
Abstract
Summary
The aim of the study was to determine human papillomavirus (HPV) type-distribution in the cervix of Chinese women, and to estimate the potential future impact of HPV prophylactic vaccines for cervical cancer prevention in China. A total of 32 studies using polymerase chain reaction for HPV detection were included in the meta-analysis, including 2844 invasive cervical cancer (ICC), 820 high-grade squamous intraepithelial lesions (HSIL), 432 low-grade squamous intraepithelial lesions (LSIL) and 2902 women with normal cytology/histology. The overall and type-specific HPV prevalence of 18 HPV types (HPV 6, 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68, 70, 73 and 82 of different cervical stages) were estimated. Overall HPV prevalence was 83.7%, 66.2%, 61.3% and 11.2% in ICC, HSIL, LSIL and normal, respectively. HPV 16 was the predominant type in all cervical stages. Estimated HPV 16/18-positive fractions in ICC, HSIL, LSIL and normal were 69.7%, 45.5%, 32.23% and 4.6%, respectively. HPV-16/18 vaccine has the 69.7% potential prevention in ICC. HPV 58 and 52 were the priority HPV types in Chinese women.
INTRODUCTION
Cervical cancer is one of the leading cancers among women worldwide. 1 An estimated 493,000 new cases and 274,000 deaths from invasive cervical cancer (ICC) occur among women worldwide each year according to the global data from the International Agency for Research on Cancer (IARC). 1 Approximately 100,000 cases occur annually in China where cervical cancer is the leading form of cancer threatening the health of women.
Human papillomavirus (HPV) is a necessary cause of ICC and its associated precursors including cervical intraepithelial neoplasia grade 3 (CIN 3). 2–6 There was sufficient evidence to establish carcinogenicity for HPV types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59 and 66. 7 The detection and control of the HPV viral infections has became the focus of both primary and secondary cervical cancer prevention strategies. 8 Prophylactic HPV vaccines hold great promise to reduce the global burden of cervical cancer if coverage is ensured. 9 Previous meta-analyses indicate a geographic variation in the distribution of HPV types: 10–15 HPV types 16 and 18 being the most common across all geographical sites, with differences in the prevalence of other oncogenic HPV types (e.g. third, fourth). 10,11
With the recent successful development of HPV prophylactic vaccines, an exploration is warranted of the potential future impact of HPV prophylactic vaccines for cervical cancer prevention in China. Data on HPV type-distribution in China will be important to examine, and assist in the identification, of those additional HPV types which should be considered for the development of future generation HPV prophylactic vaccines. Several studies have been conducted to investigate HPV type-distribution among Chinese women. No systematic review of the literature, however, has been conducted to determine a clear pattern of HPV type-distribution in Chinese women, stratified by stage of cervical disease.
The primary aim of this meta-analysis is to describe HPV type-distribution in Chinese women with and without cervical abnormalities, and to estimate the potential future impact of HPV prophylactic vaccines for cervical cancer prevention in China.
MATERIALS AND METHODS
Study selection
Literature material was selected from citations listed in Medline and the Chinese literature database CNKI. Key search terms included were: ‘cervical cancer/cervical neoplasia,’ ‘human papillomavirus (HPV),’ ‘human,’ ‘female’ and ‘polymerase chain reaction (PCR).’ 11–13 The analysis included peer-reviewed published literature in the Medline database up to October 2006. Paper inclusion criteria in this pooled-analysis included: (1) cervical specimens were from Chinese women, including China mainland, Hong Kong and Taiwan; (2) identified clear pathology or cytology classification: ICC, high-grade squamous intraepithelial lesions (HSIL), low-grade squamous intraepithelial lesions (LSIL) or normal cytology/histology; (3) sample sizes ≥20 cases for each classification group; (4) HPV DNA detection by PCR with testing methods clearly described and (5) the detection of at least one other HPV type other than HPV 16, 18, 6 or 11.
Where available, HPV DNA prevalence for ICC was stratified by histological diagnosis into squamous cell carcinoma (SCC) or adeno- and adenosquamous carcinoma (ADC). If histology-specific HPV prevalence was not reported, cases were classified as being ICC. The classification of HSIL according to the Bethesda system confirmed cases of CIN2, CIN3. LSIL confirmed as CIN1. The ‘normal’ group of this analysis composed the ‘control’ group of case–control studies of ICC, HSIL, LSIL group or of women from population-based studies.
Data abstraction
The following key information was extracted for each study: (1) geographical site; (2) classification of pathology or cytology (ICC [SCC/ADC], HSIL [CIN 2/3], LSIL [CIN 1], normal); (3) type of cervical specimen (fresh or fixed biopsy tissue, exfoliated cells or the combination of them); (4) chosen PCR primers used for HPV detection; (5) type-specific and overall prevalence of HPV infection, stratified by cervical disease grade and (6) publication year. For studies comparing HPV prevalence across two countries/regions, data were separated into regional components, respectively. 16,17
Estimation of type-specific prevalence
HPV prevalence was expressed as the proportion of HPV DNA-positive cases among all cases tested for HPV overall or for the specific HPV type. Type-specific HPV DNA prevalence included the detection of the 18 most common HPV types (HPV 6, 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68, 70, 73 and 82), consistent with a previous review. 11,15 Multiple HPV infections were separated into constituent types, thus type-specific HPV prevalence figures include that in either single or multiple infections. 15
Statistical analyses
Overall, HPV DNA prevalence was adjusted for five potential confounding factors (geographical area, classification of cervical disease status, publication year, type of specimen for HPV DNA testing and type of PCR primers used) using unconditional multiple logistic regression analysis. Overall, HPV prevalence and adjusted HPV prevalence with 95% confidence intervals (95% CI) for each cervical lesion grade were presented after adjustment for statistically significant variables. P values are presented comparing HPV overall prevalence by strata of selected variables, with corresponding chi-square (χ2) tests. Type-specific HPV prevalence is compared between ICC and other cervical grade classification: HSIL, LSIL and normal using prevalence ratios with 95% CI. All statistical analyses were conducted using SAS version 8.0.
RESULTS
Studies included
A total of 32 studies were included with a total of 6998 women. HPV DNA prevalence data was available for 2488 ICC, 820 HSIL, 432 LSIL cases and 2902 women with normal cytology/histology (Table 1). Twenty-four articles were in English and eight were Chinese versions. Among the 2844 ICC cases, 1545 (54.3%) were SCC, 176 were ADC and 1123 were unspecified ICC cases.
Overall HPV prevalence in 6988 women from China, stratified by cervical lesion degrees
ICC = invasive cervical cancer; HSIL = high-grade squamous intraepithelial lesions; LSIL = low-grade squamous intraepithelial lesions; CI = confidential interval
Meta-analysis of overall HPV prevalence
In ICC, HSIL, LSIL and normal group, overall crude HPV prevalence was 83.9%, 77.4%, 76.2% and 12.6%, respectively. Adjusted overall HPV prevalence was 83.7% in ICC, 66.2% in HSIL, 61.3% in LSIL and 11.2% in normal cytology/histology specimens (Table 1). Overall, HPV prevalence increased notably with increasing grade of cervical disease from normal, LSIL, HSIL to ICC (trend test P < 0.001).
In ICC, overall crude HPV prevalence in SCC, ADC and unspecified ICC was 81.6%, 70.5% and 89.1%, respectively, and adjusted HPV prevalence was not statistically significant (P = 0.06). HPV prevalence in China mainland (82.3%) was not statistically, significantly different with Hong Kong (83.3%) and Taiwan (85.8%) (P = 0.06). With regard to PCR primers, HPV prevalence was higher in specimens that were tested using GP 5+/6+ (86.7%) or MY 09/11 (84.1%) primers when compared with type-specific PCR (TS-PCR) only (67.0%) (P < 0.0001). Overall adjusted HPV prevalence increased by date of publication, from 76.6% among studies published before 2000, 84.6% in those published 2000–2003, to 90.6% in those published after 2004 (trend test P < 0.0001).
Meta-analysis of type-specific HPV prevalence
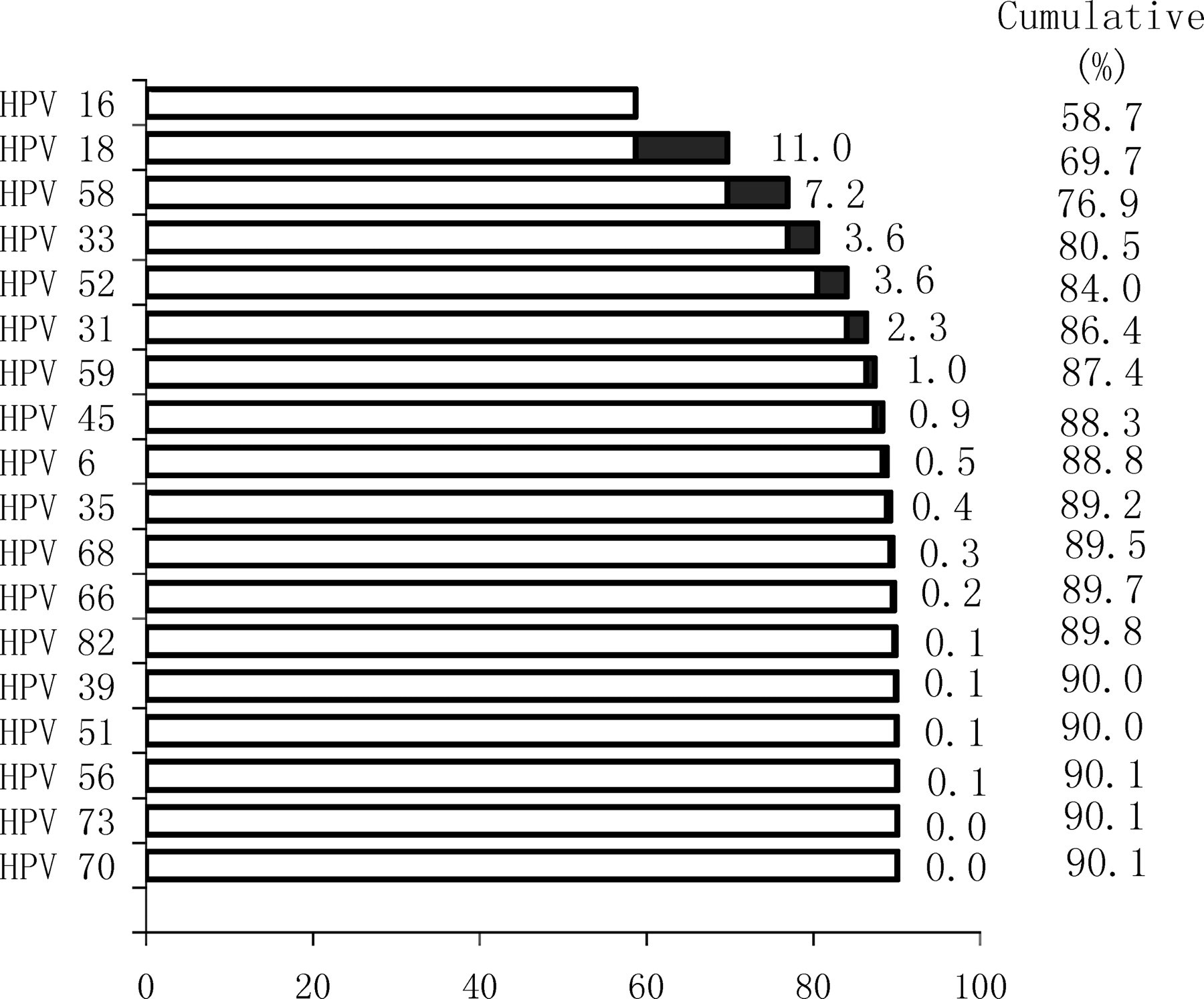
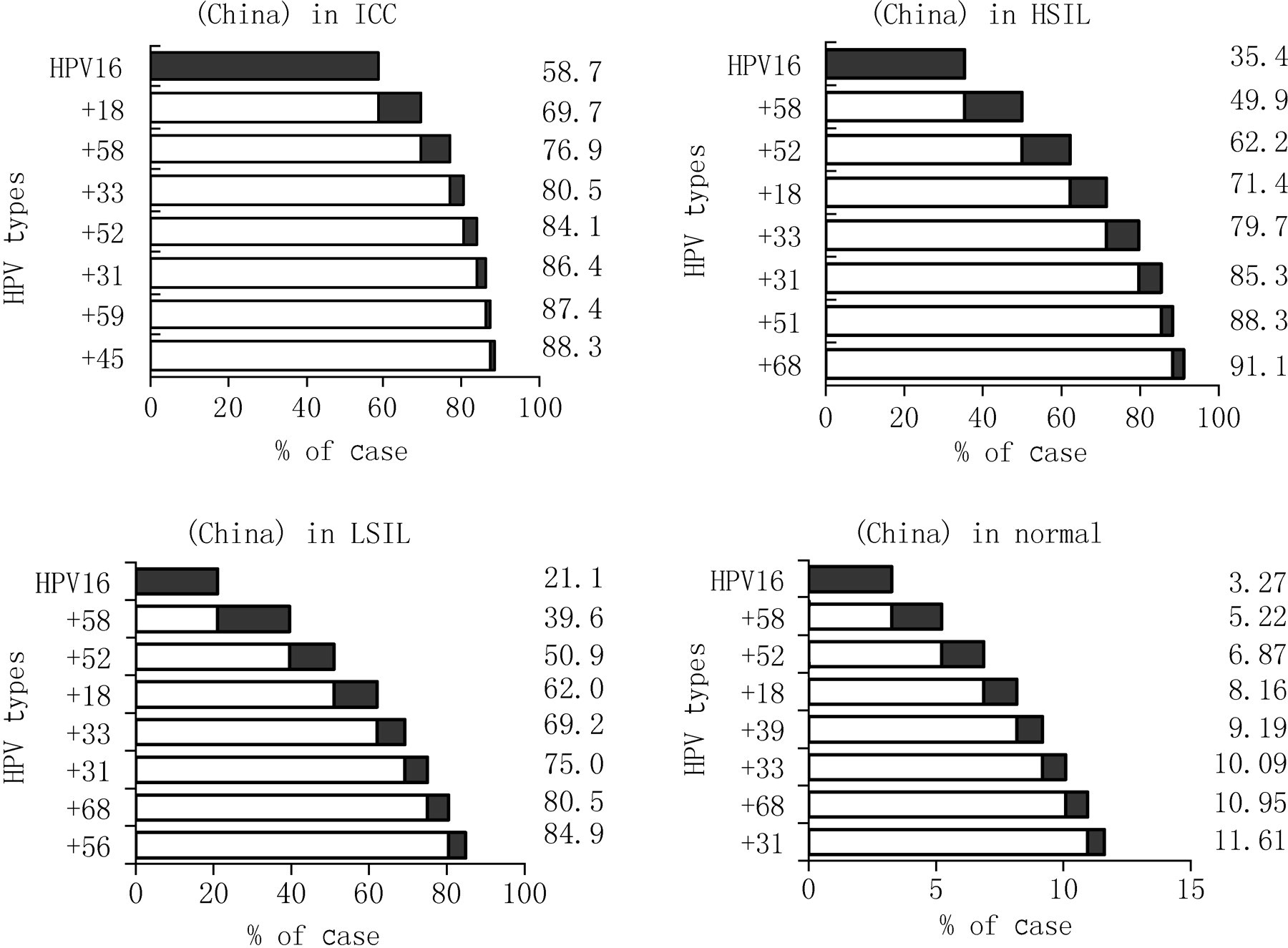
The type-specific prevalence was estimated respectively stratified by classification of lesion. In decreasing order of HPV prevalence, the 10 most common HPV types in ICC specimens from China were HPV 16, 18, 58, 33, 52, 31, 45, 59, 6 and 35 (Figure 1). In women with HSIL, HPV 16, 58, 52, 18, 33, 31, 51, 68, 39 and 66 were the most common types. The most frequently detected types were HPV 16, 58, 52, 18, 33, 31, 68, 56, 66 and 39 in LSIL and HPV 16, 58, 52, 18, 39, 33, 68, 31, 66 and 6 in women with normal diagnoses. HPV 16 was the most predominant type in all cervical grades, being 58.7% in ICC, 35.4% in HSIL, 21.1% in LSIL and 3.3% in normal specimens. In ICC, HPV 18 and 58 were most common following HPV 16. The second and third most common types were HPV 58 and 52 in HSIL, LSIL and normal cervix (Figure 2).
Percentages of cervical cancer cases attributed to the most frequent HPV types in China
HPV type-distribution by cervical lesion degrees in Chinese women
The HPV 16 type-specific prevalence in SCC (58.4%) was significantly higher than that in ADC (35.2%) (P < 0.0001). In contrast, the HPV 18 was more common in ADC (32.3%) than in SCC (6.7) (P < 0.0001).
The possible potential impact of an HPV 16/18 vaccine for the prevention of cervical abnormalities may be estimated by the HPV 16/18-positive fraction (estimated by addition of the type-specific prevalence of HPV 16 to that of HPV 18). Estimated HPV 16/18-positive fractions in ICC, HSIL, LSIL and normal women were 69.7%, 45.5%, 32.2% and 4.6%, respectively. Examining HPV 16/18 positive fractions in ICC by geographical regions indicated that the fraction was lowest in Hong Kong (65.6%), higher in China mainland (69.6%), and highest in Taiwan (70.8%) (Figure 3). The HPV 16/18-psositive fraction in HSIL ranged from 30.6% in Hong Kong to 59.1% in the China mainland and in LSIL, it ranged from 31.4% in Hong Kong to 32.3% in the China mainland.

HPV type-distribution by geographic region in Chinese women with ICC
The prevalence ratio (PR) of HPV 16 and HPV 18 in ICC/HSIL were 1.7 and 1.2, respectively (Table 2).
HPV type-specific prevalence and prevalence ratios in women from 6998 China, stratified by grade of cervical lesion
ICC = invasive cervical cancer; HSIL = high-grade squamous intraepithelial lesions; LSIL = low-grade squamous intraepithelial lesions; CI = confidential interval
After 16/18, the six most common HPV types are HPV 58, 33, 52, 31, 59 and 45 in ICC so the cumulative prevalence of the eight HPV types was 88.3%. In order to keep consistent with that worldwide19, HPV 16, 18, 31, 33, 35, 45, 52 and 58 could account for 87.7% ICC in China.
DISCUSSION
HPV 16 was the predominant type in Chinese women with both cervical diagnoses of normal or abnormal, notably consistent with data worldwide. HPV 16/18 was estimated to account for 69.7% of all ICC and 45.5%, 32.2% and 4.6% in HSIL, LSIL and normal respectively, decreasing with the reduction of cervical lesion severity. After HPV types 16/18, HPV 58, 31 and 52 were the main HPV types in Chinese ICC women.
Overall HPV prevalence
In ICC, crude and adjusted overall HPV prevalence was 83.9% and 83.7%, respectively. These overall HPV prevalence figures are lower than the almost 99% prevalence detected using the most sensitive HPV detection methods. 4 Our findings are consistent with a previous meta-analysis of HPV prevalence among 2698 ICC cases in China mainland, Hong Kong and Taiwan where HPV prevalence was 83.7%, slightly lower than in other regions in Asia (86%–91%). 15 This review included a wide range of different PCR primers for HPV DNA detection, with a range of HPV detection capabilities, with results indicating higher HPV detection rates with GP 5+/6+ and MY 09/11 consensus primers than type-specific only primers. 11,15 With regard to the type of cervical specimen tested for HPV DNA, a higher HPV prevalence was found in biopsy tissues when compared with detection rates from the exfoliated cells, as previously noted in a systematic review of HPV DNA prevalence worldwide. 11
There was no significant difference in HPV DNA prevalence among mainland China, Hong Kong and Taiwan. As expected, given the development and use of more sensitive PCR-based assays in recent years, HPV prevalence in ICC specimens from China was higher in more recent publications, when compared with earlier study results. Our study results found a similar overall adjusted HPV prevalence for SCC and ADC significantly in Chinese women, confirming the conclusion that HPV is the primary cause of both SCC and ADC through different geographical areas worldwide. 6,15,17
With the decrease in degree of severity of the cervical lesion, overall HPV prevalence reduced dramatically: Overall, HPV prevalence of HSIL and LSIL was 77.4% and 76.2% in China, and the previous reported findings were 84.2% and 67.1% in a similar systematic review. 12,13 The number of studies with HPV DNA results among women with LSIL in China, however, was quite limited and thus additional data are required to more accurately estimate type-specific HPV prevalence in LSIL cases from China.
In women with normal cervical diagnoses or from population-based samples, HPV prevalence ranged from 9.3% in mainland China to 15.0% in Taiwan. A multi-centric IARC study 18 showed that the HPV prevalence of normal cytology women in Asia was ∼8%, similar to our reported figures here from mainland China, yet lower than that reported here from Hong Kong and Taiwan.
HPV type-specific prevalence
Findings from this meta-analysis showed that HPV 16 was clearly the most prevalent type in Chinese women. In women with ICC, HSIL, LSIL or normal cervix, type-specific HPV 16 prevalence was 58.7%, 35.4%, 21.1% and 3.3%, respectively; these results are similar to results of the previous meta-analysis in Asia that found HPV 16 prevalence was 52.4% in ICC, 33.1% in HSIL, 20.0% in LSIL and 2.6% in normals. 15 In this analysis, HPV 16 was more common than HPV 18 in SCC. In ADC, in contrast, HPV 18 was more common than HPV 16, consistent with previous reports. 11,15,19 The PR values of HPV 16 and 18 in ICC/HSIL were >1, suggesting that HPV 16 and 18 were more likely to progress to cervical cancer from HSIL than the other HPV types, supporting results from previous similar study. 13,20,21
Since the studies of Huang and Li, 22,23 a series of studies showed that HPV 58 and 52 were more prevalent among women with ICC in China. 24,25 Our analysis has confirmed that HPV 58 is a commonly found type in ICC in China, being the third most common type. Moreover, HPV 58 and 52 were the 2nd and 3rd most common HPV type in women with HSIL, LSIL and normal diagnoses in China. These results of the relative importance of HPV 58 and 52 as aetiological agents for cervical carcinogenesis in China are consistent with previous studies, 11,13–15,19,22 and suggest that the inclusion of this type in future generation HPV vaccines in China may be particularly important.
In ICC, hopefully the HPV 16/18 prophylactic vaccine could provide maximal 69.7% protection against ICC in China, lowest in Hong Kong (65.6%), slightly higher in China mainland (69.6%) and highest in Taiwan (70.8%). The previous analysis report that the HPV 16/18 fraction was ∼67% in Asia, and slightly higher in more developed (72%–77%) than in less developed (65%–72%) regions. After 16/18, the six most common HPV types are HPV 58, 33, 52, 31, 59 and 45 in ICC that the cumulative prevalence of the eight HPV types was 88.3%. Two similar meta-analyses, worldwide and in Asia, reported that the HPV 16, 18, 31, 33, 35, 45, 52 and 58, which are the same most eight common HPV types in all world regions could account for 88.8% ICC worldwide and 86.4% in Asia. This analysis showed that these eight HPV types could account for 87.7% ICC in China and it was suggested that they be included in the future generation HPV vaccines.
These reported findings are the first to provide a comprehensive review of HPV DNA prevalence in the wide range of cervical diagnoses (ICC, HSIL, LSIL and normals) in China. Despite study strengths of a meta-analysis including a large sample size and extensive review of the Chinese papers, several limitations should be considered. The subjects included in this analysis are not necessarily representative of distribution of HPV-related burden of cervical disease in China, particularly that of mainland China. The burden of cervical cancer in mainland China is far higher than that in Taiwan; however, ∼40% of ICC cases included are from Taiwan. Moreover, few studies were available from mid-West China, an area with a higher cervical mortality and a higher proportion of rural residents and women with lower economic level and health infrastructure when compared with Eastern and Southern China. 26,27 In fact, most ICC cases were from Southern China, including Sichuan, Guangdong Provinces and Shanghai, which have been found to have a generally lower cervical cancer burden. Although a population-based survey in Shiaxi and hospital-based study in Shaixi and Jiangxi Province was included in this analysis, sufficient data on HPV prevalence was not available in many geographical areas including Gansu and Xinjiang provinces. Thus, HPV DNA prevalence may have been slightly underestimated in women with ICC or those in population-based studies from samples included in this review, and HPV type specific distribution could not be truly representative of entire China due to limited geographic coverage.
HPV prevalence estimates in our study may be slightly underestimated (83.7%) because HPV DNA detection methods were included that may have been relatively less sensitive, and thus some type-specific HPV positivity has been missed. Further, HPV types included in multiple infections were counted in analyses to contribute to both HPV 16 and to HPV 18-positive, which could have potentially increased the attributable fraction of HPV 16/18-positive ICC cases. However, if all negative cases were retested with more sensitive HPV DNA detection methods, the HPV 16/18-positive fraction would likely increase.
In summary, this meta-analysis shows that the most common HPV types in Chinese women with and without cervical abnormality are HPV 16, 18, 58, 33 and 52. The estimated HPV 16/18-positive fraction was averaged to ∼69.7% in ICC, 45.5% in HSIL, 32.2% in LSIL and 4.6% in women with normal cervical findings. HPV 16, 18, 58, 33, 52, 31, 35 and 45, consistent worldwide, could account for 87.7% ICC in China and are considered for future inclusion for the development of new generation HPV prophylactic vaccines in China.
Footnotes
ACKNOWLEDGEMENTS
We thank GlaxoSmithKline for partial support of this work. We are grateful to those authors who made detailed data available from their published studies.