
Abstract
Introduction
The purpose of this study was to determine the extent to which individual digit strength measures correlate with overall hand strength, pain and function in persons with osteoarthritis (OA) of the hand, and thereby judge whether individual digit strength measures are relevant to the clinical assessment of hand disability in this population.
Methods
One hundred and four community-dwelling persons with OA of the dominant hand (84 women) participated in this cross-sectional study. Correlations between measures of hand strength (grip: digit and total; pinch: tripod, wide key and narrow key), dexterity and self-reported pain and function (subscales of the Patient-Rated Wrist and Hand Evaluation) were investigated.
Results
Although OA involved radial digits more than ulnar digits, radial digit strength contributes more to total grip (59% versus 41%). Correlations between total grip and digit strength varied from excellent (digits 3 and 4: r = 0.93 and 0.88, respectively) to moderate (digits 2 and 5: r = 0.75 and 0.74, respectively). Correlations between pinch and individual digit strength (digits 2 and 3) were moderate (r = 0.66–0.74). Correlations between measures of different constructs (strength, pain and physical function) did not exceed 0.41.
Conclusions
Individual digit strength is not linked with OA involvement of that digit. At most, strength of individual digits explains just over half of the variance in total grip strength and pinch strength. Assessment of individual digit grip strength appears to provide unique information regarding hand disability in persons with OA.
Introduction
Osteoarthritis (OA) of the hand is common and known to cause a decrease in hand strength that exceeds the age-related strength deficits. 1 Lower grip strength generally results in decreased hand function and many studies indicate that hand function is limited in persons with OA of the hand. 2,3 During grip, forces are primarily exerted at the proximal interphalangeal (PIP), metacarpophalangeal (MCP) and carpometacarpal (CMC) joints. 3–5 Clinical and radiological evaluation of the small joints of the dominant hand reveal that OA severity is greatest in the interphalangeal (IP) joints in the radial 3 digits. 6 In individuals without hand problems, strength of digits 2 and 3 makes a greater contribution to overall grip strength than digits 4 and 5. 7–9 It follows that OA involvement of the radial digits may have a greater impact on deficits in grip and pinch strength. Thus, hand function, and limitations thereof, may have a stronger association with strength of the index and middle fingers than other measures of hand strength.
Hand therapists traditionally measure hand grip and pinch strength using digital dynamometry. 10 The NK Digits-Grip device permits measurement of the flexor strength of individual digits in addition to overall grip strength. 7–9 Thus, individual finger strength is recorded during a multifinger task rather than during maximum voluntary contraction of individual finger flexor muscles. Although the maximum strength of each digit may be underestimated by this method (especially when the resistance is applied distal to the PIP joints), 11 the NK Digits-Grip device could provide a measure of functional strength of each digit.
This method of digital dynamometry has been used previously to show that the ratio of radial and ulnar digit strength to overall grip strength is approximately 60:40 in persons without hand pathology. 7–9 Only one publication reported the actual force values for the individual digits and subjects were 46 healthy men between 20 and 39 years of age. 9 The percentage contribution of digital strength to overall grip strength in persons with hand OA and whether OA involvement in the joints of a finger is related to digit strength is not known since this has not been investigated to date.
Purpose of the study
The purpose of this study was to determine the extent to which individual digit strength measures correlate with overall hand strength, function and pain in persons with OA of the hand, and thereby judge whether individual digit strength measures are relevant to the clinical assessment and rehabilitation of OA-related hand disability. Specifically, we address the following research questions:
What is the relative contribution of strength of digits 2–5 to total grip strength? What is the relationship of individual finger flexion strength to other measures of hand strength (total grip strength, tripod pinch and key pinch)? What is the relationship between OA involvement of individual digits and measures of hand strength (digit grip strength, total grip strength, tripod pinch, narrow and wide key pinch)? Which measures of hand strength are related to dexterity and self-report pain and function?
Methods
Participants
This cross-sectional cohort study was performed on 104 community-dwelling older adults who were recruited by poster and newspaper advertisements. Eligible subjects were 50 years or older and met the American College of Rheumatology clinical criteria for OA of the dominant hand. 12 Patients were excluded if they had co-morbid conditions such as neuromuscular disorders or other forms of arthritis affecting hand function, cognitive impairment and/or communication barriers that would impact performance in physical and self-report measures. Participants attended for testing on one occasion and received no compensation. The study protocol was approved by our institutional research ethics board, and all subjects provided written informed consent prior to participating in the study.
Measures
Strength of grip, individual digit flexion, tripod pinch, key (narrow and wide) pinch and dexterity were measured using components of the NK Hand Assessment System (NK Biotechnical, Minneapolis, MN, USA) and the corresponding standardized instructions. Strength of individual finger flexion and total grip were measured using the NK Digits-Grip device. The size of the grip on this device is similar to position 3 on the regular grip strength instrument of the NK apparatus (Figure 1A). Tripod pinch involves three fingers (thumb and digits 2 and 3) (Figure 1B). Key pinch involves positioning of the thumb on top and the radial side of digit 2 below. Narrow key was performed with the thumb and digit 2 spaced 12 mm apart (Figure 1C) and wide key with the thumb and digit 2 spaced 32 mm apart (Figure 1D). Dexterity of the dominant hand was assessed using the NK dexterity board and recorded as the time taken to manipulate small, and then large, objects. The average of three trials was the outcome measure for the strength and dexterity tests. Reliability of the standardized protocols has been established. 13–15

Grip and pinch strength instruments of the NK apparatus. (A) Digits-Grip device for measuring force produced by individual digits and total grip, (B) tripod pinch device, (C) key pinch device positioned to measure narrow key pinch force and (D) key pinch device positioned to measure wide key pinch force
The Patient-Rated Wrist and Hand Evaluation (PRWHE) was used to measure self-reported pain and disability. The PRWHE contains three subscales: a five-item pain scale, a six-item specific activities subscale (patient describes difficulty with specific tasks) and a four-item usual activities subscale (patient describes difficulty in four domains of daily life). All questions were rated on a 0–10 scale, where 10 represents higher pain or disability. High reliability has been confirmed for subscale scores, 16 and the subscales for pain and specific activities were used in this study. The items in each scale were added to produce a pain subscale score (maximum 50) and a disability subscale score (maximum 60).
Involvement of the small joints of the hand was determined by a physiotherapist (JW) based on the following clinical examination. The presence of pain, swelling, nodules and/or deformities was recorded for the MCP, PIP and distal interphalangeal (DIP) joints of digits 2–5 and IP, MCP and CMC joints of digit 1.
Analysis
Data were analysed using SPSS for Windows (version16, SPSS Inc, Chicago, IL, USA) and statistical significance was set at P < 0.05. Descriptive statistics for each variable were determined. The percentage contribution to total grip strength was calculated for each of digits 2–5 and differences in contribution were assessed using repeated measures analysis of variance. Reverse Helmert post hoc contrasts were used to determine differences between digits. Pearson correlation coefficients were used to determine the strength of associations between the various measures of dominant hand strength (digit grip strength, total grip strength, tripod pinch, narrow key pinch and wide key pinch) and between age, self-reported pain, self-reported disability, dexterity and each of the strength measures. Eta statistics were calculated to determine correlations between measures of strength and digit involvement (categorical data). For each digit, a 0 represented no pain, swelling, nodes or deformity and a 1 represented the presence of any of these signs or symptoms. Correlational analyses were used to determine which measures of hand strength best relate to dexterity and self-reported pain and function. As a function of the sample size, all correlation coefficients >0.20 were statistically significant (P > 0.05). For interpretation of the strength of the correlations, we considered the sample size and types of variables being studied when using the guideline suggested by Portney: |0 to 0.25| = little or no relationship; |0.25 to 0.50| = fair; |0.50 to 0.75| = moderate to good; and |0.75 to 1| = good to excellent. 17
Results
Table 1 summarizes the characteristics of the 104 participants (84 women). Women tended to be younger and shorter and have less hand strength. On average, women manipulated small objects more quickly than men, but the time required to manipulate large objects was similar for both genders. Self-reported pain and disability were similar. More women had involvement of digit 5, but most participants had involvement of digits 1–3 regardless of gender.
Summary of subjects' characteristics
SD, standard deviation; OA, osteoarthritis; IP, interphalangeal; MCP, metacarpophalangeal; CMC, carpometacarpal; DIP, distal interphalangeal; PIP, proximal interphalangeal; PRWHE, patient-rated wrist/hand evaluation
*n = 83 for height and weight only
Strength was greatest for digit 3 compared with the other digits and greater for the radial digits combined (digits 2 and 3) than for the ulnar digits combined (digits 4 and 5) (Table 1, P < 0.001). The greater contribution of radial digit strength to total grip strength is illustrated in Figure 2. With the exception of digits 2 and 4, the percentage contributions of the four digits were significantly different from each other (P < 0.001).
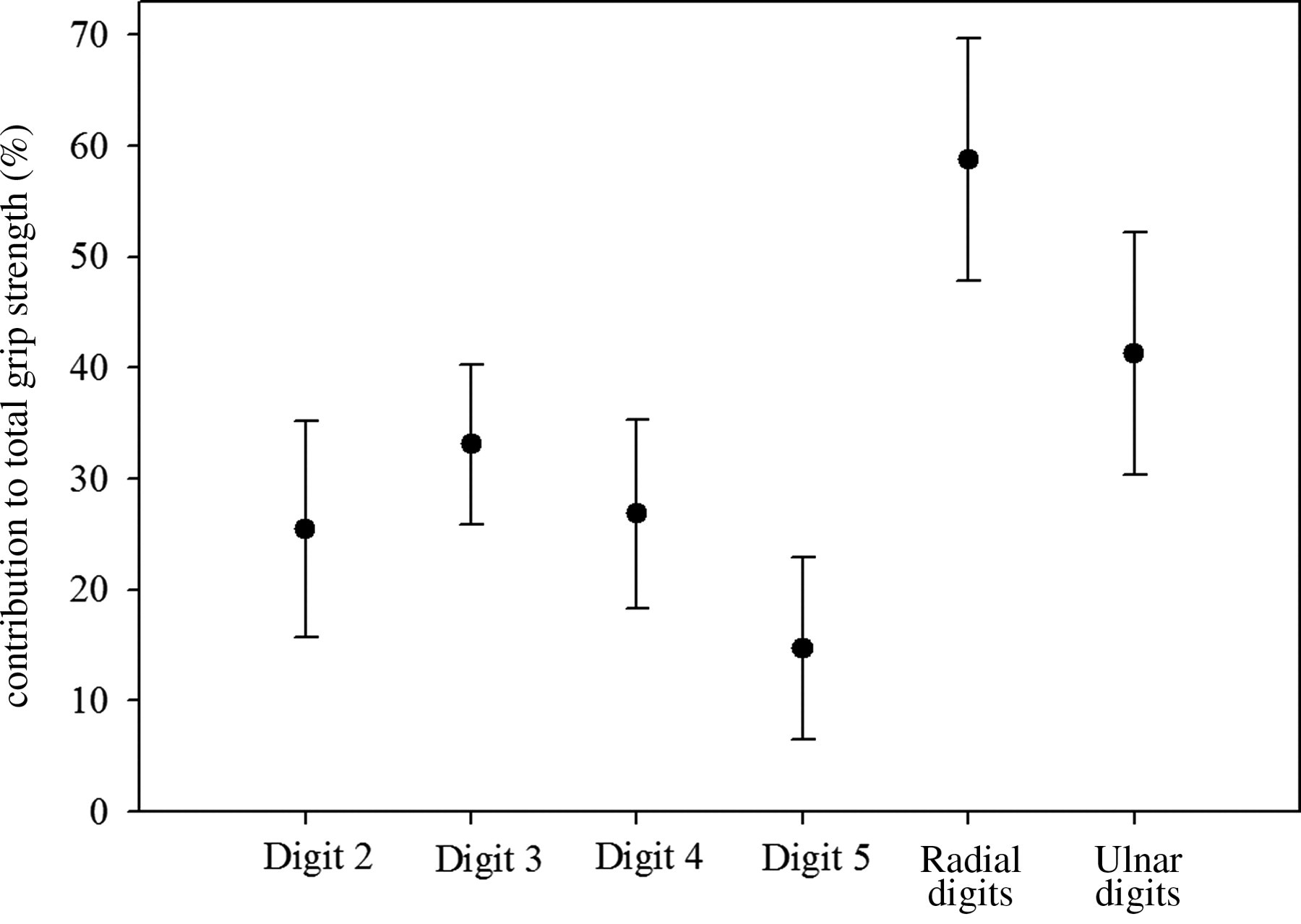
Ratio of grip strength of individual digits, digits 2 and 3 combined (radial digits) and digits 4 and 5 combined (ulnar digits) to total grip strength (%) in the dominant hand of 104 persons with hand osteoarthritis
As expected, moderate to excellent positive relationships were observed between measures of hand muscle strength (Table 2). Digital involvement did not have a clear impact on the distribution of digit strength since there were no significant associations between involvement of individual digits (2–5) and strength of individual digits or total grip (eta = −0.05 to 0.18, P > 0.05). In contrast, involvement of digit 1 was significantly correlated with all measures of strength (digit strength: eta = 0.20–0.26, P ≤ 0.05; grip: eta = 0.26, P < 0.01; pinch: eta = 0.24–0.28, P ≤ 0.01).
Relationship between measures of muscle strength in the OA hand
OA, osteoarthritis
The correlations between hand strength, age, pain, self-report disability and dexterity are presented in Table 3. Digit 2 and tripod pinch strength had a similar association with age (r = −0.22 and −0.24, respectively). Strength of digit 2, total grip and key pinch had similar associations with pain (r = −0.28 to −0.31). All measures of hand strength were related to dexterity with large objects (r = −0.25 to −0.37). With the exception of strength of digits 4 and 5, all strength measures were related to dexterity with small objects (r = −0.25 to −0.41). The same pattern was observed between strength and self-reported hand function, although the associations tended to be weak or non-significant (r ≤ −0.27).
Correlations (95% confidence intervals) between grip, pinch and digit strength and subject demographics, symptoms, function and dexterity
*P < 0.05
†PRWHE, Patient-Rated Wrist and Hand Evaluation questionnaire
Self-reported function (PRWHE-specific activities) explained less than 8% of the variance in performance-based function (dexterity with small and large objects, r = 0.28 and 0.24, respectively).
Discussion
This study is the first to demonstrate that, while grip strength in persons with hand OA is lower than age- and gender-matched normative values, the percentage contribution of individual digit strength to total grip strength is preserved. Despite the fact that our subjects had more OA involvement of their radial digits than their ulnar digits (Table 1), the percentage contribution to total grip strength of the radial and ulnar digits (59% and 41%, respectively) was remarkably similar to that previously reported for younger adults without hand pathology (61% and 39%, respectively). 7–9 The paper which reported mean values for individual digits tested healthy young men who had values 2–2.5 times higher than the 20 men in the present study. 9 Similarly, the magnitude of total grip strength in our volunteers was lower as compared with age- and gender-matched normative values. 18 However, values for total grip were similar to previous reports for men and women with OA of the hand. 2 The pattern of digit strength suggests global deficits in the force generated by the extrinsic and intrinsic finger flexor muscles 11 and do not appear to reflect inhibitory mechanisms arising from OA involvement in individual digits.
Measures of strength in individual digits (2–5) have moderate to excellent positive associations with total grip (0.74–0.93) and tripod pinch strength (0.56–0.74). However, the strength of digits 2 and 5 explain only 55% and 56% of the variance in total grip strength, respectively. Individuals with greater strength in total grip, tripod pinch and wide key pinch require less time to manipulate large objects with the strength of the association being comparable for all three strength measures (see confidence intervals in Table 3). Similarly, individuals with greater digit 2 and tripod pinch strength require less time to manipulate small objects. Pinch strength has the strongest association with self-reported pain and function. The very high correlation observed between measures of narrow and wide key pinch (r = 0.91) indicates that it is unnecessary to measure strength using both types of key pinch in individuals with hand OA. Taken together, our findings suggest that measurement of pinch strength (tripod and narrow or wide key) and individual digit strength provides unique information regarding hand function in persons with uncomplicated hand OA.
The presence of pain, swelling, nodes and/or deformity in specific fingers did not result in preferential loss of grip strength in those digits. Similarly, total grip strength and pinch (tripod and narrow and wide key) strength were not related to the presence of clinical features of OA in individual digits. In contrast, OA involvement of the thumb had a weak (but statistically significant) association with all measures of hand strength. As the most force during tripod pinch is on the CMC-I 5 and the thumb is required to stabilize the hand dynamometer during total grip strength testing, signs and symptoms in the thumb require particular attention in order to maximize strength in the OA hand. These results indicate that thumb involvement may be a limiting factor in production of force for patients with hand OA.
Limitations of our study must be considered when interpreting these results. One limitation is that we investigated the clinical utility of individual digit strength in persons with hand OA using a cross-sectional design, which permits only correlational analyses. Sensitivity to change and predictive validity of these strength measures were not investigated. A second limitation associated with testing muscle strength is the inability to confirm that the participants produce maximum force during their voluntary effort. We addressed this challenge by averaging three consistent trials for each measure of hand strength, which resulted in maximum grip forces that compare favourably with values previously reported for similar study participants. 2 A third limitation is that our study confirms the previously reported percentage contribution of digit strength to overall grip strength using the same method of assessment (Digits-Grip device). Previous work comparing digit force generated during isolated testing of that digit with the force generated in that digit during a four-finger task, suggests that using the Digit-Grip device to record individual digit strength in all four fingers simultaneously may underestimate individual finger force. 11 Finally, the construct of hand disability was evaluated using a single self-report measure and a single performance-based measure. The relations between hand strength and function reported in this study may not apply to different measure(s) of hand disability. Further research is needed to confirm our findings in longitudinal studies using a variety of methodologies available for measuring impairment, physical function and disability in persons with varying severity of hand OA.
The purpose of this study was to determine the extent to which individual digit strength measures correlate with overall hand strength in persons with OA of the hand, and thereby judge whether individual digit strength measures are relevant to the clinical assessment and rehabilitation of OA-related hand disability. Although persons with hand OA demonstrate generalized loss of hand strength, our findings suggest that assessment of individual digit strength (particularly digit 2) may provide useful information regarding functional status and effectiveness of strengthening exercises. The weak associations between physical impairment measures, self-reported function and performance-based measures of hand dexterity indicate that these tests provide different information and all should be included in a comprehensive assessment of persons with hand OA.
Footnotes
Acknowledgements
This study was funded in part by the Canadian Foundation for Innovation, NSERC, and the Evelyn Mackin Grant for Research in Hand Therapy from the American Society of Hand Therapists.
Competing interests
None declared.