
Abstract
Summary
The aim of the study is to evaluate the influence of antiretroviral treatment on health-related quality of life (HRQOL) of three groups of HIV-positive inmates: those who are taking antiretroviral treatment, those who are not on treatment as it has not yet been indicated, and those who refuse to take treatment even though it has been recommended. A cross-sectional study was conducted on 585 HIV+ inmates in three prisons. The response variable was HRQOL. Independent variables were: sociodemographic variables, psychosocial and drug-related variables. Two multivariate linear regression models were constructed in order to determine the HRQOL, physical health score (PHS) and mental health score (MHS), for each of the three groups identified, using patients who refused treatment as the reference category. Patients who refused therapy had a lower MHS compared with patients in whom treatment was not indicated (P = 0.038). With regard to PHS, patients refusing therapy had a lower score than patients who were not indicated therapy (P = 0.005), and than patients receiving therapy (P = 0.010).
Introduction
The chronic nature of HIV infection has brought about a change in its therapeutic objectives. These objectives are no longer limited to increasing survival and reducing the incidence of opportunistic infections.1,2 There is a new tool in this context: health-related quality of life (HRQOL). In the nineteenth century this was defined as a subjective well being 3 and in recent years this tool has been widely used in health, and in chronic disease in particular.
The HRQOL assesses intrinsic, changing aspects in a patient's life. The assessment does not necessarily coincide with the severity of the disease as defined by the patient's doctor. 4 The HRQOL considers the patient's perception as an essential aspect of evaluating health results. 5
Outside the prison environment, there have been many studies on HRQOL in HIV-positive patients,6–10 describing diverse factors that are associated to QOL. However, few studies have been conducted in prisons. The prison environment has unique characteristics that means that QOL factors in the non-prison environment cannot be extrapolated to a prison environment. This fact is demonstrated in the case of antiretroviral adherence. 11
HIV infection prevalence in Spanish prisons stands at 12%, which is the highest rate in Europe. 12 About 52% of seropositive prisoners are on antiretroviral therapy (ARV). 13 The therapeutic opportunities and conditions are the same in Spanish prisons as in a non-prison environment. 14 Although the same criteria apply for starting treatment, the final decision lies with the individual doctor and with the patient who is free to decide whether or not to follow his/her doctor's advice. 15 In the case of antiretroviral therapy, these decisions classify patients into three groups: those who are on antiretroviral treatment, those who are not on treatment as it has not been recommended and those who refuse to take treatment although it has been indicated.
It has been reported that for many inmates, the time spent in prison is the only occasion they have to receive the specialized medical care that is required for their disease. 16 It has been described in literature that patients do not receive health care when they leave prison, and this shows the difficulties that this population group has in gaining access to health care.
Furthermore, patients who refuse to take antiretrovirals in a non-prison environment usually lose contact with health services and therefore are not available as study subjects. For all these reasons, prisons offer an opportunity to maintain contact with this population group, which is uncommon in the literature. 17
The aim of the study is to evaluate the influence of antiretroviral treatment on QOL of three groups of HIV-positive inmates: those who take treatment, those who do not take treatment as it has not been indicated and those who refuse to take treatment although it has been indicated.
Materials and methods
A cross-sectional study was conducted on all HIV-positive inmates in prisons in Albolote (Granada), Córdoba and Huelva between May and July 2004.
Variables collected
The response variable was HRQOL. Independent variables were: sociodemographic variables, psychosocial variables and drug-related variables; age, gender, level of education (incomplete primary education, and primary or secondary education), social support in prison and methadone treatment. Clinical and antiretroviral treatment variables: CD4 lymphocyte count (cells/mm3, viral load (RNA copies/mL); definitive AIDS stage, time as antibody carrier, hepatitis C infection, mental health problems, self-perception of health in comparison with the previous year (improvement, same or deterioration) and other chronic diseases; whether on ARV or not, and the reason for not receiving treatment (not indicated by the doctor or refused by patient), whether the patient believes that he/she is receiving the help he/she needs for the disease, and other treatment prescribed. Variables related to the prison environment: prison situation (preventive detention a or prison sentence), length of sentence and time still to serve in prison (in months), opinion of quality of meals (good or bad), any court cases pending and destination in prison (work or occupation in prison).
Preventive or provisional prison is a cautionary measure, which consists of provisional imprisonment while the prisoner awaits trial. This type of imprisonment must be approved by the judiciary authority and deprives the affected party of his or her freedom as a result of being charged for a crime.
Measurement tools
HRQOL was evaluated through the Spanish version of Medical Outcomes Study (MOS)-HIV, developed from the MOS. This is one of the most commonly used measures to evaluate the HRQOL in seropositive patients.18,19 It consists of 35 items grouped in 11 health domains that result in two global scores: physical health score (PHS) and mental health score (MHS). It takes 10–15 min to complete and the Spanish version has been shown to have sufficient reliability and validity to be used in clinical investigation. 20
Psychological distress: was measured with the 12-item General Health Questionnaire (GHQ-12). This questionnaire has been validated in this setting. 21 It is a self-administered questionnaire. A structured questionnaire that has been used before in this setting was used for other variables. 22
Procedure
Interviews were organized by the medical department at each prison, with the prior authorization of the Prison Director and the Technical Board of the Prison Centres’ General Office.
Questionnaires were administered by trained interviewers who were unrelated to the prison environment. After explaining to the inmates the study objectives and the voluntary nature of participating in the study, the inmates signed an informed consent, in accordance with article 8.1 of the prison law. Likewise, confidentiality of data was guaranteed. Hepatitis C infection, definitive AIDS stage and CD4 and viral load counts were obtained from computerized clinical records.
Flow cytometry was used to measure CD4 and the nucleic acid sequence-based amplification (NASBA) technique was used to measure the viral load. A viral load of <50 copies/mL was considered as undetectable.
Statistical analyses
Statistical analysis was performed using the statistical package SPSS 12.0. First, a descriptive analysis was performed with reference to frequency, percentage, mean and standard deviation. Second, an analysis was made of any differences in the PHS and the MHS in the HRQOL, according to the independent variables. For independent qualitative variables with normal performance and homogeneity of variance, Student's t-test and ANOVA were used. For the other variables, the Mann-Whitney U-test and Kruskal-Wallis H-test were used.
Finally, two multivariate linear regression models were constructed in order to determine the two scales within HRQOL, (PHS and MHS), for each of the three groups identified, using patients who refused treatment as the reference category. Patients who were not prescribed antiretrovirals due to adverse reactions to therapy were excluded from this analysis. Both models were adjusted by means of potentially confounding variables, such as level of education, mental health, methadone treatment, self-perception of health, definitive AIDS stage, time in prison and opinion of meals. Dummy variables were created for independent variables with more than two categories. Variance homogeneity of variables was verified, along with model homocedasticity and non-colinearity of variables. A significance of 5% was established.
Results
Information was obtained on 585 inmates out of a total of 614 (95.27%). Mean age in the sample was 37.03 years, 8.4% were women and 62.2% had not completed primary education; 43.9% of the inmates said they felt supported in prison and 49.7% of the population were on methadone treatment.
With reference to clinical variables, mean CD4 was 427.82 cell/mm. 3 ; 32.7% presented an undetectable viral load and 38.3% had more than 1000 RNA copies/mL. Mean time since HIV infection had been detected was 149.89 months; 20% had a diagnosis of AIDS; 86.1% had Hepatitis C co-infection and 26.2% stated that they had another chronic disease; 61.3% had psychological distress and 35.2% stated that their state of health was worse than the previous year, in comparison with 36.7% said they felt better than the previous year.
With regard to variables related to ARV, 45% were not on antiretroviral therapy. Within this group, 59.1% had not been indicated therapy and 37.1% had refused therapy. 38.5% were being treated for other diseases apart from their HIV infection. Patients had commenced ARV a mean number of 1.4 times during their life.
In relation to the variables referring to the prison environment, 3.4% of inmates were in preventive detention, 20% had a pending court case and 52.1% had an occupation in prison. Mean length of sentence already served was 31.02 months and mean pending sentence was 24.48 months; 80.2% graded prison meals as poor (Table 1).
Population characteristics and their relation to quality-of-life scores (MHS and PHS)

Student's t-test
Mann-Whitney U-test
ANOVA
Kruskal-Wallis H-test
MHS = mental health score; PHS = physical health score
Table 2 shows the characteristics of each of the subgroups, according to ARV prescription. It is interesting that inmates receiving treatment had a higher prevalence of AIDS (27.8%), higher frequency of social support (46.4%), better opinion of prison food (21%) and had received more courses of ARV (1.84). With regard to inmates who were not prescribed treatment, this group contained a larger percentage of women (11.1%), were younger (36.5 years), had been in prison for longer (37.81), had a higher level of education (43.8% had completed primary education), had a higher incidence of preventive detentions (5.2%) and had had antibodies detected a shorter time ago (142.52 months). Finally, the group of patients who refused therapy were those who had a longer time still to serve (30.61), higher viral load and lower CD4 count (65755 and 305.06, respectively), and a lower incidence of occupation in prison (41.1%). In this group, the inmates showed a higher rate of pending court cases (22.9%), methadone treatment (62.5%), hepatitis C co-infection (91.1%), mental health problems (65.9%), other chronic diseases (80.9%) and also more received treatment for other chronic diseases (41.7%).
Characteristics of seropositive inmates receiving treatment, those who refuse treatment, and those in whom treatment is not indicated
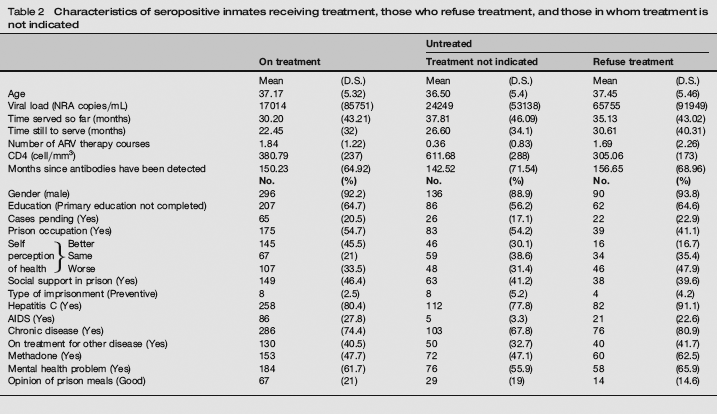
Table 3 shows the mean HRQOL scores for both scales and the 11 domains. Patients who were not indicated treatment had the highest HRQOL scores. In contrast, patients who refused treatment had the lowest HRQOL scores in the two global scales and the 11 domains alike.
Quality of life according to whether antiretrovirals are prescribed or not, and whether the patient refuses treatment

Krustal-Wallis H-test
MHS = mental health score; PHS = physical health score
When differentiating between the reasons for not taking therapy, it was observed that patients who refused therapy had a lower MHS compared with patients in whom treatment was not indicated (P = 0.038). With regard to PHS, patients refusing therapy had a lower score than patients who were not indicated therapy (P = 0.005) and than patients receiving therapy (P = 0.010) (Table 4).
Quality of life in treated inmates and untreated subgroups (treatment refused and treatment not indicated)
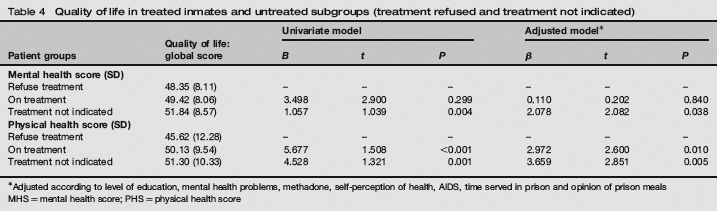
Adjusted according to level of education, mental health problems, methadone, self-perception of health, AIDS, time served in prison and opinion of prison meals MHS = mental health score; PHS = physical health score
Discussion
Although there are other articles that evaluate QOL in HIV-positive inmates, 23 this is the first that not only includes those who refuse ARV, but also distinguishes the former from those who take the therapy and those in whom ARV is not yet indicated. As a result, it is harder to compare the results, because of the absence of data in and outside prison environments.
This study has several limitations that should be taken into consideration when interpreting the results. The cross-sectional nature of the study does not enable causal relationships to be established. It should also be considered that patients in prison were in a poorer state of health at the time of the study, which would affect the external validity of the study. Also, patients refusing ARV may be the ones who refused to participate in the study. However, this percentage was too low to affect the validity of results. Furthermore, HIV infection has undergone major changes with regard to clinical criteria for commencing therapy, and also in the therapeutic arsenal used in such therapy. This means that we are unable to confirm that the former criteria for starting ARV were the same for all study patients.24,25 Even nowadays, with standard criteria for action followed in all prisons, it is recommended to carry out an individualized study on each patient, and this implies that there may be clinical variability. 25
In this study, inmates who refused treatment presented a lower QOL than those receiving treatment and those who were not indicated treatment.
In previous articles, on the non-prison environment, mental and physical HRQOL are similar in treated and untreated patientss. 26 This similarity might be explained by the fact that the untreated group consisted of two subgroups of very different patients, since some do not take treatment because it is not indicated, and in the other group ARV is indicated, but refuse to take it.
If untreated persons present a better QOL in the non-prison environment, this may be because patients who refuse to take therapy are not included in these studies.
There are several factors that could explain why inmates who refuse therapy have a lower QOL. First, it should be considered that in Spain the protocol for indicating ARV states that a CD4 lymphocyte count of between 200–350 cell/mm3 is the most significant factor of reference to start therapy. 15 Thus, patients in the group that refuse antiretrovirals have low CD4 levels, and this in itself is related to a low QOL and a higher rate of progression to AIDS and death. Furthermore, the profile of those who refuse therapy, bears the closest relation with parenteral drug abusers and it is logical that this will influence their QOL. Finally, the fact that they are not on treatment will jeopardise the physical consequences of their disease (apart from QOL). This may be the cause of a lower level of physical activity and a lower rate of occupation in prison and could influence these differences to some extent at least.
According to the prison doctors, the principal reasons given by patients for refusing ARV are their adverse effects and the excessive number of drugs that have to be taken in antiretroviral therapy. Although it has been well demonstrated that these factors are negatively associated with QOL, it is likely that the excessive importance given to these factors actually make patients refuse to start treatment. This study concludes that apart from the adverse effects of antiretrovirals, the QOL of HIV-positive patients who refuse therapy is lower than in the rest of the population.
The results of this study could offer prison doctors a tool for persuading inmates who refuse therapy to take it, because it will give them a better QOL. This is extremely important because it appears that seropositive patients with a better QOL have a higher survival rate. 27
Access to the seropositive population outside prisons is largely limited to patients who attend for treatment. This neglects all patients who cannot or do not wish to be treated. It is logical that this group will probably be comprised of patients who are not very concerned about their health, or who suffer a degree of social exclusion. In this respect, prisons offer an excellent opportunity to identify the needs and motivations of this group, and to encourage patients to commence therapy, which has shown to be so effective. Thus, not only will we be able to improve the health of these inmates, but also to prevent an escalation of infections such as tuberculosis.
Footnotes
Acknowledgements
The authors would like to thank Fernando Ruiz, Albolote prison doctor, for his collaboration in this study. Work subsidised by the Andalusian Health Service, dossier no. 262/02 and by the Epidemiology and Public Health Network (Carlos III Health Institute) (C03/09).