
Abstract
Introduction
Circumferential measurements (CMs) are used by hand therapists to monitor digital oedema. There are a range of tape measures available commercially to measure digital circumference, but none of them have any data to support their reliability or validity.
Method
Observational measurement studies using a repeated measures design were undertaken to assess if a weighted tape measure, used with a protocol, could provide accurate and reliable CMs of swollen digits.
In study 1, validity and responsiveness were determined by two raters measuring 16 steel bars of known circumferences and comparing the known measurements to those taken with the weighted tape. In study 2, intra- and inter-rater reliability was assessed by three raters measuring 12 prosthetic digits. In study 3, 27 swollen digits were measured by three raters to assess intra- and inter-rater reliability of the raters using the weighted tape in a clinical setting. The analysis of validity was based on the Bland–Altman plots. Reliability was based on the intraclass correlation coefficient (ICC).
Results
There was near-perfect agreement between the measurements taken by two assessors at the start and end of the trial and the actual circumference of the steel bars (all mean differences <1 mm). A minimum change in circumference of 2 mm could be detected with the same rater and a change of 3 mm could be detected with a different rater. On swollen digits the ICC values were significantly greater than 0.9 for both inter- and intrarater reliability. The lowest values for inter-rater reliability were ICC 0.983 (0.965–0.992) and for intrarater reliability were ICC 0.978 (0.954–0.990).
Discussion
The weighted tape measure has been shown to be valid and reliable in this study when used with a protocol for measuring swollen digits. It was easy to use and may become a clinically useful tool.
Introduction
In an age of accountability the need for objectivity when carrying out a comprehensive hand assessment should be fundamental to hand therapy.
Without objective markers to refer to, an assessment of patient status and progression is severely limited; meaningful professional communication and the ability to undertake research requires valid and reliable outcome measurements. In her 1986 publication, Fess 1 stressed the need for therapists to ‘become more sophisticated in our demands for better assessment instruments’. Therapists should be using objective markers but also must ensure that the tools they use are both valid and reliable for clinical decision-making and in research. A valid tool is one that measures consistently the phenomenon for which it was designed, e.g. circumference, strength and volume. 1,2 A reliable tool is one that has demonstrated statistically it can measure consistently between sessions, examiners and instruments and is assessed by the intra- and inter-rater reliability. 1,3,4 Intrarater reliability shows agreement between successive measures from a single rater, while inter-rater reliability shows agreement between different raters at the same time. 3 The intraclass correlation coefficient (ICC) has been used for assessing the intra- and inter-rater reliability and it reflects both the association and agreement of ratings. 5–8 ICC values range from 0 to 1 and values of 0.90 and above suggest excellent agreement, between 0.75 and 0.89 moderate agreement and below 0.75 poor agreement. Reliability coefficients of 1 are rare, as no tool is perfect; so reliability is a property that is attained to varying degrees. 8 Another important characteristic of a tool is responsiveness, defined by Beaton et al. 9 as the ability of an instrument to detect accurately a change when it has occurred. This allows the clinician to differentiate between what is a real change rather than variability due to measurement error or the nature of the phenomenon being measured; hence, the responsiveness of an assessment tool is a context-specific attribute.
The presence of digital oedema in patients attending for hand therapy is of significance to the treating clinician. The potential complications of prolonged oedema are pain, stiffness and joint contractures. 10 The American Association of Hand Therapists recommends the use of the hand volumeter for the assessment of oedema. 11 The volumeter has been both praised 12,13 and criticized 14–16 for its level of validity and reliability. In terms of usability there are drawbacks of using this method of assessment: it requires bulky specialist equipment, a water source, the exclusion of patients who cannot immerse the limb up to the forearm and the inability to assess digits in isolation. The alternative to measuring hand volume in the clinic is to measure digital circumference using a tape measure. Here each digit can be assessed independently and without the use of expensive specialist equipment. However, circumferential measures have also been criticized for variability in the tension used to tighten the tape around the digit. 17–19 From the authors' clinical experience of using a fabric tape measure or Jobst tape™ to assess digital oedema, the following problems have been noted: inconsistency in tape placement and replacement, inability to achieve a snug fit around a joint in slight flexion, differing quality of tapes, e.g. paper tapes are frequently used but should not be re-used as they tear and stretch and potential inaccuracies in reading the scale.
In 1988 Palmada et al. 14 reported the need for more precise laboratory type methods to be employed by therapists in their assessment of oedema. In our study a weighted tape measure (registered design 4010150) along with a protocol of use was designed in an attempt to try and meet the demands for a tool that is both accurate and reliable but still readily accessible and easy to use by all clinicians whatever their level of experience. Currently there is only one prototype weighted tape measure, which was used for this research study. The design is registered with the UK patent office and thus protected from being copied. Anyone wishing to use it must contact the first author or the Hand Unit for permission to borrow the equipment.
Methods
Study design
A series of studies using a repeated measures design were undertaken to examine the validity, responsiveness and reliability of the weighted tape measure. The Derby Hospitals NHS Foundation Trust Research and Development Department and the Derbyshire Research Ethics Committee approved the study (LREC reference: 06/Q2401/59).
Description of the weighted tape equipment
The weighted tape is a length of tape that can be looped around a digit and instead of manually pulling the tape to tension it around the digit, a small weight attached to the end of the tape provides a standardized amount of tension. The tape itself is made of 0.5 cm wide non-stretch fabric. It was hoped that this slim tape would aid conformity around the digits, especially around flexed proximal interphalangeal joint (PIPJ). The tape was mounted in a small metal frame that includes a scale in millimetres and a Perspex reading plate that aids accurate reading of the scale by minimizing parallax error.
A small weight of 10 g was chosen to provide the standardized tension to the tape. This weight was selected, as it was great enough to overcome the friction of the tape moving in the frame, but small enough not to cause visible compression of a digit. The metal frame can be stood upright in a wooden base unit (Figure 1). The protocol for use can be obtained by contacting the corresponding author.
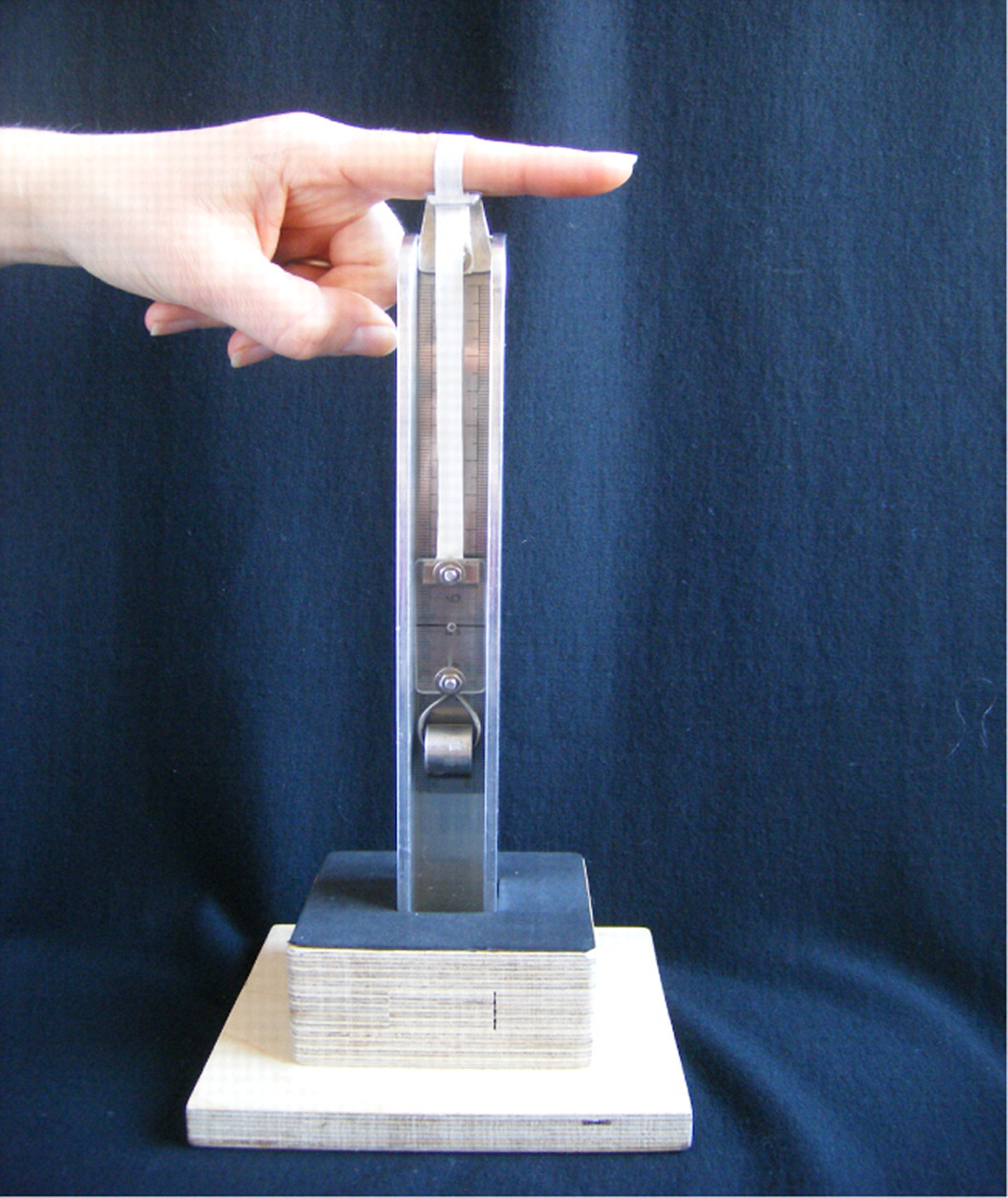
Weighted tape and stand
Study 1: Validity and responsiveness
The objective was to determine the validity and responsiveness of the weighted tape when measuring cylinders of a known, fixed circumference.
Using inert objects of known fixed circumference eliminated possible variability in measurements due to physiologically mediated changes as could occur in a human sample.
Sixteen ground steel bars were fabricated with specific calibrated circumferences varying from 31–94 mm. This range was selected to represent a range of adult digit circumferences.
Two raters participated in this study, one physiotherapist with over 16 years experience treating hand patients and one occupational therapist with over five years experience. The two raters were randomly selected from 14 available professionals in the Hand Unit using random tables. All the raters in the three studies had time to read the protocol and 10 minutes to practise with the tool before taking their measurements.
The investigator clamped each bar in random order and each rater measured the bars once using the weighted tape according to the protocol of use. The bar order was randomized in blocks of 16 to ensure no memory of the previous readings by the raters using NQuery Advisor software.
The raters were blinded to the actual circumference of the bars and to each others' readings. When study 3 was complete, study 1 was repeated by the same investigator and raters. This repeat measure at the end of study 3 was carried out to provide information on the validity of the weighted tape over time (19 months) and after repeated use.
The statistical analysis was performed with the Statistical Package for the Social Sciences, SPSS version 17.0 for Windows. The distribution of the continuous variables was tested using their histograms. The results for the skewed variables were presented as median (interquartile range) and for those following a normal distribution as mean (±standard deviation). 5
Bland–Altman plots were used for testing the validity of the tool for measuring the actual circumference of the steel bars.
4,5
The mean (±standard deviation) of the difference between the raters' measurements and the actual circumferences of the steel bars was presented. The responsiveness of the tool was calculated using a formula by Waylett and Selby
13
(
A sample size of 16 steel bars was calculated based on 95% confidence interval (CI) of the expected ICC of 0.98. The lowest acceptable limit of agreement was set high to 0.95 in this study, as the tool was compared with straight steel bars with standard circumference and it was expected to measure very accurately.
Results
The mean difference between the known circumference of the bars and that measured by two raters at both time points, pre- and poststudies 2 and 3, was less than 1 mm (Table 1). For all the measurements the difference between the raters' measurement and the known circumference of the steel bars was within the limits of agreement (Figures 2 –5). This indicates the tape measure and the protocol for use provided accurate measurements on inert objects throughout the study time period (19 months) and that this level of validity was achieved by more than one rater.
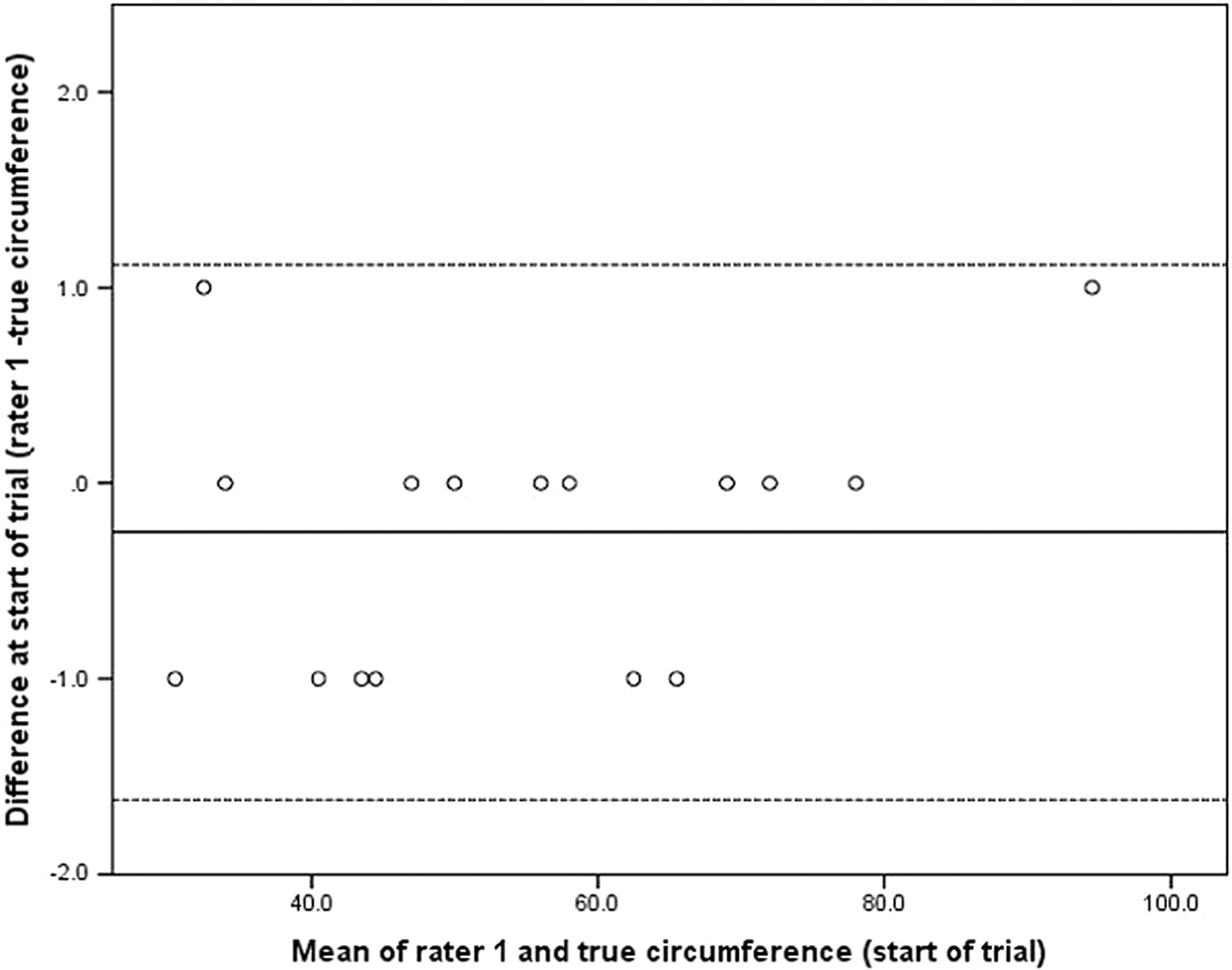
Bland–Altman plot to illustrate the differences of first assessor's measurements against the true circumferences of the steel bars at the start of the trial. 100% of the differences fell within the limits of agreement, indicating excellent accuracy of the tool. Solid line: the mean difference of first assessor's measurements against the true circumferences (−0.25); dashed line: the limits of agreement (−1.61, 1.11)
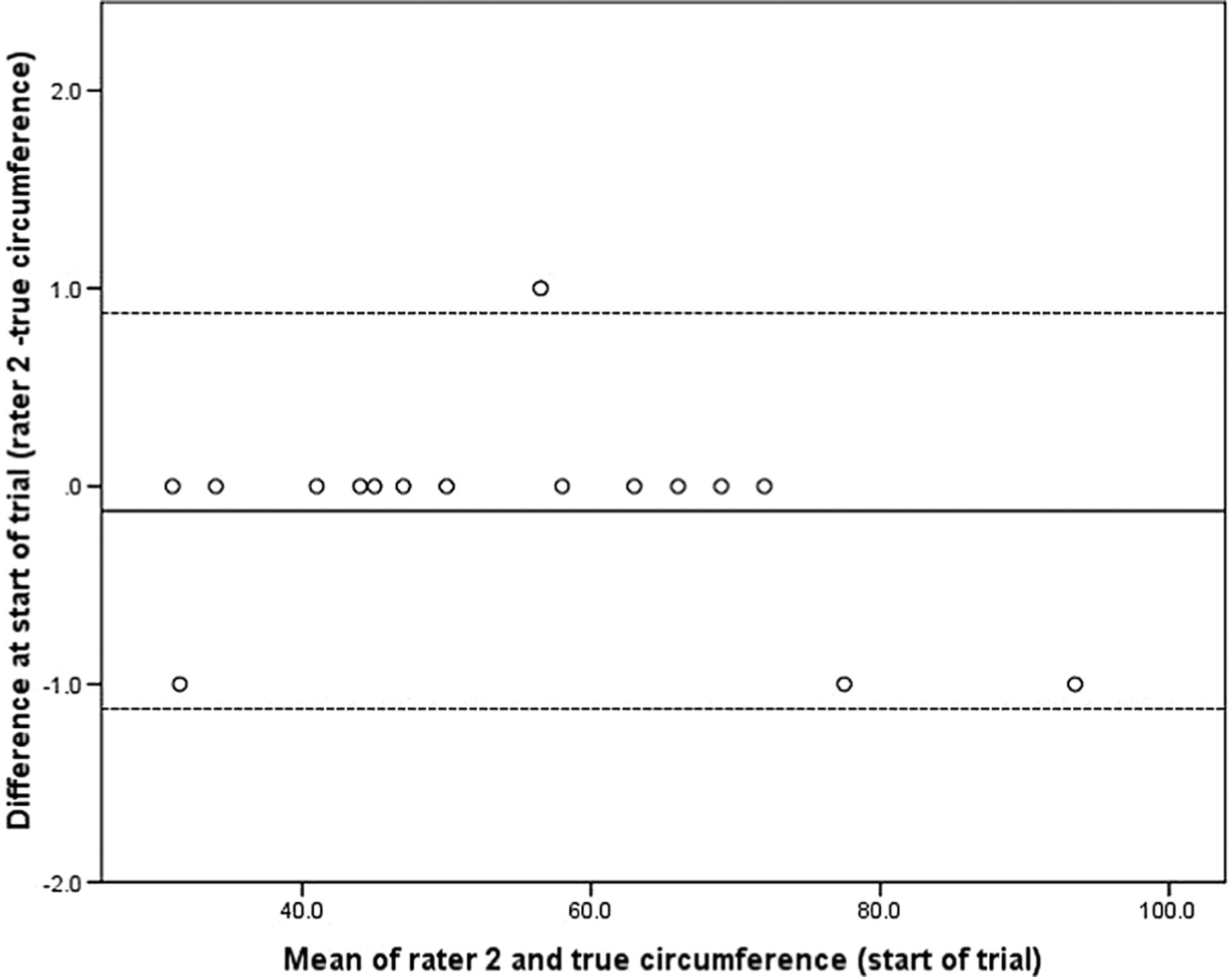
Bland–Altman plot to illustrate the differences of second assessor's measurements against the true circumferences of the steel bars at the start of the trial. 94% of the differences fell within the limits of agreement, indicating excellent accuracy of the tool. Solid line: the mean difference of second assessor's measurements against the true circumferences (−0.125); dashed line: the limits of agreement (−1.125, 0.875)
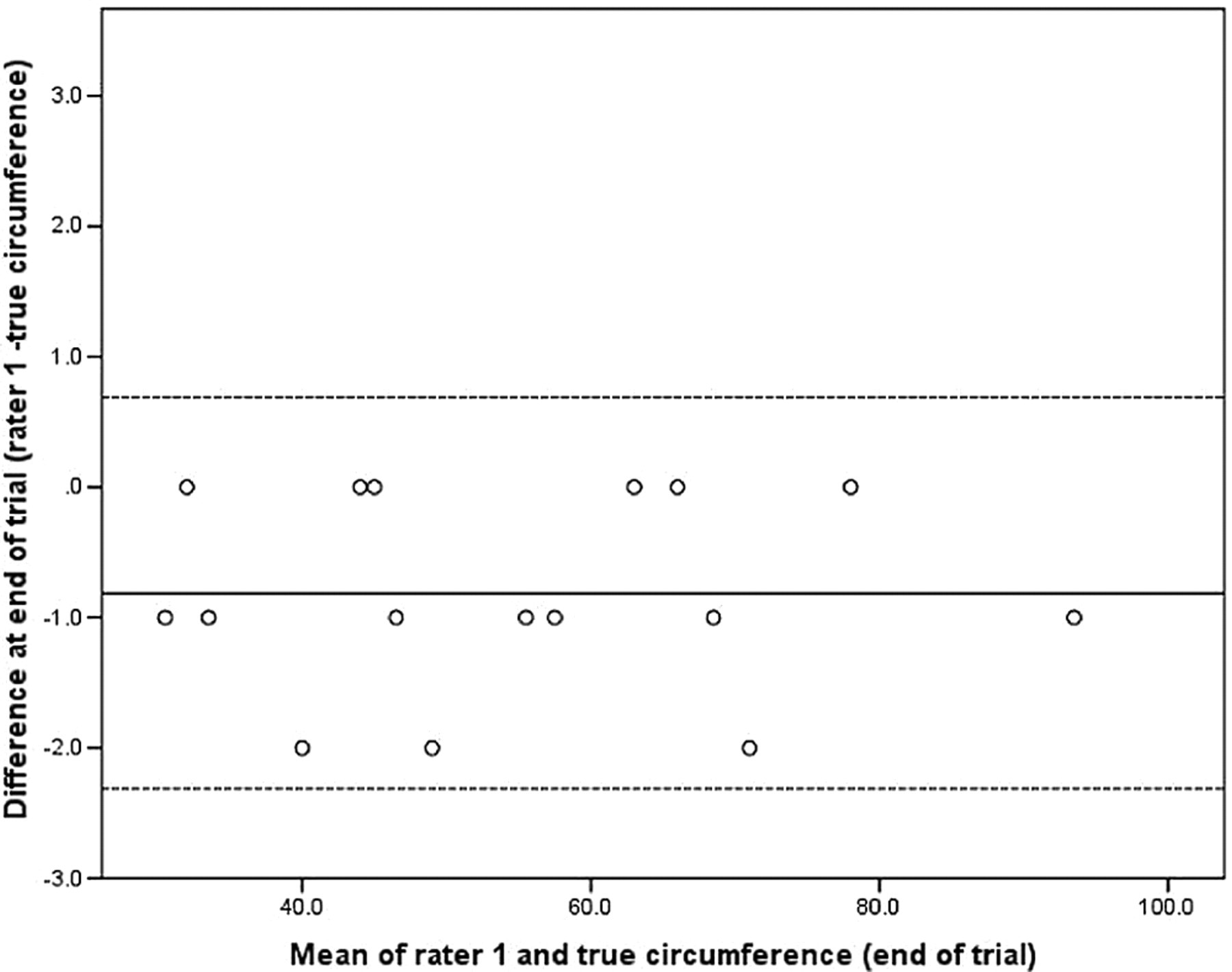
Bland–Altman plot to illustrate the differences of first assessor's measurements against the true circumferences of the steel bars at the end of the trial. 100% of the differences fell within the limits of agreement, indicating excellent accuracy of the tool. Solid line: the mean difference of first assessor's measurements against the true circumferences (−0.813); dashed line: the limits of agreement (−2.31, 0.68)
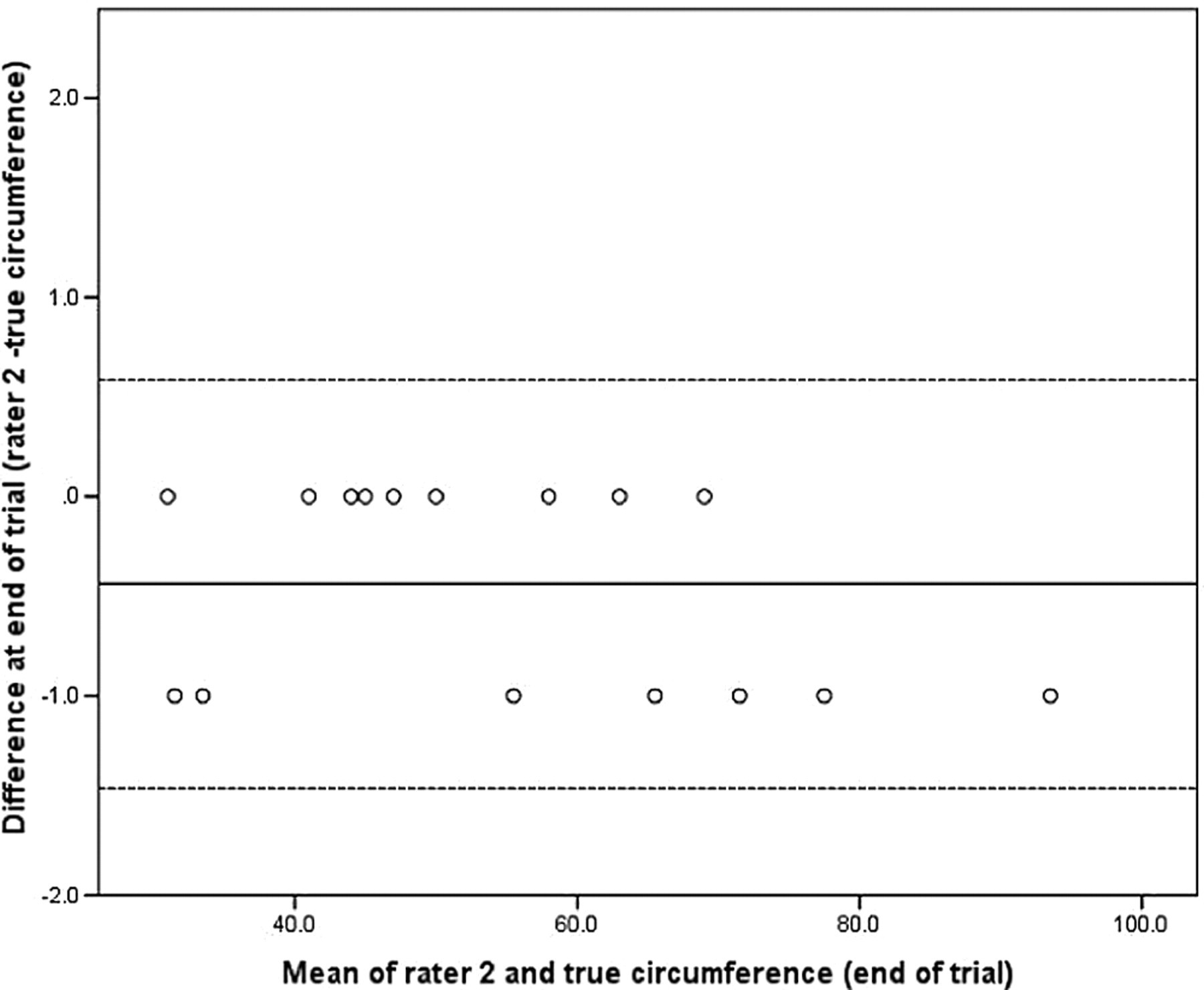
Bland–Altman plot to illustrate the differences of second assessor's measurements against the true circumferences of the steel bars at the end of the trial. 100% of the differences fell within the limits of agreement, indicating excellent accuracy of the tool. Solid line: the mean difference of second assessor's measurements against the true circumferences (−0.438); dashed line: the limits of agreement (−1.463, 0.586)
Results of mean of difference (mm) between the raters' measurements and the actual circumferences of the steel bars
SD, standard deviation
The responsiveness analysis showed the weighted tape is responsive for measuring a change in circumference of 2 mm with the same rater measuring and 3 mm with a different rater measuring.
Study 2: Intra- and inter-rater reliability on prosthetic digits
The objective was to determine the intra- and inter-rater reliability of the weighted tape when measuring prosthetic digits by three raters with different years of professional experience and to update the protocol for use.
Unlike the metal bars the prosthetic digits were not of uniform circumference along their length and thus this phase introduced the need for accurate tape placement and assessed the ability of the tape to conform. It was hoped that any problems with the weighted tape itself or the protocol for use would be highlighted so that any necessary changes could be made prior to the enrolment of patients (study 3).
Twelve prosthetic digits were cast from volunteers (men and women) with no history of recent hand trauma, their ages ranged from 4 to 84 years. The digits were cast in relaxed extension of the PIPJ (varying in range from 6° to 20° of flexion) and all digit types were represented at least once.
Three raters participated in this study, randomly selected based on random tables from 14 available professionals who had been grouped by years of experience in hand therapy (less than 1 year, 1–5 years, more than 5 years). Two were physiotherapists, one with 13 years and one with nine months of experience in hand therapy, and one was an occupational therapist with five years of experience in hand therapy.
The prosthetic digits were marked up by the investigator on the volar surface and a tape then looped around the digit to mark dorsally and laterally (using a standard tape measure) volar markings as described:
Proximal phalanx (P1) – midway between the distal crease of the metacarpophalangeal joint (MCP) and the proximal crease of the PIPJ. PIPJ – centre of the joint. Middle phalanx (P2) – midway between the most proximal flexion crease of the PIPJ and the distal interphalangeal joint.
Each digit was measured twice by each rater in a single session and in random order. The order of the 12 digits was randomized in blocks of 12 using NQuery Advisor software. The digits were held by the investigator while the rater measured each of the three marked locations. The raters were blinded to each others' results.
Prior to progressing onto study 3, the raters were then asked to complete a questionnaire (available on request) regarding the tape measure and protocol for use, for example ease of use, problems encountered, time required to practise and perceived clinical usefulness.
The single measures ICC and 95% CI were used for the analysis of intra- and inter-rater reliability as the individual circumference measures were used (studies 2 and 3). 5–7 A one-way random effects model was used for estimating the intrarater ICC as one rater has taken two measurements on all the available digits (studies 2 and 3). 5,6 The two-way random effects model was used for estimating the inter-rater ICC as a random sample of three raters is selected and each rater measured each digit (studies 2 and 3). 5,7 The estimated ICC was compared with the lower ICC limit using the Z-test for proportions so as to test that the reliability is significantly higher than the lower acceptable limit of agreement we set in each study. The significance was set at P < 0.05.
In this second study the weighted tape was used in prosthetic digits that had some flexion and were expected to have higher variability within the measurements compared with study 1. Therefore, we set the lower acceptable limit to 0.85. A sample size of 12 prosthetic digits was calculated based on ICC of 0.95.
Results
There was slightly more variation in the measurements than seen when measuring steel bars, but the agreement (ICC) in measurements was significantly higher than the lower limit of acceptability 0.85, indicating good intra- and inter-rater reliability for using the weighted tape on prosthetic digits (Tables 2 and 3). There were also similar ICC scores for all the raters indicating profession and years of experience in hand therapy had no influence on ability to use the weighted tape.
Results of ICC and 95% CI for intrarater reliability of three raters measuring prosthetic digits
ICC, intraclass correlation coefficient; CI, confidence interval
*Comparison of ICC versus the lower limit of 0.85
Results of ICC and 95% CI for inter-rater reliability of three raters measuring prosthetic digits
ICC, intraclass correlation coefficient; CI, confidence interval
*Comparison of ICC versus the lower limit of 0.85
From the results of the questionnaire, the raters all felt confident to use the weighted tape after reading the protocol and practising with it for 10 minutes.
However, the following changes were implemented to improve its ease of use for study 3:
The line on the perspex reading plate was darkened to make reading the scale easier. Rather than the rater trying to hold the tool steady while taking a measurement, the tool was placed in its wooden base unit so it was fixed allowing the therapist greater freedom of movement. To accommodate digits with severe flexion contractures an alternative subject position was added to the protocol. The subject's forearm could be positioned in mid-prone and the MCP joint flexed allowing access to the digit and enabling the tape to be positioned vertical to the middle phalanx. This was not possible in the fully pronated position when PIPJ were severely flexed.
Study 3: Intra- and inter-rater reliability on patient's oedematous digits
The objective was to determine the intra- and inter-rater reliability of the weighted tape and protocol for use when measuring oedematous digits.
The same raters for study 2 participated in study 3. Hand therapists working in the Derby Hospitals NHS Foundation Trust, Pulvertaft Hand Unit invited patients to take part based on the study inclusion and exclusion criteria (Box 1). Written informed consent was obtained by one of the researchers. Sixteen patients with 27 oedematous digits were measured by the three raters. There were six men and 10 women, whose ages ranged 27–74 years with a mean of 52 (±13.47) years.
Inclusion and exclusion criteria for study 3
Inclusion criteria
Visible swelling along the proximal and middle phalanx of the digit as assessed by their treating physiotherapist.
Patients whose wounds have healed and they are permitted to wash the hand.
Patients who are able to give informed voluntary consent.
Patient willing to allow non-permanent pen marks to be made on the finger.
Adult patients only, i.e. 16 years or over at the time of consenting to take part in the study.
Exclusion criteria
Open wounds or scabbed areas on proximal or middle phalanx.
Inability to understand written and verbal English for informed consent.
Unstable fractures or ligament injuries, tendon repairs, etc. that need constant splintage, making the digit inaccessible.
All digit types were measured, and there was an even distribution between them (5 thumb, 6 index, 6 middle, 4 ring and 4 little fingers). Thirteen digits (48%) were measured at the subacute (taken as 2–8 weeks from onset) and 13 (48%) at chronic stage (beyond 8 weeks) with only one measured in the acute inflammatory stage of healing.
The patients presented with a range of injuries and conditions causing increased finger size and oedema. As well as trauma (wrist and digit fractures, 15 digits) and surgery (6 digits), there were three digits each from hands with chronic regional pain syndrome and brachial plexus injury. There was equal spread of digits from dominant (48.1%) and non-dominant (51.9%) hand. The degree of active extension of the PIPJ/IPJ is shown in Figure 6 and represents a good spread of measurements from hyperextension (mainly thumb IPJs) to significant fixed flexion deformity of −52°. This enables us to establish if a fixed flexion deformity at the IPJ would affect reliability of circumferential measurements at the joint. Each digit was taken as an independent observation even if it was a second digit measured in the same hand. This is because clinically each digit has a different challenge for the rater varying joint extension at the PIPJ, ring and middle fingers being harder to access the P1 if finger abduction is limited and a fixed flexion deformity dictating the digit should be measured with the forearm in neutral rather than pronation.
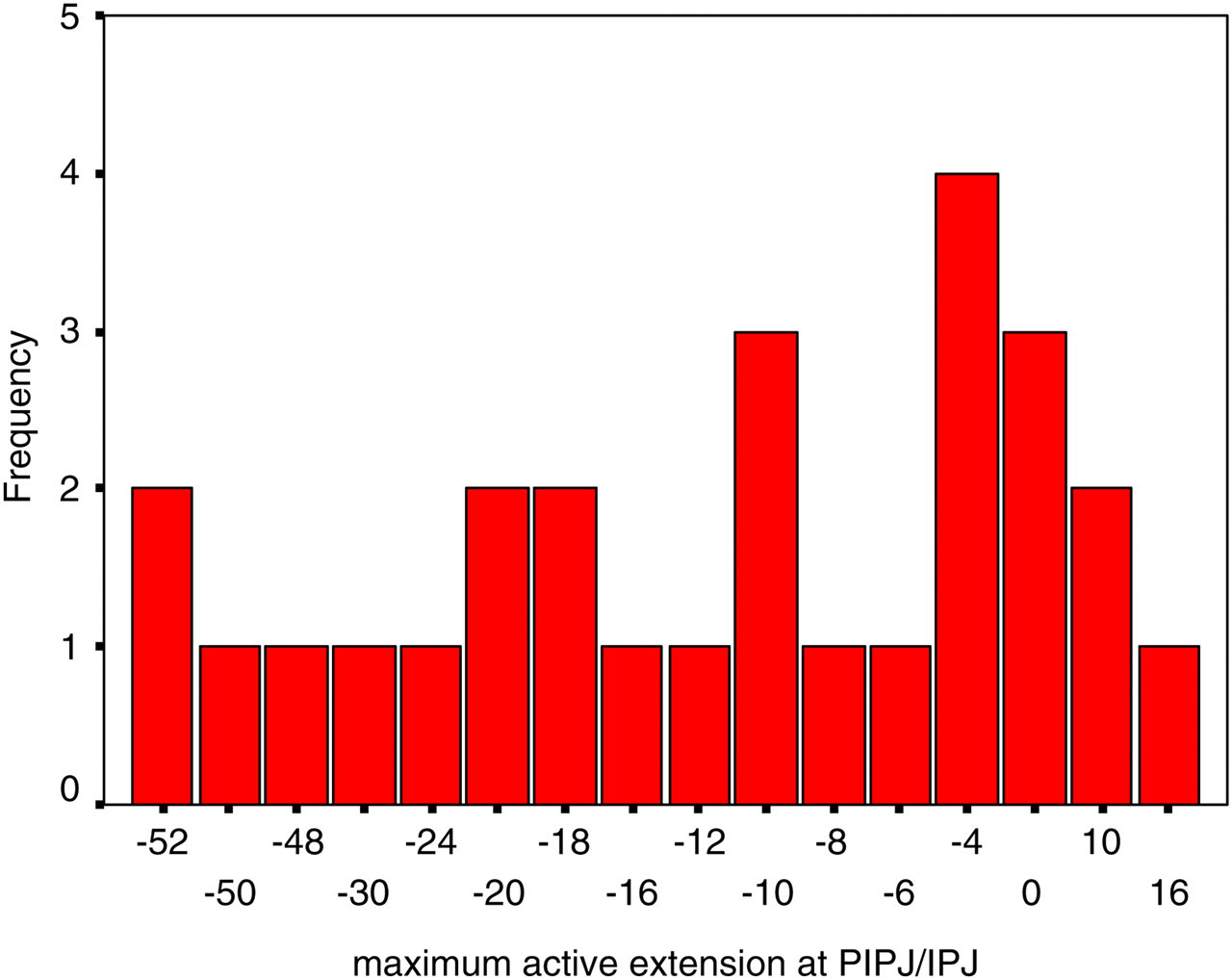
Distribution of the degree of maximum extension of the proximal interphalangeal joint/interphalangeal joint (thumb) in the oedematous digits
The same statistical methods as for study 2 were used in study 3. The 27 digits were taken as independent observations even if they were measured in the same hand.
In this study, the lower acceptable limit was set at 0.9 as more variability was expected compared with study 1 but a higher limit than in study 2 would be preferable for clinical use. A sample size of at least 24 digits was calculated based on an ICC of 0.95.
The investigator interviewed each patient and obtained details of cause and onset of the oedema. The digit to be measured was assessed and recorded for PIPJ flexion contracture using a goniometer. The digit was then marked up as described for study 2.
The order in which the three raters measured each digit was randomized so that the same therapist was neither first nor last to measure every time using simple randomization by digit. Each rater in turn was asked to measure each location on the digit once and call out their measurements, which were recorded by the investigator. The same rater then repeated the measurements and it was hoped that this would minimize the rater's ability to remember their previous measurement for the same location and thus influence the reading of the scale. The raters were blinded to each other's results.
Results
The measurements taken showed digits ranged in circumference from 31 to 94 mm (median for P1 = 65 mm [60–76], for PIP = 62 [59–70] and for P2 = 54 [51–60]).
The ICC values for all three raters at each of the locations measured was significantly higher than the lower limit of 0.9, with narrow 95% CIs showing that on swollen digits regardless of the degree of flexion of PIPJ (up to −52°) the tool and method of use had excellent intrarater reliability, achieving 0.99 is nearly perfect reliability (Table 4). There was also no relationship between years of hand therapy experience and intrarater reliability.
Results of intrarater reliability of the raters on swollen digits
ICC, intraclass correlation coefficient; CI, confidence interval; PIPJ, proximal interphalangeal joint
*P value <0.001 versus the lower ICC limit of 0.90
The inter-rater reliability at each location measured on the swollen digits was estimated separately for the first and the second reading (Table 5). The ICC for all the locations after the first and second reading was significantly greater than 0.9, indicating excellent inter-rater reliability when using the tool and the protocol for use, on oedematous digits at the proximal phalanx, PIPJ and middle phalanx. For the proximal phalanx and the PIPJ, the ICC was slightly higher and the 95% CI narrower for the second reading compared with the first, indicating slightly greater reliability and hence a benefit in using a second reading. The order in which the raters took the measurements had no effect on reliability (ICC).
Results of inter-rater reliability for all raters on oedematous digits
ICC, intraclass correlation coefficient; CI, confidence interval; PIPJ, proximal interphalangeal joint
First and second measurements are separated
*Comparison of ICC versus the lower limit of 0.90
Discussion
The weighted tape is a new tool devised to address the problems of measuring the circumference of digits. As with all measurement tools it relies (for validity and reliability) on the person using the tool to be familiar with it and to follow a protocol. Answers to the questionnaire showed our raters all felt confident with the weighted tape measure and, as such, it should be easy for any clinician to use.
To meet infection control standards the tape was wiped clean with alcohol wipes between patients. After a period of time this had the effect of causing the tape to run less smoothly through the metal loop, presumably because the coating on the tape was being removed. Although it felt to the raters that this may affect the tension exerted by the weight there was no change in reliability (measures taken on patients) or validity (measures taken on steel bars) in the latter part of the study.
The raters performed two measurements per location (e.g. PIPJ) for testing the intrarater reliability in each location. The difference in first and second reading for inter-rater reliability is small, but it is apparent that the second reading taken was more reliable for all the raters. This may have been due to the rater becoming more confident with how to position the tape; we would advise that two measurements in each location should be taken and the second measurement should be used for clinical decision-making.
The weighted tape has acceptable levels of validity in that it measures circumference accurately as shown by the measurements with the steel bars. However, the validity of circumferential measurements for oedema is open to question. The measurements do not reflect which part relates to normal tissue, interstitial fluid and which part is oedema. An increase in circumference could indicate increased oedema or bleeding or just diurnal variation; likewise a decrease in circumference of a digit may not indicate reduced oedema. The clinician must interpret their measurements with care; however, this would also hold true for the volumeter. The weighted tape can identify unevenly distributed oedema in the digit, which will not be apparent when using the volumeter; therefore, we suggest that swelling is measured in more than one location on a digit.
In this study the tool was shown to be valid (study 1) even if it was slightly underestimating the true circumference of the bars following the 19 months of use. This has probably happened because the raters were rounding down the measurements lying between two numbers the second time. Guidance has been added to the final protocol for use indicating for rounding up.
Limitations
In this study the subjects had their forearm supported; this was due to the length of time they had to remain static to allow three raters to perform all the measurements. Clinically it would be easier and quicker to use the weighted tape without the forearm support. The weighted tape was reliable when used with prosthetic digits, which were hand-held rather than placed in a clamp. Again the clinician would have to judge that the patient is able to keep the digit still while lightly resting it on the weighted tape.
The digits were marked up by an investigator and not by each individual rater; this may affect reliability for repeat measurements over time if there was variation in the marking up. It is believed that the protocol for marking the digits would limit this form of error. The tape was used on PIPJs with fixed flexion deformities of up to 52°; we cannot state measurements would be reliable for larger fixed flexion deformities (FFDs). It would be essential to be able to position the digit so that the tool was perpendicular to the part being measured and that the tape was in contact with the skin at all points.
Conclusions
In this study the weighted tape has been shown to be accurate in measuring the circumference of steel bars, and to be reliable when used with a protocol for measuring the circumference of prosthetic digits and oedematous digits on patients. It may become clinically useful to therapists, nurses or doctors who wish to monitor digit circumference.
Footnotes
Acknowledgements
The authors wish to thank Mr Bryan Ward for his ideas and help in making the weighted tape; Mr Steve Attfield for his practical assistance; and Sue Kennedy, Anicia Baron and Marie Morgan for taking the measurements. The study was funded by The British Association of Hand Therapists Ltd (small projects award) and the Derby Hand Surgery Trust Fund.
Competing interests
None declared.