.
Footnotes
Acknowledgements
The authors received written permission from the soldier to discuss and submit the case for publication and presentation. This paper is an adaptation from the case report section at the American Society of Hand Therapists Annual Meeting (Boston, October 2008).
Competing interests
None declared.