
Abstract
Objective.
Longitudinal glide of the median nerve is affected in typical entrapment neuropathies such as carpal tunnel syndrome. The upper limb tension test one (ULTT1) is used by clinicians to assess patients’ responses to passive movements that affect the median nerve. ULTT1 is thought to mainly assess the longitudinal glide of the median nerve; however, transverse glide of the nerve at the wrist may be a more sensitive measure of an entrapment neuropathy.
Method.
Sixteen wrists of four male and 11 female healthy volunteers were studied with ultrasound imaging in this small original study. Images were collected in eight different combinations of shoulder, elbow and forearm posture. In each posture the wrist was moved from full flexion to 30° of extension.
Results
Nerve excursion from full wrist flexion to 30° of extension was mainly in a radio-dorsal direction. It ranged from a minimum of 1.8 mm (SD ± 2.0 mm) up to 3.57 mm (SD ± 1.86 mm) of transverse movement, and 0.22 mm (SD ± 0.59 mm) of volar movement to 0.96 mm (SD ± 0.76 mm) of dorsal movement. In all eight of the positions tested, forearm supination led to greater transverse movement of the nerve at the wrist.
Conclusions
Transverse movement of the median nerve is most marked with forearm supination, irrespective of other changes in the kinetic chain. The nerve moves dorsally in all movements except when the forearm flexors are off-loaded in elbow extension and elbow flexion. These findings confirm the transverse movement of the median nerve at the wrist, during active wrist extension within positions of the ULTT, but that the shoulder and elbow position have little impact on the degree of movement.
Introduction
For our bodies to move, the nervous system has to be able to accommodate the different postures into which we place our limbs. 1 Nerves must be able to slide and move within their beds and interface without compromising their own blood flow and nutrition. If they are repeatedly placed into a position that is close to the end of their normal physiological range, either tensioning or compressing them at a consistently high level, there may be adverse effects on this delicate haemodynamic position and the nerve will start to exhibit changes in its function.1, 2 Nerves usually glide in both a longitudinal and a transverse direction, but they always displace towards the area of highest tension in order to equal out the total nerve tension.1–4 This is a phenomenon called convergence, and can assist therapists as they assess the neurodynamic system and areas of possible entrapment. Elvey initially described an upper limb tension test (ULTT) for the upper limb nerves in 1983. 5 The test is a set of movements, which sequentially increases the tension or induces movement within the neural structures and their coverings. 6 The movement in the ULTT was explained as being a longitudinal glide of the nerve designed to pick up any sensitivity to movement within and around the nerve, when the passive sequential movements were performed.1,7,8 A more recent theory put forward is that the tests look at the relationship the neural structures have with their environment, and their mechanical and physiological functioning. 2 Kleinrensink et al. 9 assessed the original ULTT as described by Elvey in their cadaver study, and found this test was highly sensitive to the median nerve. The ULTT One (ULTT1) has been found to be the position in which the median nerve experiences the most mechano-sensitivity. 7 The ULTT1 is widely used within the clinical setting to diagnose neurodynamic problems relating to the median nerve, but it has been used on the premise that it affects the longitudinal gliding of the nerve.
Although the longitudinal glide of the median nerve is affected in typical entrapment neuropathies such as carpal tunnel syndrome, 10 or in non-specific arm pain, 11 the effect on the transverse glide of the nerve at the wrist may be a more sensitive measure of the extent and degree of an entrapment neuropathy. 12 Transverse gliding occurs when the nerve moves sideways out of the way of muscles and tendons, to decrease the total compression on the nerve at that point. In the wrist the median nerve moves in a transverse direction to avoid the flexor tendons during movement of the wrist, fingers and forearm.1,11,13 There has been little research into the transverse glide of the median nerve at the wrist when using positions of the ULTT1. This study assessed the impact of different positions of the ULTT on the transverse glide of the median nerve at the wrist in asymptomatic subjects to provide normative data, prior to further discussion or research relating to symptomatic populations.
Methods
Sixteen wrists of four male and 11 female participants were studied (one woman included both the right and left wrists), who had no history of neck problems, upper limb, shoulder, elbow or wrist pain, who had no carpal tunnel syndrome within the last year, and were not pregnant. Ethics approval was obtained from the Ethics Committee of University College London, London, as part of an MSc research project. Written informed consent was obtained from all participants. All candidates had a full range of motion and ability to perform the ULTT1. They were recruited via posters and requests within and around the authors MSc cohort and department, and friends. The participants were predominately women due to time constraints relating to the data capture and the MSc having a majority female intake.
Ultrasound images were captured at 50 frames using a Diasus ultrasound system (Dynamic Imaging, Livingston, Scotland, UK) with a 10–22 MHz, 26 mm array transducer, and three cineloops were collected in each position to gain an average excursion. This way of capturing data has been shown to be both reliable and effective in analysing median nerve movement.14–16 They were captured by the author and a colleague, both of whom were physiotherapists and not sonographers. The images were saved onto a personal computer, and were analysed offline as bitmap images using TPSDig2 software (F James Rohlf, Department of Ecology and Evolution, State University of New York, New York). The nerve coordinates were measured from frames taken at static five-frame intervals throughout the cineloop (50 frames), starting from the most useable frame (Appendix 1). For each position the subject was lying in a supine position with the head supported on a pillow and the shoulder girdle relaxed. Each subject was asked to keep their nose pointing at the ceiling during the data collection, and to keep the contralateral arm relaxed over the stomach. The subjects were asked to maintain this position during each test. Three measurements (cineloops) were taken in each position, on moving the wrist from full comfortable flexion to 30° of wrist extension. Four points were identified at the extreme upper, lower, right and left borders of the nerve by the author. This gave a single point that corresponded as closely as possible to the centre of the nerve. Owing to the software used, the author was able to state a start and end position of the nerve. The measured coordinates were put into an Excel spreadsheet and the average change (mm) in nerve position was calculated from the three cineloops. Only the motion of the nerve was analysed, although skin markers had been used to ensure the movement being measured was that of the nerve, and not movement of the skin under the transducer.
The transducer was held in position at the wrist using a custom-made support fitted to the transducer head. The support was positioned so that the distal edge was against the distal wrist crease. The support was held in place on the subjects’ wrist using adjustable straps. A piece of ‘stand-off’ sonogel was placed under the transducer to create a clearer picture on the image, as well as ultrasound gel being used to give the connection with the skin. A plastic splint was used to identify to the subjects how far they had to extend their wrists (30° and no further), and each subject started in full comfortable flexion of the wrist. The 90° flexion angle of the elbow was achieved using a bracket that was taped to the volar aspect of each subject's arm.
A standard goniometer was used by the same examiner to measure the glenohumeral joint at 10° of abduction (the neutral position) to ensure the edge of the couch was missed when moving into wrist extension, and 90° abduction. Each subject was placed into eight different positions (Table 1).
Positions of the ULTT1 used for data capture
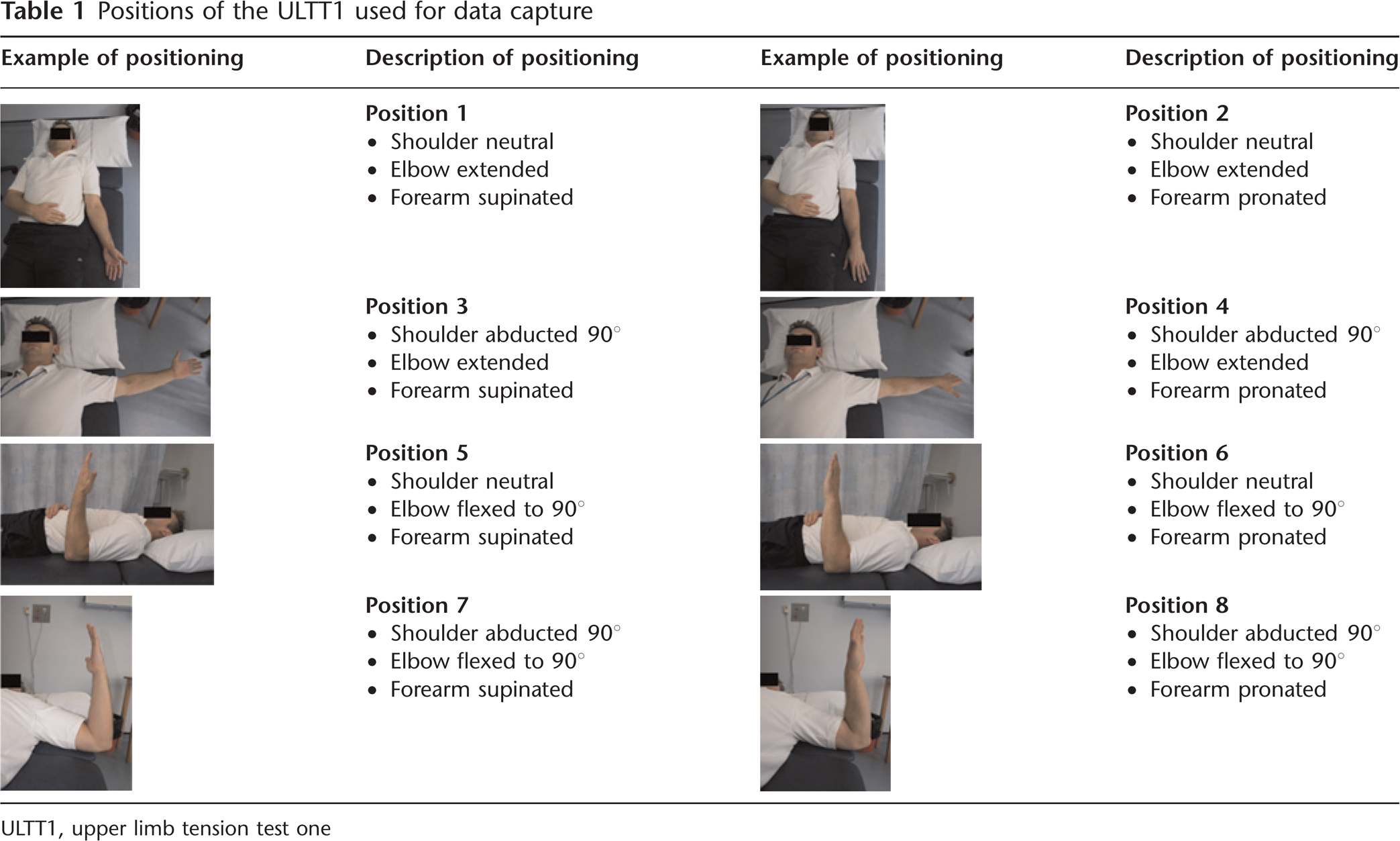
The wrist was moved slowly, over a count of three, with digit extension once the dorsal aspect of the hand was in contact with the splint. The subjects were asked to move the wrist slowly for two reasons: the first is that fast movements have been shown to increase the stiffness of nerves, and may decrease their excursion; 17 the second is to reduce the effects of a myostatic stretch reflex of the flexor muscles, 7 which can also affect the nerve excursion. Each subject was allowed a practice run in each new position if desired. They were asked to describe if there were any unusual feelings, or if the position was more/less comfortable than the previous ones. The non-dominant arm of each subject was assessed, with the exception of one subject who had both arms assessed.
Once the images had been analysed on the computer and a mean movement calculated for each movement from all the participants, a paired t-test was used to determine whether there was any significant differences between the movements (P = 0.05). A paired t-test was used as the cohort was being compared against itself, and data were assumed to be normally distributed. Each position was analysed against a second position just three times, and only two positions were compared together.
Results
Table 2 summarizes the radial and dorsal movement of the median nerve at the wrist in the eight different positions. A total of 16 wrists were assessed. In all ULTT1 positions, it was the addition of supination that produced most transverse movement of the median nerve at the wrist (Figure 1). When assessing the volar–dorsal movement of the nerve when the forearm was in a supinated position, the nerve moved dorsally in only one position (Figure 2).
Each ULTT1 position and subject, with the average nerve movement and direction, and the mean values with relevant standard deviations (SD) and standard error of the mean (SEM)
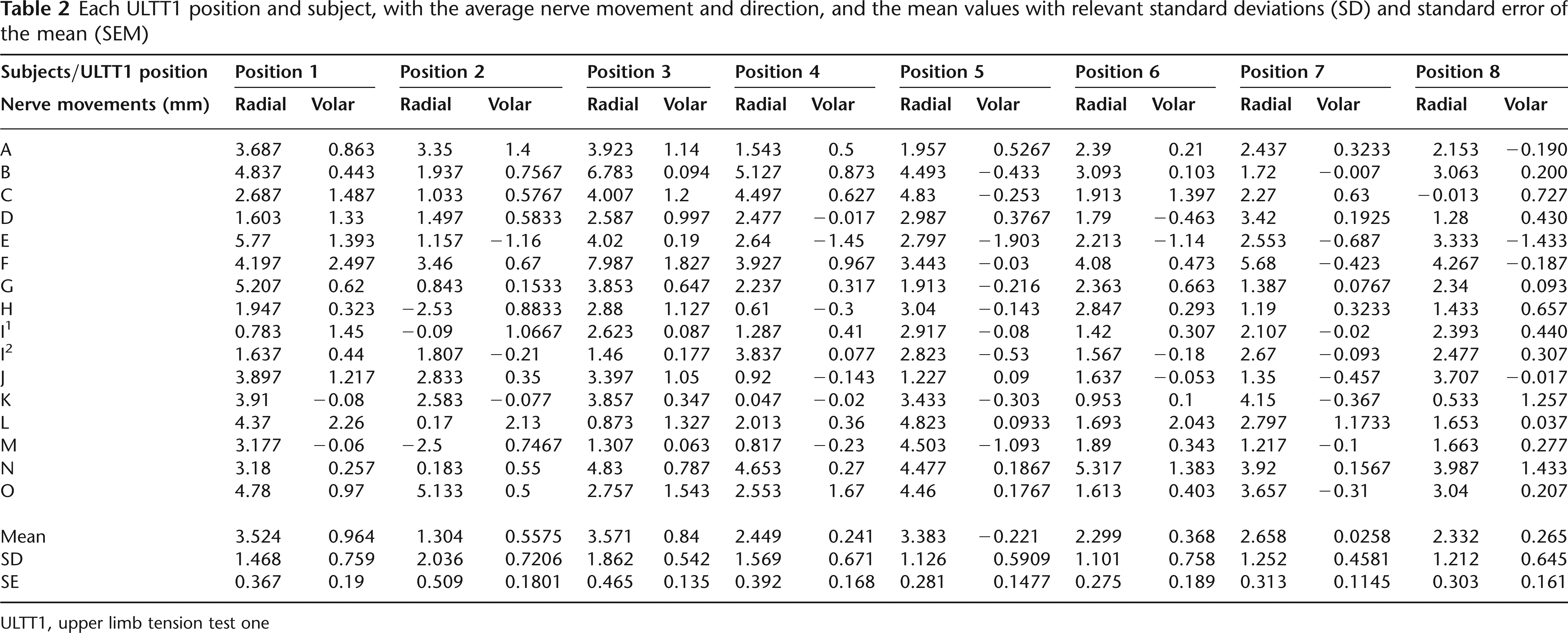
ULTT1, upper limb tension test one
Graph showing the transverse movement of the median nerve at the wrist in all test positions Graph showing the amount of nerve movement with a supinated forearm position

Differences between the movements were found to be statistically significant in transverse movement between the positions of 1 (shoulder neutral, elbow extended and forearm in supination) and 2 (shoulder neutral, elbow extended and forearm in pronation) (P = 0.001). Also between position 5 (shoulder neutral, elbow flexed and forearm supinated) and 6 (shoulder neutral, elbow flexed and forearm pronated) (P = 0.009), both of which showed this significance with the addition of supination. In the volar-dorsal movement it was positions 3 (shoulder abducted, elbow extended and forearm supinated) and 4 (shoulder abducted, elbow extended and forearm pronated) (P = 0.009), and also position 5 (shoulder neutral, elbow flexed and forearm pronated) and 6 (shoulder neutral, elbow flexed and forearm pronated) (P = 0.02) (Table 1 for images of these positions). The position of a neutral shoulder and elbow flexion with the movement of the forearm from pronation to supination (between positions 6 and 7; Table 1) was statistically significant in both the transverse movement (P = 0.009) and volar movement (P = 0.02) of the median nerve at the wrist. There was no significant difference in the transverse movement of the median nerve at the wrist with a change in shoulder or elbow position.
Discussion
Transverse movements of the median nerve at the wrist have previously been measured in subjects with and without carpal tunnel syndrome or non-specific arm pain.11,12,17,18 Research has been completed looking at the strain and tension of the median nerve at the wrist in the upper limb tension test position and in positions of relative relaxation,9,19,20 yet there has been limited research into the effects of the upper limb tension test on the transverse movement of the median nerve at the wrist.
There was significant transverse movement of the median nerve on wrist extension within positions of the ULTT1. This movement was maximal when the elbow was extended and the forearm supinated. The supinated position of the forearm increases the tension in the forearm muscles and thus within the anatomical bed of the median nerve. If looking at longitudinal glide of the nerve, the pronated forearm position should allow further nerve excursion.7, 19 Longitudinal glide of the nerve is altered with increased tension to the nerve, which comes primarily during shoulder abduction.3, 20 However, as shoulder abduction and pronation affect the longitudinal excursion of the nerve rather than the transverse movement, it may explain the outcome of this study, and support the idea that transverse movement of the nerve may be a more sensitive measure of median entrapment neuropathy. 12
Phalen's 21 test states that the already sensitized median nerve can be compressed against the edge of the transverse flexor retinaculum, creating increased paraesthesia. The paper 21 goes on to state that wrist extension increases the pressure within the carpal tunnel, and there is biomechanically more tension on the flexor tendons in the supinated forearm position when the wrist is subsequently extended. An extended elbow will also increase the tension within the flexor tendons, meaning the median nerve will have to move further in a transverse direction away from the tensioned tendons, in order to maintain its integrity.
If elbow flexion produces less tension within the anatomical bed of the median nerve,22, 23 but does not significantly affect the transverse movement of the nerve at the wrist as found in this study, then placing the arm into supination, neutral with the elbow flexed may be a more comfortable position for diagnosing acute nerve pathology in the wrist, while adding wrist extension. Coppieters et al. 4 found that sliding a nerve can give similar results at the area being assessed, when compared with adding full longitudinal tension to the nerve. The author finds these results support the previous study 4 as the change in the kinetic chain did not affect the amount of transverse movement of the median nerve at the wrist (P = 0.731) when compared with the full ULTT1 position. This position, as stated, 4 reduces the amount of aggravation to an already sensitized nerve.
When looking at the longitudinal movement of the median nerve, it has been found that abduction of the shoulder did not significantly increase the tension of the median nerve at the axilla. 20 Kleinrensink et al., 19 who also studied cadavers, found that shoulder abduction, although it did increase tension in the median nerve in the axilla and by the pronator teres muscle it did not affect the tension of the median nerve as it passed through the wrist. This may be relevant if looking at the ULTT1 as a way of diagnosing restrictions in the longitudinal movement of the median nerve at the wrist, but should not have much bearing on the transverse movement. This research supports my findings of no difference in the transverse movement of the nerve at the wrist between the pronated and supinated forearm positions when the shoulder was in abduction; there was not enough change in the tension/strain of the nerve to override the forearm biomechanics and alter the transverse movement of the nerve.
There were two positions in which the nerve moved in an ulnar direction when the wrist was extended, rather than the more common radial direction. 12 This happened to three subjects when the position was pronation with the elbow extended, and one subject when the arm was in pronation abduction with the elbow flexed. One explanation for this could be found in previous research 24 according to which, when the index finger was passively extended, the nerve moved in an ulnar direction. They hypothesized that this was due to the pressure of the flexor tendons on the radial border of the nerve, pushing it in an ulnar direction. The reason only some of the subjects in this study had an ulnar direction of movement could have been due to the order in which they unfurled their digits when their wrist was extended. If they extended their index fingers first, it may have pushed the median nerve in a more ulnar direction than if the unfurling started from the little finger, although there was attempts to standardize this movement.
When looking at the movement that occurred when the forearm was supinated with the shoulder in a neutral position, the authors found the nerve moved an average of 3.52 mm (SD ± 1.47 mm), whereas previous research 24 only found a transverse movement of the nerve of 1.75 mm (SD ± 0.49 mm). This study looked at the movement of the whole wrist into extension, and other studies 24 only assessed transverse movement when the index finger was extended. The author would therefore expect the present study to demonstrate a larger movement, as more tendons are implicated in the movement.
The Nakamichi study 24 is supported by that of Hough et al. 22 who found a transverse movement of 1.75 ± 1.33 mm of the median nerve with the arm in abduction. However, they do not state whether the elbow was in flexion or extension when this movement occurred and as such it is difficult to fully compare the results. 22
When comparing the movement of the nerve with the arm in neutral and the forearm in pronation, this study has very different results from those of Greening et al., 18 who found that when the wrist was in flexion, it was 4.8 mm (SEM = 0.42) more radial than when the wrist was in extension. This study found a movement of only 1.3 mm (SEM = 0.51) with the wrist moving from flexion to extension. This could be the way in which the data were collected in this study compared with the Greening study 18 as they assessed the movement of the nerve in a series of static positions, and the current study measured transverse movement of the nerve through a dynamic movement. This could have affected the images and the final end position. The nerve may ‘slide’ and thus settle into a different end position when the measurement is static, or is held for a longer time at the end of the movement than was done in this study. Further research comparing these different ways of collecting data needs to be completed to be certain, with a longer hold at the end of the dynamic movement.
Study limitations
Had there been more time to collect data, it would have been advisable to gain a second opinion of the nerve positioning and data collection. Having the data collected by a trained sonographer in follow-up studies will increase the robustness of the results. There may be an element of selection bias within this study, as the subjects were friends of the author and colleagues on the MSc course, and may not be representative of the general population. There was no sample size calculation, as participant numbers were based on time available to the author to complete the study. A sample size of only 16 wrists is too small for the author to be confident that the results can be extrapolated to the general population without further research being completed. This study should be repeated with a larger sample size randomly sampled from the general population to increase the validity of the results. It could also be used as a pilot study for further research and aspects of this study could be completed with a population of symptomatic subjects and a control group to increase its external validity and use within the clinical setting.
Elbow extension was not standardized between each subject as position of comfort was used instead. This position was decided upon to make the study more relevant to the clinical setting. In the clinical setting, therapists do not standardize the elbow extension, they extend the elbow depending upon the tension they and the patient feel, and any changes in the subjective markers, such as an increase in pain or pins and needles.
Conclusions
This study has shown that positions of the ULTT1 for the median nerve can be assessed in both the neutral and the abducted shoulder position with no significant difference to the degree of transverse movement of the nerve at the wrist. The transverse movement of the nerve can be assessed with the elbow either flexed or extended with no significant difference between the two positions. However, if the forearm is positioned in supination when the wrist is moved into extension, this gets the largest change in position of the median nerve in normals and may make it a clinically more effective test. If transverse movement of the nerve at the wrist is a more sensitive measure of median nerve entrapment, 12 then one can detect or provoke median nerve transverse movement by asking the patient to supinate the forearm and extend the wrist in any position of the shoulder or elbow. When a nerve is already sensitized, being able to test its movement in a position of offload, such as elbow flexion and shoulder in a neutral position, it is preferable to place it under tension.
Footnotes
Acknowledgements
Thanks go to Mr Henk Giele, Consultant Plastic Surgeon, for assisting in the drafting of this research for publication, and to Mary Reach for assisting in data collection.
Example of Images used in the analysis
(Frames read from left to right).