
Abstract
Summary
This study aims to measure indicators of HIV-related stigma among students of high schools in the North West of Libya. The results will be part of baseline data and evaluation of the impact of successive interventions. Understanding the behaviour of risk groups in a society, such as young people, is essential in order to draw effective prevention strategies. Behavioural surveillance surveys have been shown to make an important and useful contribution to informing the response to HIV. This study was part of a large Knowledge, Attitude, Beliefs and Practice survey. A self-administrated questionnaire method was used. The response rates were high (83–92%). Despite high level of stigma shown by both boys and girls in the study, 91% of students supported providing free care to HIV infected individuals. The HIV intervention programmes for young people should operate within a comprehensive strategy to combat HIV/AIDS. The stigmatizing and the discriminatory perceptions of HIV infected individuals should be addressed as part of the education campaign.
Introduction
Despite the reported relatively low HIV prevalence; Libya is facing a growing HIV epidemic. Available evidence reveals trends of increasing HIV infections especially in younger age groups. 1 The main mode of HIV transmission in the North-West of Libya is injecting drug use, although unprotected sexual contact is becoming an increasingly important factor and it is the dominant mode of transmission in the rest of the country. 2 The National AIDS Programme (NAP) in Libya figures show that at the end of 2006, a cumulative total of approximately 10,000 HIV infections had been reported and 90% of adult infections are the result of injecting drug use. A national survey conducted in 2004–2005 showed that HIV prevalence among the general population had reached 0.67% in Alkoufra governorate in the south-east of the country, 0.4% in Tripoli compared with national prevalence of 0.13%. 3
Libyan culture is strongly influenced by Islamic religious teaching. The stigma attached to HIV/AIDS is particularly strong. An essential component of efforts to prevent new HIV infections is the use of voluntary HIV counselling and testing especially among members of population at risk.4–6 To increase the number of persons at risk of HIV who receive voluntary counselling and testing services, barriers to these services must be identified and removed. Libya appears more willing to acknowledge and tackle the epidemic. This is encouraging exception to what appears to be a general pattern of official denial in the region. While the HIV epidemic is now acknowledged and openly debated and some public health campaigns have been carried out, Government-sponsored effective prevention is speedily needed, designed to target vulnerable risk groups including young people.
Aims and Objectives
This study aims to measure the indicators of HIV-related stigma among students of high schools in the North-West of Libya. This study is conducted in collaboration with the Libyan NAP. The results will be part of baseline data to identify specific areas where health education needs to be intensified for HIV/AIDS prevention and evaluation of the impact of successive interventions.
Methods
A self-administrated questionnaire study was undertaken between August 2004 and August 2005. Data were analysed in Statistical Package for the Social Sciences (SPSS) (SPSS Inc, Chicago, IL, USA) using descriptive and inferential statistics. Non-parametric tests were used to determine whether the difference between explanatory variables reaches statistical significance: Mann-Whitney test for two unrelated variables and Kruskal–Wallis test for three or more variables. For this study, a P value ≤0.05 was considered statistically significant.
The design of the questionnaire was based on the intervention module: Learning for life: a guide to family health and life silks education for teachers and students. 7 The variables included in the questionnaire were informed by a series of workshops with the relevant health-care professionals at NAP in Tripoli. The questionnaire was designed in Arabic and adopted to Libyan norms and culture. This paper deals with the analysis of the parts of the questionnaire covering stigma against HIV infected individuals. The data collected were categorical or ordinal (Likert scale) data.
Subjects
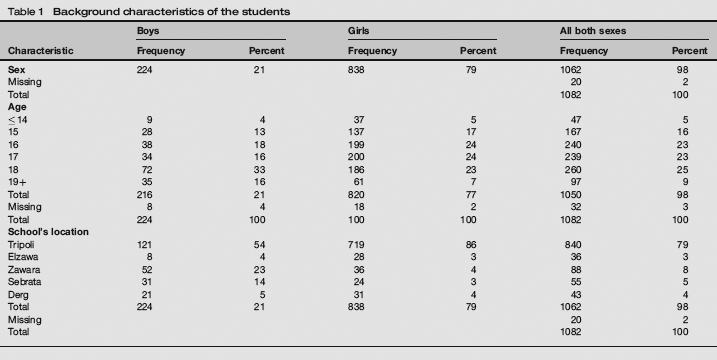
A total of 1082 were recruited from five cities in the North-West of Libya. The cities selected included the large cosmopolitan capital city of Tripoli, the relatively large city of Elzawa, and the relatively small cities of Sebrata, Zawara and Derg. All cities selected except Derg are located on the coast of the Mediterranean Sea. Derg is more rural and located in the desert within the province of Ghadames. Within each city, the schools were selected using the education authorities register of high schools. This convenience sampling was subject to the permission granted by the education authorities. Ten public, single sex high schools were selected; seven schools from Tripoli and one school from each other city. Every student who appeared to the site during the study visit was included in the sample. Informed consent of the subjects was obtained. Confidentiality and anonymity were explained and guaranteed to all participants. The questionnaires were sealed in individual envelopes and kept in safe storage until they were opened off-site. The age distribution shows that 84% of the respondents were aged 15–18 years (range 13–30). The overall mean is 17 with standard deviation of 1.49.
Results and Discussion
This is the first study of its kind conducted in Libya. Literature searches showed no similar published surveys have been conducted with young people in the Arab world. The response rates were exceptionally high (83–92%). The background characteristics of the sample population is summarized in Table 1.
Background characteristics of the students
Transmission of HIV infection
The listed statements in this part explore the knowledge of HIV transmission and suggest stigmatizing attitudes towards HIV-infected individuals. Participants were given a list of statements and were asked to tick against each statement; true, false or do not know. As the statements were not factually correct, the score was therefore reversed, i.e. answers ticked as correct were given 0 score. Answers ticked as false or do not know were given 1 point. The maximum score of this part is 3 points. The participants were asked: You may catch HIV infection by?
Use of public toilets Getting near to an HIV-infected individual while sneezing or coughing Looking after an HIV-infected individual
This part of the questionnaire received a high response rate of 92%. This may be attributed to the fact that they were testing knowledge, which is less personally revealing and, therefore, less threatening than questions, which probe behaviour and attitudes. A total of 450 (42%) agreed and 530 (49%) did not agree or did not know that they may catch HIV infection by the use of public toilets. Three hundred and thirty or 31% agreed and 635 or 59% did not agree or did not know that you may catch HIV infection by getting near to an HIV-infected individual while sneezing or coughing. This compares with 70% of Greek students identifying that HIV cannot be transmitted by coughing or sneezing and 48% by using public toilets. 8 Three hundred and twenty-seven (327) or 30% agreed and 625 or 58% did not agree or did not know that you may catch HIV infection by looking after an HIV-infected individual. Six hundred and thirty-two or 64% of respondents recognized that all or two out of the three listed statements do not expose to the risk of HIV infection. No significant difference was found between boys and girls with a median score of 2 (P value = 0.994). The median score for the students in Tripoli, Sebrata, Elzawa and Zawara was 2. The data suggest that students from Zawara performed less well with a median score of 1 and students from Derg had the highest median score of 3 (P value = 0.000).
Stigma against HIV-infected individuals
Participants were given ‘right’ and ‘wrong attitude’ statements in terms of stigma towards HIV patients. Students are asked to tick against each statement on Likert scale from 1 to 5. The ‘right attitude’ statements were scored as follows: 1 is strongly disagree, 2 is disagree, 3 is unsure, 4 is agree and 5 is strongly agree. In the ‘wrong attitude’ statements, the coding was reversed, where 1 is strongly agree, 2 is agree, 3 unsure, 4 is disagree and 5 is strongly disagree.
The participants were asked: Banning an HIV-infected individual from work is a form of stigma? In this question 1 is strongly agree and 5 is strongly disagree.
Two hundred and seventy-three or 25% strongly agreed and 186 or 17% of students agreed, 124 or 12% strongly disagreed and 123 or 11% disagreed and a further 200 or 19% were unsure that barring HIV infected individuals from work is a from of stigma. The overall median score was 4 (agree). Table 2 shows the results of the attitudes of boys and girls. Girls were more unsure than boys with median score of 3 (unsure), boys on the other hand seem to show less stigma with median score of 4 (agree) (P value = 0.012). Students from Derg, Sebrata and Zawara had similar attitude with median score of 4 (agree). Students from Tripoli and Elzawa were less sure with median score of 3 (unsure) (P value = 0.219).
Attitude of the boys and girls to banning HIV infected individuals from work

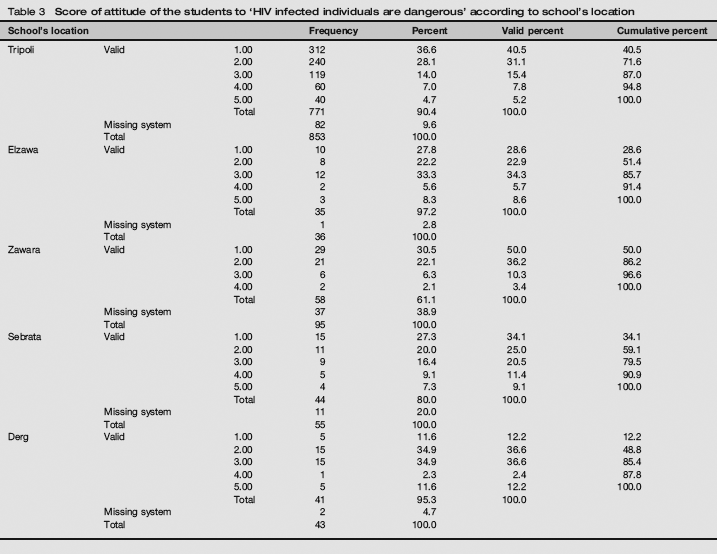
The participants were asked: HIV-infected individual is dangerous to others? In this question 1 is strongly agree and 5 is strongly disagree.
The students’ response to this question suggests a high level of stigma against HIV infected individuals with an overall median score of 2 (agree). Three hundred and seventy-one or 34% strongly agreed and 295 or 27% of the students agreed that HIV infected individual is dangerous to others. One hundred and sixty-one or 15% were unsure, 70 or 7% disagreed and only 52 or 5% strongly disagreed. The median score is equal for boys and girls at 2 (agree). Despite girls seem to show more stigma than boys but there seems to be no large difference in the attitude of boys and girls (P value = 0.060). Table 3 outlines the distribution of the scores of the students in the five cities. Surprisingly students from the more rural town of Derg seem to show less stigmatizing attitude. Table 3 suggests that more students from Derg were unsure with a median score of 3 and students from Sebrata, Zawara, Tripoli and Elzawa showed similar attitude with median score of 2 (agree) (P value = 0.000).
Score of attitude of the students to ‘HIV infected individuals are dangerous’ according to school's location
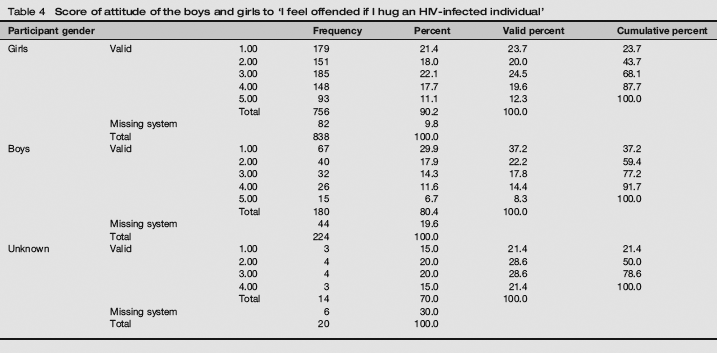
The participants were asked: I feel offended if I hug an HIV-infected individual? In this question 1 is strongly agree and 5 is strongly disagree.
Two hundred and forty-nine (249) or 23% of the students strongly agreed, 195 or 18% agreed and 221 or 20% of the students were unsure that they might be offended if they hugged an HIV-infected individual. One hundred and seventy-seven or 16% disagreed and 108 or 10% of the students strongly disagreed. However the overall results suggest that the majority of the students were unsure with an overall median of 3 (unsure). Table 4 suggests that boys felt more offended with median score of 2 (agree) while girls were less sure with median score of 3 (unsure) (P value = 0.000). There seem to be no large differences of the attitudes of the students from the different cities. The median score of the attitude of the students from Tripoli and Derg is 3 (unsure), from Sebrata, Elzawa and Zawara is 2 (agree) (P value = 0.142).
Score of attitude of the boys and girls to ‘I feel offended if I hug an HIV-infected individual’
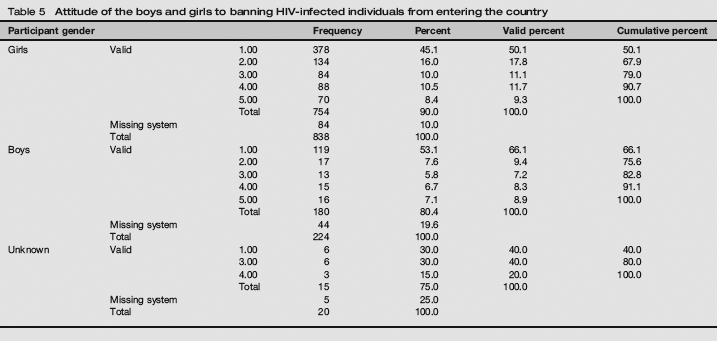
The participants were asked: The authorities should ban HIV-infected individuals from entering the country? In this question 1 is strongly agree and 5 is strongly disagree.
Five hundred and three or 47% strongly agreed and 151 or 14% agreed and 103 or 10% of the students were unsure that the authorities should ban HIV-infected individuals from entering the country. One hundred and six (106) or 9% disagreed and 86 or 8% of the students strongly disagreed. The results suggest a high level of stigma with an overall and equal median score for boys and girls of 1 (strongly agree). This compares with 45% of Scottish students who agreed that all HIV infected individuals should be banned from entering the country. 8 Table 5 suggests that more boys than girls felt that HIV infected individuals should be banned from entering the country (P value = 0.001). results also suggest that there is no large difference of the attitudes of the students from the different cities with equal median score in all cities at 1 (strongly agree) (P value = 0.910).
Attitude of the boys and girls to banning HIV-infected individuals from entering the country
Participants were asked about their Attitude towards Providing Free Care to HIV-Infected Individuals. The participants were asked: Free health care should be provided to all HIV-infected individuals? In this question 1 is strongly disagree and 5 is strongly agree.
Despite the high level of stigma demonstrated 735 (68%) strongly agreed and 125 (12%) of the students agreed that medical care should be provided free of charge to all HIV-infected individuals. Fifty-five (55) students or 5% were unsure, 18 or 2% strongly disagreed and 15 or 1% of the students disagreed. Boys and girls have equal median scores of 5 (strongly agree) (P value = 0.092). The results do not suggest large differences in the attitudes of the students from the different cities with a median score of 5 (strongly agree) (P value = 0.711).
Conclusions
The attitudes and beliefs of the students should be interpreted and explained within the context of the Islamic faith and Libyan culture. This study demonstrates that there is high level of stigma towards HIV-infected individuals. In a conservative Muslim society where most practices associated with HIV infection are either forbidden or condemned, this is not surprising. Free health care, including drugs, is provided free of charge to all Libyan citizens. It is noteworthy that, despite the high level of stigma, the vast majority of students felt that free care should be provided to HIV-infected individuals. This may be explained by the fact that compassion, kindness and mercy are highly valued virtues in Islam, especially towards the sick, the weak and the old, but the religious message that is frequently dispensed is that HIV is equated with ‘a curse’ and those who lived with it are ‘sinners’. There is a need to shift the attitudes from ‘punishment’ towards positive Islamic values. Religious leaders are essential in a successful response to HIV/AIDS, as they have legitimacy and a durable presence in local communities. They help shape social values and norms, which is critical to ending stigma and discrimination related to HIV/AIDS. They are also well positioned to influence public attitudes and national policies related to HIV/AIDS. The provision of care and the above virtues should apply equally to HIV infected individuals, without judgement. This message was reinforced in the final communiqué of the conference of the eminent Muslim scholars on HIV/AIDS in Cairo in 2004. 9
Schools have been successful in helping young people acquire the knowledge, attitudes and skills needed to avoid infection. Education, when it is appropriately planned and implemented, is one of the most viable and effective means available for stopping the spread of HIV infection.10,11 Education represents the best opportunity not only for delivering crucial information on HIV/AIDS, but also for chipping away at the ignorance and fear that perpetuate stigma and discrimination. An effective strategy for preventing HIV/AIDS among youths is making sure that all children receive formal education in a safe culture and gender-sensitive school environment. Measuring attitudes and the correlates of stigmatizing attitudes is important for guiding efforts to remove's barriers to HIV prevention. HIV prevention for young people should be implemented within the context of community mobilization and policy reform in the Libyan society to de-stigmatize HIV infection and treat HIV-infected individuals with dignity and respect. Negative attitudes, discrimination and stigmatizing of HIV-infected individuals should be addressed as part of the education campaign.
This study helps to inform a baseline against which intervention may be benchmarked. Evaluation and monitoring of HIV/AIDS educational programmes should be an on-going process. Since the results of the study cannot be generalized to other similar populations, other groups of young people should be investigated in order to have a better picture of the Libyan context during this period of the expansion of the HIV/AIDS epidemic. Further research should also be undertaken to investigate the differences in attitudes and beliefs of boys and girls, and why students from Zawara performed less well than the students from the other cities did.
Footnotes
Acknowledgement
This study was supported and conducted by the National AIDS Programme in Libya. No other grants were provided.