
Abstract
Summary
Current genitourinary medicine patients (202) and potential future patients (542) completed a questionnaire-based survey to determine their preference for obtaining test results, their acceptability of including a named infection on contact slips and to report expectations about the acceptable length of an appointment. Overall, most respondents (78% [n = 582]) felt it unacceptable to be only contacted if their results were positive (‘no news is good news’). In the clinic, a majority preferred a contact slip to be coded (68% [n = 137]), in the general public views were balanced. Significantly, more people in the general population expected an appointment to last no longer than 30 min (32% [n = 173] cf. 10% [n = 21], P < 0.001). A clear preference was expressed to receive sexually transmitted infection test results even if they are negative. Telephone and face-to-face contact were most popular with relatively few choosing mobile telephone text messaging or email as their preferred option.
Introduction
Patient perspectives aid sexual health-care planning and the need to modernize genitourinary (GU) medicine departments has been a widely recognized priority owing to a significant increase in demand for services. 1 Strategies to achieve the 48 h waiting time target, 2 and the implementation of payment by results for GU medicine clinics has also led to departments needing to identify more cost effective ways of managing the follow up of patients. 3
The implementation of ‘no news is good news’, where patients are only contacted if their tests reveal a positive result, has been introduced in many clinics to reduce the number of patients requiring follow up, 4 but may not necessarily be acceptable to the patient. 5 Newer technologies have also been suggested as an appropriate way to automate the delivery of results, e.g. text messaging, telephone messaging, internet.6–8 Concerns around confidentiality and interpretation of results when these technologies are used have, however, been raised. 9
Determining patient preferences for contacting their potentially infected partners may improve the success of partner notification, reduce re-infection rates and prevent onward transmission of disease. 10 Many sexually transmitted infection (STI) clinics in the UK give infected patients a ‘contact slip’ to pass on to their partner, who is then asked to bring it with them to a GU medicine clinic. The contact slip usually contains the index patients case notes number, address of the clinic and a code corresponding to the index patient's diagnosis, which ensures that the partner gets appropriate testing and treatment. It has been suggested that including the specific diagnosis on the contact slip may increase the number of partners presenting for STI screening. 11
Patients views remain an important input to the design of sexual health-care services, 12 including the measurement of satisfaction with new initiatives.5,13 This study obtained views from STI clinic patients and a community sample on alternative ways of providing results to patients, methods of partner notification and expectations on how long a clinic attendance for STI screening should last.
Methods
Participants between the ages of 16–25 were recruited from a city centre STI clinic and from households within the Birmingham area as reported previously.
14
A standardized questionnaire, developed by sexual health clinic research staff and an external market research company, was used to interview each participant. This included an assessment of preferences in three different domains:
options for obtaining test results; use of a specific infection name (rather than a code) on contact slips which patients would give to their potentially infected partners to facilitate partner notification; expectations about the length of time spent in clinic during a first consultation for STI screening.
We collected data specifically regarding the acceptability of only being contacted if results were positive (‘no news is good news’) and whether the acceptability of this method changed if it led to a reduction in clinic appointment waiting times from 2 weeks to 1 week. Methods of receiving results were ranked in order of preference and tabulated against patient access to the internet.
Demographic data and previous attendance at a STI clinic were recorded.
As previously described, the study was designed to provide 80% power to detect a significant odds ratios of 1.55 or 2.15 when the prevalence of an outcome measure was 50 or 10%, respectively, requiring minimum sample sizes of 500 community and 200 clinic interviewees. 14
The response to each question between the two samples (clinic and community) was compared. Where these differed significantly then both are reported, otherwise the overall reporting is presented. The χ 2 test is used for univariate testing comparing independent groups, and χ 2 test for trend where the factor is ordered. McNemar's test is used to compare the frequency of responses to two items within the questionnaire, and the binomial test is used to test whether one response option is more commonly reported than another (removing those with no preference). Multivariate analysis is based on multiple logistic regression. All analysis is performed in Stata 9.
Results
The response rate of those approached in the clinic was 92% (202/220) and 43% (542/1260) for the community sample. The demographics of the study population are as previously reported. 14
‘No news is good news’ approach to giving results
A large majority of respondents reported that it was unacceptable to only be contacted with results if their diagnosis was positive (78% [n = 582]). The community sample particularly disliked this approach (unacceptable to 81% [n = 439]). No significant difference in responses was found by age, ethnicity or gender although patients attending for a follow-up appointment at the clinic found this approach slightly more acceptable (Table 1).
Acceptability of only being contacted if STI test results are positive
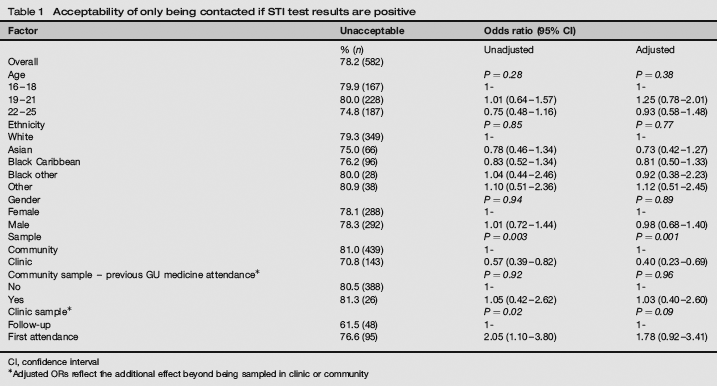
CI, confidence interval
Adjusted ORs reflect the additional effect beyond being sampled in clinic or community
If the introduction of ‘no news is good news’ would result in a reduction in clinic appointment waiting times then 58% (n = 430) still felt it unacceptable to only be contacted with results if their diagnosis was positive. However, a greater difference in the level of acceptance was reported between the clinic sample and the community sample (unacceptable in 33% [n = 66] and 67% [n = 364], respectively, P < 0.001). Those patients who were attending for a follow-up appointment were particularly likely to accept a ‘no news is good news’ approach if waiting times were reduced as a consequence (unacceptable in 62% [n = 48] reducing to 17% [n = 13], P < 0.001).
Preferred options for receiving STI results
Telephone (40% [n = 295]) and face-to-face consultation (41% [n = 304]) were the most popular methods for receiving STI test results (excluding HIV). Seventy-five percent (n = 560) of interviewees had access to the internet. This had little influence on responses regarding the face-to-face method to receive their STI results, but those without internet access were more likely to choose the telephone than those with internet access (47.8% [n = 88] cf. 37.0% [n = 207], P = 0.009).
Overall, less than 5% of interviewees reported their first choice for receiving test results to be by mobile telephone text messaging, email or the internet. Preferences for receiving STI test results did not vary by age, ethnicity or gender (data not shown).
When the STI results included an HIV test the pattern of preferences remained similar but using the telephone decreased in popularity (40% [n = 295] to 27% [n = 204], P < 0.001), face-to-face contact was more popular (41% [n = 304] to 60% [n = 443], P < 0.001) and sending results by post was less acceptable (16% [n = 116] to 9% [n = 69], P < 0.001).
Inclusion of a named infection on the contact slip
Respondents expressed a slight preference that the contact slip given to their sexual partners should be coded rather than name a specific infection (45% [n = 337] cf. 36% [n = 267], P = 0.005). Preferences reported differed greatly between community and clinic samples (P < 0.001), in particular preference for coding was greater in clinic than community (68% [n = 137] cf. 37% [n = 200]) (Table 2). Preferences differed according to age and ethnicity, but not after adjustment for other factors.
Preference for description of diagnosis on contact slip
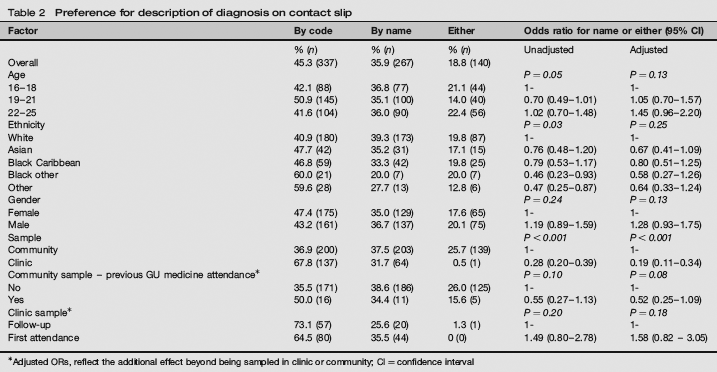
Adjusted ORs, reflect the additional effect beyond being sampled in clinic or community; CI = confidence interval
The likelihood of passing on a contact slip to their partner was unchanged for the majority of the sample population (61% [n = 426]) whether or not it named a specific infection – 18% (n = 122) were more likely to pass it on and 18% (n = 127) less likely to do so.
Respondents in the community had significantly different expectations regarding the length of time a consultation for an STI screen would take compared with those who were attending the clinic. Most patients expected an appointment to last between 1 and 1.5 h. However, significantly more people in the community sample expected an appointment to last no longer than 30 min (32% [173] compared with 10.4% [21] of the clinic sample P < 0.001).
Discussion
Our results strongly suggest that patients prefer to receive their STI test results by telephone or via a face-to-face consultation with few, when given the choice, wanting to use mobile telephone text messaging, email or the internet. When HIV results were included, 60% of individuals preferred to receive these in person. Only a small minority found the ‘no news is good news’ approach of only contacting them with positive test results acceptable. Most clinic attenders (68%) preferred to give a coded contact slip, rather than one naming a specific diagnosis, to their partners to inform them of the need to attend for testing and screening. Those in the community who had not attended a clinic previously were evenly split as to whether the contact slip should name the infection concerned (36 against cf. 39% for). The majority of individuals who have not previously undergone a STI screen expect the attendance to last no more than 1 h.
The survey was undertaken at a time where many STI clinics had routine waiting times of several weeks, 15 which may have influenced the response of those clinic attenders who had already experienced long delays in being seen. This may have made alternatives to improve access, such as ‘no news is good news’, more attractive. Even allowing for this, patients and potential patients expressed a clear preference to receive their results explicitly even if they were negative, which is in accordance with a previous report. 5 Although ‘no news is good news’ may free clinic resources, reduce costs and improve waiting times it remains generally unacceptable to patients.
Effective and efficient communication with patients to provide their results is a core component of providing an STI testing service. Text messaging, email and the internet provide new and potentially cheaper ways of sending results to patients but proved unpopular when patients were given the alternative of telephone contact or receiving results in person. Previous studies have reported high levels of acceptance for these new technologies.6,7,9 It is possible that although initially apprehensive, patients are happy with these newer technologies once they have been educated in their use and had experience of them. However, being able to ask questions and interact with someone on the phone or face-to-face is valued by patients and remains an appropriate option for many of them (Brown L, Using Focus Groups to Provide Patient Input to Sexual health-care Delivery,. in preparation).
The information provided to an index patient may influence the likelihood of potential partners attending for testing and treatment. 16 Historically, STI clinics in the UK have used a contact slip with a code, which is recognizable to other clinic providers, but not to the patient's partner, in order to protect confidentiality and reduce embarrassment. Including a named infection on the contact slip has been reported to be acceptable and be associated with improved outcomes. 11 Although many of those surveyed from the community in our study found this approach acceptable, it was less so for clinic patients who preferred a coded contact slip. Responding to patient preferences for contacting their partner influences their likelihood of passing on information and has the potential to improve contact tracing rates. 10
It seems appropriate to ensure that patients are given a realistic expectation of how long a STI screen will take when they book an appointment. Our data suggest that there is considerable variation in patient expectations, which will in reality depend on the underlying diagnosis, availability of rapid diagnosis technologies, type of appointment and availability of staff and efficiency of the clinic.
The strengths of the study were the inclusion of a large number of STI clinic attendees and a general population sample, which improves the generalizability of the findings. Interviewees were also asked to choose from a number of options in each area of interest, rather than just indicate whether they wanted access to a new option or service, which reflects the choices that providers have to make in a limited resource environment. However, assumptions made for certain aspects of service delivery, such as the specific impact on waiting times, may not represent other clinic settings. Also it remains unknown whether stated preferences will reflect actual behaviour.
Assessing how best to deliver sexual health care involves understanding the demography of the population, which the clinic serves. 1 As new technology becomes available, it is often appropriate to utilize it but patients should have a choice in how their results are delivered, and currently many still prefer the telephone and face-to-face consultation.
Footnotes
Acknowledgements
We thank Rebecca Newson for her assistance in recruiting patients for this study. This study was supported by Heart of Birmingham tPCT. Ethical approval was obtained for the study.