
Abstract
Women attending a dedicated medical gynaecology and family planning referral clinic for women with HIV were surveyed using a standard questionnaire about their knowledge and attitudes to post-exposure prophylaxis after sexual exposure (PEPSE) and emergency hormonal contraception (EHC). Eighty percent of them had not heard of PEPSE, but once informed about it, 86% said they would inform a partner about it. Less than 10% had any idea of the duration of effectiveness. Seventy-three percent of the women knew about EC and 45% of them had used it previously. Ninety-eight percent of them would use it in the future if necessary. Eighty percent of them knew its period of effectiveness. There is a clear need for information about PEPSE, which needs to be delivered around the time of HIV diagnosis and reinforced later. Some women will need help in discussing it with HIV-negative partners.
Introduction
Administration of antiretroviral drugs as post-exposure prophylaxis after sexual exposure (PEPSE) to HIV is thought to reduce the risk of acquisition of HIV infection.1,2 For PEPSE to be an effective intervention, it needs to be promoted and made available to ‘at risk’ groups. To limit the transmission of HIV they need to be willing and able to inform partners of the availability of PEPSE.
For HIV-positive women planned pregnancy is vital in order to reduce the risk of HIV transmission to the child. Teratogenic effects of antiretrovirals on the foetus and the physical and psychological effects of abortion are also the possible sequelae of unplanned pregnancy. Hence, these women must have an easy access to contraceptive services and emergency hormonal contraception (EHC).
Objective
To study the level of awareness and use of PEPSE and EHC in women attending a dedicated medical gynaecology and family planning referral clinic for women with HIV.
Method
All patients attending the referral clinic in the first six months of 2006 were surveyed using a standard questionnaire about their knowledge and attitudes to PEPSE and EHC.
Results
A total of 100 patients were seen of whom 83% were black African, age distribution 20–29 years, 10%; 30–39 years, 68%; 40–49 years, 20%; over 50 years, 2%; 76% were on antiretroviral therapy.
Eighty out of one hundred (80%) patients had not heard of PEPSE. Of the remaining 20, only 13 had some idea of where it was available. Nine thought it would have to be taken within 72 hours after sexual intercourse to be effective. Once informed about PEPSE, 78/91 (86%) said they would inform a partner about it, 3/91 (3%) would not, while 9/91 (10%) did not know. The question did not apply to nine patients.
Seventy-three out of one hundred (73%) of the women knew about EHC, 60/100 (60%) patients knew of between one and four sources of EC. The various sources were genitourinary (GU) medicine clinic (10), pharmacy (32), family planning clinic (17), general practitioners (GP) (34) and accident and emergency department (4). Thirty-three out of seventy-three (45%) of the women had used EHC previously, but only 10 recalled where they had obtained it, sources being GU medicine clinic, family planning clinic, pharmacy and GP. Twenty-three thought it was easy to obtain while three did not, two of them because they had to pay for it!
On the period within which EHC was effective 60/73 patients thought <72 h, one >72 h, the rest did not know.
Eighty-seven out of 89 (98%) patients would use EHC in the future, if the need arose. In 11 cases the question was not applicable because, for instance, a patient might be seeking to conceive or had had an intrauterine contraceptive device fitted. Only two patients did not know (Figure 1).
Levels of awareness of post-exposure prophylaxis after sexual exposure, and of emergency contraception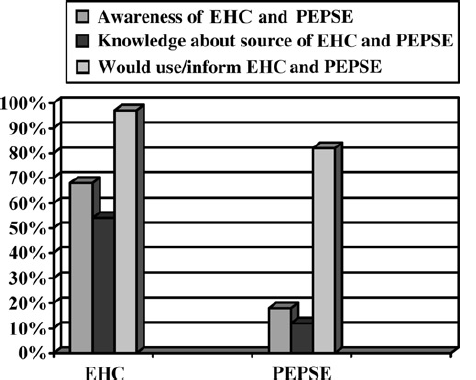
Discussion
Post-exposure prophylaxis after sexual exposure
The finding that 80% of the women had not heard of PEPSE is disturbing but not surprising. De Silva et al. 3 found just under half of male (MSM) respondents to a questionnaire were not aware of PEPSE despite an awareness campaign by the Terrence Higgins Trust and numerous publications in the general press around the time of survey. HIV in women has not attracted such general publicity. There is little published data on the awareness of PEPSE in HIV-positive women. Only five patients had informed a partner about PEPSE. Eighty-six percent of women said that they would inform a partner about PEPSE, if they had unprotected sex or condom accident with a partner who is HIV-negative or status unknown. Once they knew about PEPSE, 10% did not know if they would inform a partner and 3% would not. The concerns of such women would have to be tackled in any further intervention.
Emergency hormonal contraception
Seventy-three percent of the women knew about EHC, a figure somewhat less than that obtained by Mathew and Urquart 4 (75%) who surveyed women in a termination of pregnancy clinic elsewhere in the UK; 33/73 (45%) had used EHC. In our population, factors limiting its use may be related to knowledge about where to access EHC (only 60% could name one or more sources) and cost, specifically mentioned by two patients.
When questioned on the duration of effectiveness, 82% of these women had a good knowledge. They tended to be those who knew about one or more sources of EHC and had used it previously.
Once given information on its effectiveness and availability, 65/67 (97%) would use EHC in future, if the need arose.
Conclusion
There seems to be little information about awareness of PEPSE among the sample of HIV-positive women considered in this article. There is a clear need for information about PEPSE, which needs to be delivered around the time of HIV diagnosis and reinforced during subsequent interactions with health care professionals. Some women need additional help around issues of disclosure to allow partners to access all forms of PEPSE.
There is also a clear need for more education about EHC for HIV-positive women. This information has to include where to access emergency contraception and its duration of effectiveness.