
Abstract
Avulsion fracture of the base of the second metacarpal is a rare injury due to the stability of the carpometacarpal joints. There are few documented cases in the literature of extensor carpi radialis longus (ECRL) avulsion. The ECRL avulses from the base of the second metacarpal usually as a result of forced wrist hyperflexion and can be exacerbated with the hand in ulnar deviation. This is often as a result of a fall and the patient usually presents with pain in the region of, and dorsal to, the anatomical snuffbox. The base of the second metacarpal articulates with the base of the third metacarpal, capitate, trapezium and trapezoid. The ECRL has its origin on the lower third of the lateral epicondyle and the supracondylar ridge of the humerus and inserts distally into the base of the second metacarpal. The actions of ECRL are wrist radial deviation and wrist extension, the ECRL imparting a greater moment for radial deviation than the extensor carpi radialis brevis, while the opposite relationship is found for wrist extension. This paper presents the case of a patient with this injury, the diagnostic images, subsequent surgical and therapy management and final outcome.
Introduction
A 29-year-old man, right-hand dominant sales manager, presented to the Accident and Emergency department following a punch injury during an altercation.
After initial clinical and radiological assessment by a nurse practitioner in Accident and Emergency, a fracture of the base of the right second metacarpal was diagnosed and a volar plaster of Paris slab was applied. He was then referred to the therapy-led closed trauma clinic for assessment and decision-making with regard to treatment.
Assessment
The patient was assessed by the clinical specialist hand therapist in the closed hand trauma clinic. The trauma clinic is staffed by experienced specialist hand therapists who assess all patients with closed injuries referred from Accident and Emergency. Complex or potential surgical cases are discussed with the hand surgeons based in an adjacent clinic running concurrently.
The patient presented with pain over the dorsal radial aspect of the right wrist and second carpometacarpal joint. There was a palpable tender bony lump between the bases of first and second metacarpals. Active wrist extension and radial deviation were painful in addition to movements of the thumb including pinch grip.
Radiographs (Figure 1) were reviewed and demonstrated a bony fragment at the base of the right second metacarpal with minimal displacement. A very small bony flake was also seen at the radial border of the carpus.
Radiographs showing a second metacarpal base fracture with separate bony flake subsequently identified as being attached to the avulsed extensor carpi radialis longus
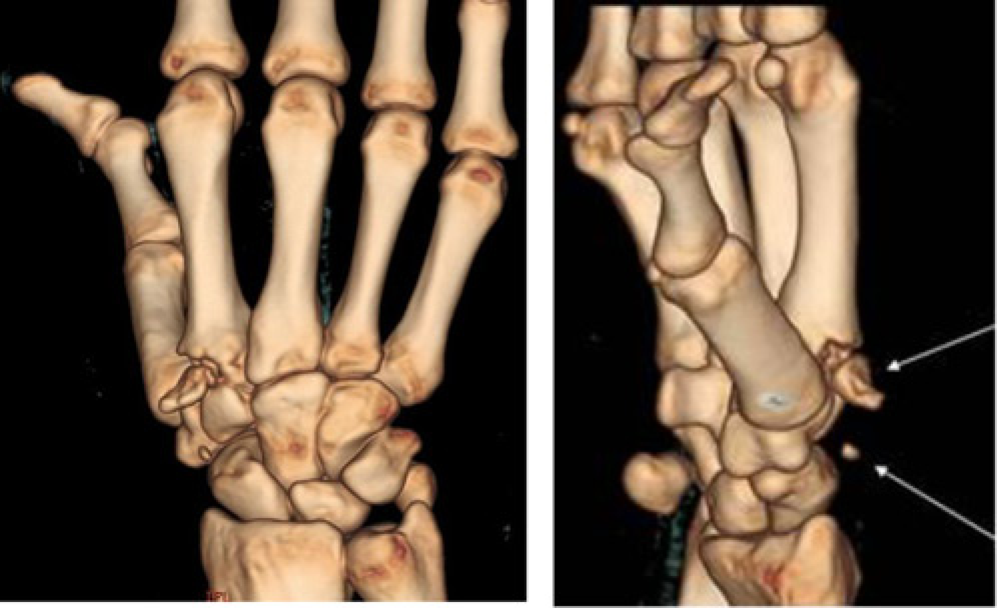
The patient was referred for further imaging to better visualize the fracture and subsequently underwent urgent computerized tomography (CT) scans. The scans (Figures 2, 3a and b) confirmed the diagnosis of the second metacarpal base fracture with an avulsion of the extensor carpi radialis longus (ECRL) tendon attached to the smaller more proximally situated bony fragment.
Transverse computerized tomography slice revealing base of second metacarpal fracture (a) Three-dimensional computerized tomography reconstructions revealing the intra-articular second metacarpal fragment and (b) more proximally base flake of bone lying over the distal scaphoid
Treatment
Initially both options of operative and non-operative treatment were considered by the hand trauma team. However, a review of the literature highlighted not only the likelihood that the ECRL has avulsed more proximally than initially thought (the tendon being located on the bony flake, not on the large fragment) but also the possible complications of treating this fracture pattern nonoperatively which are discussed in the conclusion of this article.
The patient was listed for surgery by the specialist hand therapists and underwent an open reduction and internal fixation (ORIF) (Figure 4). The surgery was carried out under a general anaesthetic with tourniquet control. A longitudinal dorsal incision was made over the base of the second metacarpal and dorsal branches of the superficial radial nerve were seen directly beneath the scar and protected throughout the procedure. The main fragment was reduced and buttressed by a nonlocking low profile T-shaped plate. The avulsed ECRL tendon was re-attached to the dorso-ulnar aspect of the second metacarpal using a non-absorbable suture through the drill holes in the base of the bone. The tissues were then closed in layers with absorbable sutures to close the skin. A volar plaster of Paris slab was then used to protect the surgical repair. The wrist was subsequently immobilized for six weeks in 20° of wrist extension to provide protection for the repaired tendon in a shortened position.
Postoperative radiographs of bony fixation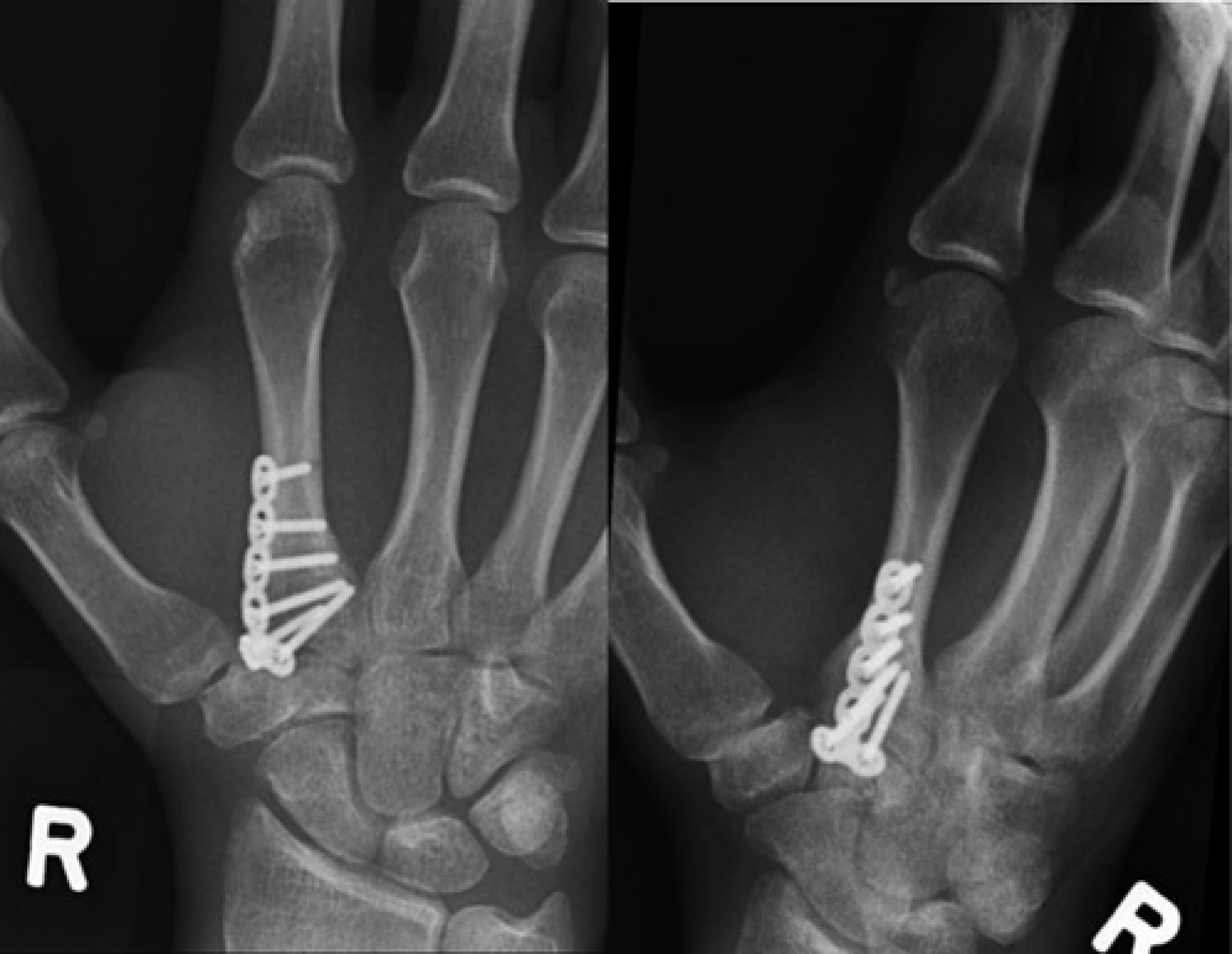
At 10 days postoperatively the wounds were reviewed and the initial back-slab plaster of Paris cast was changed to a complete resin cast. At this review, the patient reported reduced sensation over the radial border of the hand and the thumb likely due to a neuropraxia or scar tethering of the superficial branch of the radial nerve. At six weeks, after removal of the cast, the patient was placed in a removable wrist brace splint for a further week. Radiographs were repeated and demonstrated satisfactory reduction and plate position.
The patient was referred for hand therapy to regain range of motion. Initially active flexion, extension, radial and ulnar deviation movements were performed with flexion and ulnar deviation limited to gentle active motion only to protect the tendon re-attachment, these were progressed to full active range over the following two weeks. Light activities of daily living were permitted but no heavy use or strong gripping. The patient was advised to massage the scar daily. The number of therapy sessions was minimal with no hands on treatment beyond advice regarding movement and use.
At the 9 week review passive stretches to all wrist movements were commenced to further increase range, these were to be performed by the patient at regular intervals four times daily. At 12 weeks postoperation the patient was instructed on progressive strengthening exercises for grip and wrist musculature including wrist extension and radial deviation using theraband for resisted exercise and gripping tools three times daily.
Results
On removal of the resin cast at six weeks the range of movement was recorded, this was then repeated at 12 weeks when the patient was reviewed and range of movement was found to be restored almost to normal (Table 1).
Range of movement of operated right hand six and 12 weeks postoperation compared with an uninjured non-dominant left hand
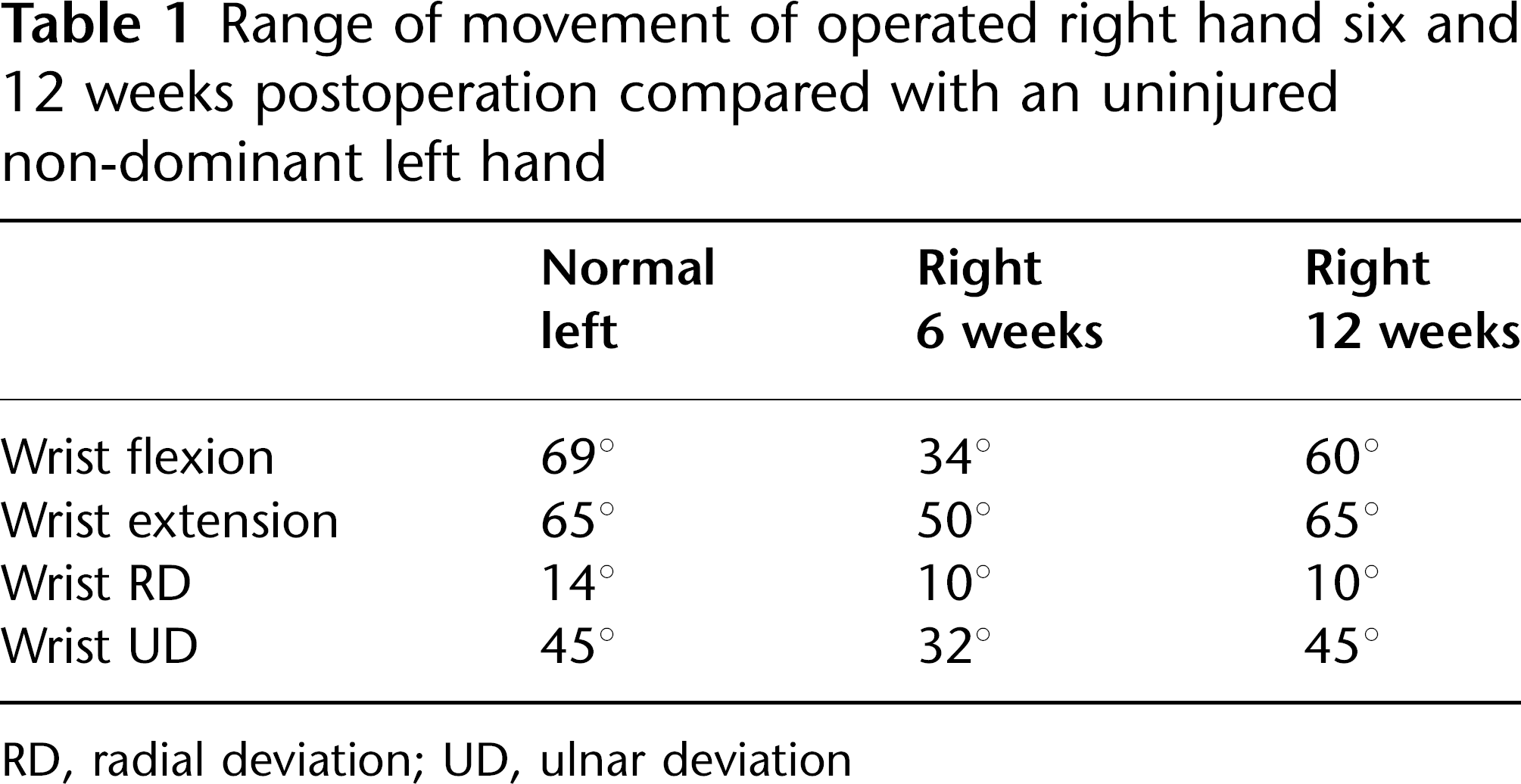
RD, radial deviation; UD, ulnar deviation
Strength was recorded using the Jamar dynamometer and found to be 90% of normal assuming an average 5–10% more power in the dominant hand 1 (left 46.5 kg, right 47 kg). The patient had returned to work after only 1 week postsurgery in his normal administrative role. By 12 weeks he had resumed all former activities. He reported he was experiencing no problems apart from persistent reduced sensation in the dorso-radial aspect of the thumb which, although he found irritating, did not interfere with function.
At a telephone follow-up at eight months postoperation, the patient stated that he still had the persistent parasthesia symptoms and also reported an electric shock feeling on touching the scar. He was advised regarding scar desensitization and a follow-up appointment was arranged to discuss the issue with the surgical team to investigate the possibility of some tethering of a cutaneous nerve in the scar. The patient also reported that he had some feelings of weakness of the right wrist in certain positions during some activities e.g. holding a tray with the forearm in supination. It was suggested that he might wish to attend for a review to be re-assessed and for the hand therapist to consider a programme for specific wrist strengthening in this position if this continued to be troublesome.
Conclusion
There are only 14 cases in the literature (excluding this case) of isolated ECRL avulsion spanning from 1987 to 2008.2–12 Mechanisms of onset have mainly consisted of falls onto a flexed wrist but a dashboard injury during a road traffic accident, 9 and one other injury sustained during an altercation 3 as in this case, have also been reported.
Clark et al. 3 described a clinical sign to aid recognition of this injury: a palpable bone lump on the dorsum of the hand in the presence of wrist extensor pain or weakness after a wrist hyperflexion injury. The patient in this study presented with this sign. Previous papers have discussed both conservative management and surgical fixation to reduce the fracture and repair the ECRL tendon with most authors advocating surgery as the better option.3,5,8–12
Reported complications of conservative management include attrition rupture of the extensor pollicis longus tendon on the displaced bony fragment,2, 6 weakness of wrist extension and grip4, 10 and one paper reported prominence of the metacarpal base requiring surgical removal. 4 In this case study, the patient underwent an ORIF with ECRL re-attachment. He sustained an apparent neuropraxia to the superficial radial nerve causing some mild parasthesia.
Although not essential, CT imaging proved helpful in the diagnosis, CT giving better bony resolution than magnetic resonance imaging and plain radiographs.
The patient did not require extensive rehabilitation and the overall clinical outcome at three months postoperatively was very good in terms of objective measures and return to functional activity. He has some complications with regards to the nerve irritation and loss of strength which may need to be addressed if the symptoms have failed to settle at the next review appointment. Although this is a rare injury, therapists working in the field of acute hand trauma should be aware of this condition and the importance of early diagnosis and effective surgical treatment.
Footnotes
Acknowledgements
The authors thank Fiona Peck for her support and encouragement in writing this paper.