
Abstract
Introduction
Children affected by obstetrical brachial plexus injury frequently have residual externalrotation weakness in the shoulder. Secondary surgical procedures are available for improvement. The aim ofthis study was to describe and compare children's and parents’ expectations, the importance of selectedarm/hand function, and performance of activities before and satisfaction after surgical correction of rotationdeformity in the shoulder.
Method
In the Department of Hand Surgery, Södersjukhuset Sweden, all patients ≥4-year-olds (n = 42)affected by obstetrical plexus injury who underwent secondary surgery to release rotation contracture of the shoulder were included in this study between November 2001 and May 2006. A disease-specific questionnaire was developed and used.
Results
The expectations before surgery were that the majority of the activities and functions would be improved. There were some differences between the adolescents’ and their parents’ expectations. After surgery, both children and parents were overall satisfied.
Conclusion
This study shows that expectations before surgery were high and both children and parents reported positive experiences three months after surgery. A longterm study is warranted if final conclusions are to be drawn.
Introduction
In Sweden an estimated 200–300 children are affected annually by obstetrical brachial plexus injury. In countries with good maternity care, this injury has a frequency of 2–3 per 1000 births. 1 The injury occurs most often in the final stages of difficult deliveries. This can put stress on the brachial plexus, and may cause a nerve injury which affects all or parts of the upper limb. The severity of the injury varies from a paralysed arm to barely visible symptoms compared with the unaffected side. Spontaneous total recovery probably occurs in more than 75% within a few weeks to six months after birth.2–4
Children with obstetrical brachial plexus lesions, even those who recover excellent global function, frequently have a residual rotation deformity in the shoulder, with poor external rotation. This affects the ability to place the arm/hand above the shoulder, e.g. put the hand to the mouth without lifting the elbow (‘trumpet sign’). 5 The lack of external rotation limits use of the hand with precision and security. 5 This impairment affects the child in play and performance in daily activities and restricts the ability to participate fully in activities. 6 Children change as they grow. Their different roles, activities, priorities and the meaning of the roles change during this growth. The roles have a great impact on their identities and choice of activities. 7 Studies on children with obstetrical brachial plexus injury describe problems for these children as they grow older. The problems include, e.g. difficulties in performing activities of daily living and presence of pain.8,9
Before the 1980s, the majority of obstetrical brachial plexus injuries were treated conservatively. The purpose of the treatment was to prevent joint contracture. 10 Today, reconstructive surgery of the nerves can be done to improve recovery from the most severe injuries.11,12 A number of secondary surgical procedures are also available to improve shoulder stability and arm function. The aim of secondary surgery is to improve function for the children and adolescents with remaining dysfunction.11–13
After secondary surgery, a rehabilitation programme is usually provided. Studies emphasize that it is important that a multidisciplinary team provides the rehabilitation, where contributions from both occupational therapists (OTs) and physiotherapists (PTs) are essential.5, 6, 14, 15
The purpose of this study was to examine expectations and the importance of arm/hand function and performance of activities before secondary surgery on the shoulder in children with obstetrical brachial plexus injury; further, to examine the level of satisfaction after surgery and rehabilitation.
An interest in identifying patients’ perception of the quality of care has increased in recent years. 16 Asking people about their ability to perform activities could give important information about their limitations and need for interventions. 17
No studies have been found so far concerning the expectations of the children or their parents before and satisfaction after secondary surgery and rehabilitation of obstetrical brachial plexus injury. There are, however, studies, concerning other diagnoses, describing views from children and parents, where a difference in views between the two groups has been noted.18, 19
Method
Participants and procedure
In the Department of Hand Surgery, Södersjukhuset Stockholm, Sweden, all patients ≥4-year-olds who underwent secondary surgery to release rotation contracture of the shoulder after obstetrical plexus injury were included in this study. All patients were operated with an open subscapularis elongation, to release the contracture. Eleven of them also had a latissimus dorsi to infraspinatus transfer to augment the lateral rotation power, and in 13 patients a dorsal subluxation of the gleno-humeral joint was relocated. The participants were asked to fill in a disease specific questionnaire. This procedure was performed as part of the regular clinical program for the target group during the period November 2001 to May 2006. No ethics committee approval was sought as such service evaluations do not require permission from an ethics committee according to the regulations in Sweden. However, all participants gave informed consent and were assured that their anonymity would be protected. Further, it was emphasized that participation was voluntary and that not completing the questionnaire would not impact or interfere with any ongoing or future treatment. In addition all participants received a standardized rehabilitation program by OTs and PTs. There were 42 children-adolescents, 24 girls and 18 boys, who independently or together with their parents filled in one disease-specific questionnaire about expectations before (Part 1) and one about satisfaction after surgery (Part 2). The children and the parents agreed about who would fill in the questionnaires. The questionnaires were used at the time of secondary surgery for children from the age of four, before and after surgery.
Expectations of improvements and importance of selected activities before secondary surgery on the shoulder
Before surgery, expectations of improvements and importance of selected activities were rated on a four point scale. For the following activities regarding the affected arm/hand: (1) Eat with knife and fork, (2) Drink from a glass without elevating the elbow, (3) Hold the handset of the telephone to the ear and (4) Take an object from a shelf at head height, and (5) Appearance of the arm/hand, (6) Movement of the upper extremity and (7) Strength of the upper extremity. The four-point scale for expectation was graded as follows:
1 = No expectation of improvements, 2 = Little expectation, 3 = Better and 4 = Much better. The scale for importance was scored as follows: 1 = No importance of improvements, 2 = Little, 3 = Great importance and 4 = Greatest importance of improvements. In addition, the presence of Pain in the affected arm was recorded as Yes or No. If Yes, pain intensity was rated on the four-point scale.
Satisfaction with activity performance and upper extremity function after secondary surgery on the shoulder
Three months after surgery and rehabilitation, satisfaction with performance and outcome regarding the selected activities, as well as satisfaction with functioning of the upper extremity were rated on a four-point scale, where 1 = Unable to perform the activity, 2 = Great difficulty, 3 = Some difficulty and 4 = Without difficulty. Satisfaction with the functioning of the upper extremity was rated as 1 = Not satisfied, 2 = Neither-nor satisfied, 3 = Rather satisfied and 4 = Satisfied. Presence of pain was recorded as Yes or No. If Yes, the degree of pain reduction was rated on a four-point scale.
Analysis
During the analysis of the questionnaire, Part 1, the ratings of the expectations of improvement were aggregated: Scores 1 and 2 were classified as ‘no/little’; 3 and 4 were classified as ‘better’. Concerning the importance of the selected activities, 1 and 2 were also labelled ‘no/ little’, 3 and 4 were labelled ‘great’. During the analysis of the questionnaire, Part 2, at three months after surgery, the ratings of the activities were aggregated. Scores 1 and 2 were labelled ‘great’ difficulty; 3 and 4, ‘no/little’ difficulty and finally satisfaction 1 and 2 were classed as ‘not satisfied’ and scores 3 and 4 as ‘satisfied’.
Results
Demographic data of the participants
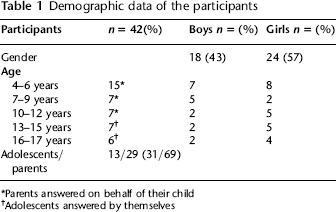
Parents answered on behalf of their child
Adolescents answered by themselves
Parents'and adolescents’ (n = 42) ratings regarding expectations and importance of the activities: functioning of upper extremity (arm/hand) and pain before surgery and ratings regarding the activity performance and satisfaction with the performance, functioning and pain, three months after surgery
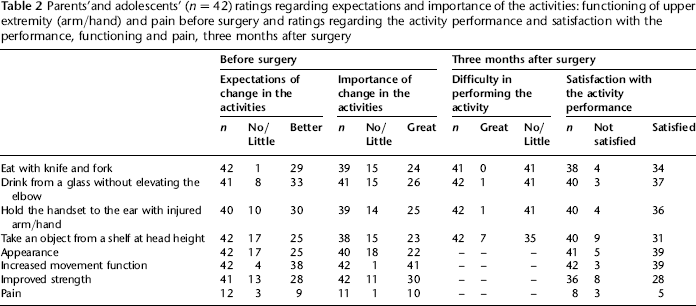
Before surgery, most parents and adolescents had great expectations of change. The most common expectation was that surgery would provide increased movement function, and the second most common was improvement in the activity drink from a glass without elevating up the elbow.
Regarding the importance of the expected changes, the majority of the participants thought that increased movement function was most important followed by improved strength, whereas arm/hand appearance was the item that was ranked as being the least important. All participants gave increased movement function the highest score.
Ratings three months after surgery and rehabilitation are shown in Table 2. The difficulties in performing the selected activities eat with knife and fork, drink from a glass without elevating up the elbow and keeping the handset of the telephone to the ear were rated as ‘no/little’ difficulty by 41 participants.
Three months after surgery and rehabilitation of the shoulder, the participants were satisfied in general with their performance of the activities and with movement function, strength and appearance of the involved arm/ hand. The majority of the participants were most satisfied with the movement function. Both parents and adolescents expressed great satisfaction with the performance of the activities drink from a glass without elevating the elbow and keep the handset of the telephone to the ear and with the arm/hand appearance.
Before surgery, 12 participants declared that they had pain. Three months after surgery and rehabilitation, nine participants had pain, four of them also indicated pain before surgery. Among the participants who rated pain three months after surgery, five were satisfied and only one was not satisfied. This participant also indicated pain before surgery and rehabilitation.
The adolescents had greater expectations than the parents before surgery and overall they also rated the importance higher. All of them used the highest score for the importance of increased movement function, while only half of the parents used the same rating. The only question where the majority of the parents rated no/little importance was regarding appearance, whereas the adolescents felt to a greater degree that appearance was of importance. After surgery, the parents used ‘no’ or ‘little’ difficulty for the performance of all activities except for eat with knife and fork. In contrast, the adolescents rated the performance of the same activity as ‘no’ or ‘little’ difficulty.
Discussion
To our knowledge, there are no previous studies concerning expectations before and satisfaction after secondary surgery and rehabilitation of the shoulder after obstetrical brachial plexus injury. This study shows that, before secondary surgery of the shoulder after obstetrical brachial plexus injury, the expectations of both adolescents and parents were that the majority of the rated activities and functions would be improved. Three months after surgery, both groups were overall satisfied and considered that the rated activities could be carried out with little or no difficulty.
Expectations of performance of the activities and functions were high before surgery. This result may have been influenced by all the information given beforehand as well as attitudes towards surgery as expectations reflect patients’ beliefs. Ratings regarding importance are considered to have a more valid basis for the score from a patient perspective as importance ratings reflect how the person wants the results to be. 16 The activity take an object from the shelf at head height, got the lowest importance rating among the four selected activities both before and after surgery. An explanation might be that this activity requires good arm movement function, i.e. the arm can be lifted above shoulder level, which most of the children with plexus injury have difficulties to do.5,9 The children may have been used to compensating in various ways, which might have influenced their expectations before surgery.
After surgery and rehabilitation, the low rating of the performance of the activity take an object from the shelf at head height, might also be influenced by the short lapse of time after surgery. This also might be the case with the great difficulty with the arm/hand movement function improved strength, which had received the lowest rating regarding satisfaction. Three months after surgery is a very short time for the healing process and rehabilitation, which is still in progress. It also takes time to develop new patterns for performing various activities, i.e. reaching an object on a shelf, which requires good arm movement and strength.
Before surgery, 12 participants reported that they had pain. Three months after surgery and rehabilitation, the majority (eight) reported that they had no pain. Nine participants in total had pain after surgery, of whom five reported pain after surgery but not before. This pain may disappear over time as the healing process was still in progress. However, longer follow-up is needed to ascertain that surgery does not induce chronic pain.
There were differences in ratings between the adolescents and the parents similar to the findings of Daltroy et al., 20 who have shown that adolescents rated themselves higher than their parents concerning physical and mental health, while parents had higher expectations for treatment outcomes. In some items, e.g. increased movement function, the reason for the difference between children and their parents in how they rated importance might be that adolescents are likely to demand more movement function and hence increased ability in the performance of the activities in order to be able to participate in different contexts. Children continuously change and develop as they grow. Their roles and expectations and the meaning of the roles also change during this set. The attitudes of friends also affect the way teenagers look at their own bodies. Furthermore, the physical development associated with puberty leads to different social and psychological consequences for different people. 21 Our roles are dynamic in the way they are acquired and replaced through life. 7 Limitations in the physical capacity could disturb the expectations which are parts of our roles or might even disrupt the roles. 17
In order to get an idea of patients’ expectations before surgical management of the shoulder after obstetrical brachial plexus injury and an understanding of changes after surgery and rehabilitation, we chose to administer self-assessment questionnaires. The questionnaires were designed to be used in clinical practice, easy to administer in a standardized way and easy for the patient to fill in. However we cannot draw any conclusions regarding differences between pre- and postratings of the status since the questions were not identical pre- and postsurgery. The focus before surgery was on the expectations and the importance of the four selected activities, whereas after surgery the emphasis was on satisfaction with the performance of the same selected activities. To allow comparison between the pre- and postsurgical status there is a need to develop the questionnaire so that, e.g. the self-rated performance of the selected activities can be done both before and after surgery.
Another limitation of the study is the short time that had elapsed between surgery and the three months data collection. We chose to do the postoperative evaluation at three months, because at this time most of the patients were thought to have returned to full daily use of their arms and they still had a good recollection of their preoperative function. Therefore they were expected to be able to do a useful comparison at this time. However, the questions were designed on a basis of our clinical experience and consisted of focused and structured questions as recommended in order to get an answer regarding specific problems in a patient group. 22 It is very important to keep focusing on the patients’ views of the quality of care, in spite of the increasing demand for shorter treatment periods with continuous high quality outcomes.
Conclusion
This study shows that expectations before secondary surgery of the shoulder after obstetrical brachial plexus injury were high. The study also shows some differences between adolescents’ and parents’ ratings, i.e. the adolescents rated the importance of positive change in the activities and functions higher. Further development of the questionnaire to include a question regarding satisfaction with the performance of selected activities both before and after surgery is needed to make comparisons. In spite of the few participants and the high expectations, this study indicates positive patients’ and parents’ experiences at three months after surgery. A longterm study is warranted if final conclusions are to be drawn.
Footnotes
Acknowledgements
My thanks go to my colleagues Birgitta Lindqvist for initiating the design of the questionnaire and Ann-Marie Rosenquist for support and creative comments in preparation of the manuscript.