
Abstract
Summary
The aim of this study was to investigate the incidence of reinfection with sexually transmitted infection (STI) and its possible predicting factors among patients reattending a department of genitourinary (GU) medicine. The method included a retrospective study on consecutive patients re-screened for STI in a busy department of GU medicine between January 1996 and April 2005. Cox regression model was used to investigate the association of age, gender, sex group, previous STI, counselling for an STI on the last attendance, number of sexual partners in the previous attendance episode, condom use and the number for partners with whom they had unprotected sex, with STI at current screening. The results show that 302 consecutive patients with more than two attendance episodes were included in the study. Patients were mostly women (92%), younger than 35 years (80%) and heterosexual (98%). At baseline, 70 (23%) patients had STI. The incidence density of STI at the end of follow-up period was 15.69/100 person-years. Testing positive for an STI was associated with age younger than 25 years (hazard ratio 2.70 [95% confidence interval 1.70–4.57]; P = 0.000). In conclusion, our study confirmed the improvement in access to GU medicine services, encouragement of patients with an STI for re-screening on regular basis and use of novel STI counselling strategies, especially for younger patients may reduce the incidence of subsequent STI.
Introduction
The increasing prevalence of most sexually transmitted infections (STI) in the UK over the recent years has been alarming. 1 Facilitation of patients’ screening and treatment of infected patients and their partners may reduce the incidence of STI. With increase in public awareness of STI, the proportion of patients reattending departments of genitourinary (GU) medicine may increase. A proportion of those patients may continue with high-risk sexual behaviour.
Patients with STI are routinely counselled for safe sexual behaviour to prevent their reinfection in GU medicine clinics. Little data, however, are available to support the success of routine counselling provided at GU medicine centres in reducing the rate of high-risk sexual behaviour and consequent STI. 2 The incidence of STI among patients re-screened at GU medicine centres may add some light on the extent of success of counselling.
The aim of the present study was to investigate the incidence of reinfection with STI and its possible predicting factors among a group of patients reattending a busy department of genitourinary medicine.
Methods
Study population and setting and clinical policy
This was a retrospective study on consecutive patients who attended the Department of Genitourinary Medicine at Whittall Street Clinic, Birmingham, UK for more than one episode between January 1996 and April 2005.
Patients were routinely offered screening for Chlamydia, gonorrhoea, syphilis and HIV. Screening for hepatitis B was offered to all men who have sex with men (MSM) routinely. Women were also screened for Trichomonas vaginalis.
Those testing positive for any of the STI were counselled by ealth advisors for contact tracing and safe sexual behaviour.
Clinical policy and laboratory methods
A sexual history was obtained from all patients accepting STI screening. After genital examination, tests for different STI were carried out.
Presence of Chlamydia trachomatis was investigated in male urethral and female endocervical materials. Before 1999, culture was the method of detection of chlamydial infection. ProbTec® (Becton Dickinson, UK), a strand displacement assay method has been used since 2001.
Gonococcal infection was investigated in urethral material obtained from men who have sex with women, females and MSM, in endocervical material of all women, and in endo-rectal material in MSM and women with history of receptive sexual intercourse. Oro-pharyngeal material of all MSM and heterosexual patients with genital gonorrhoea was screened for gonococcal infection. Culture method using modified New York City culture media for inoculation of material from the above sites was used to diagnose gonococcal infection.
Presence of more than five polymorphonuclear cells in high power field (×1000) of microscopic examination of gram-stained urethral material of men was considered as non-specific urethritis (NSU) if those patients tested negative for gonococcal or chlamydial infections.
Women with history of abdominal pain or pain during sex underwent a bi-manual examination for exclusion of pelvic inflammatory disease (PID). Patients with cervical excitation or adnexal tenderness were treated for PID.
Wet mount slide of material obtained from vaginal fornices was examined under microscopy for the presence of T. vaginalis.
Clinical diagnosis of genital herpes was confirmed with culture method.
Serum samples were obtained to test for the presence of syphilis antibody with an enzyme immuno-assay (EIA) method. Positive samples were subsequently tested with a profile of different tests for confirmation.
Serum samples were obtained to test for the presence of HIV antibody with an EIA method. Positive samples were confirmed with additional EIA and Western blot tests as per National guidelines. Before 2002, HIV testing was carried out on patients’ request and was offered to those deemed at high risk of HIV. Since April 2002, HIV testing has been offered to all patients requesting screening for STI.
Serum samples were tested for the presence of hepatitis B surface antigen and hepatitis B core antibody.
Statistical analysis
The list of patients was retrieved from the department's database. Case notes of all patients identified with more than one new-episode attendance at the Department were inspected. Note of patients’ age, gender, sexual group, days since their last unprotected sexual intercourse, the numbers of their partners in the previous six months and that of with whom they had unprotected sex with, and the results of STI screening on each episode, and being counselled by health advisors were recorded.
The recorded categories were recorded in a Microsoft Excel® spreadsheet. Median values with inter-quartile range were calculated for non-parametric data. Mann-Whitney's and Fisher's exact tests were used for comparison of non-parametric and categorical data, respectively.
Episodes of NSU, PID, gonococcal, chlamydial, trichomonas, syphilis, HIV and hepatitis B infections in addition to the first episode of positive testing for genital herpes and genital wart were considered positive STI in the final model. Infection with more than one STI at each attendance was considered a single episode of infection.
Cox regression analysis was used to investigate the independent effect of possible variables for testing positive for an STI during subsequent attendance periods. Data were adjusted for patients’ age groups, use of condom, testing positive for STI and being counselled for STI on previous visit. Adjusted hazard ratio (HR) with 95% confidence intervals (CI) for each recorded factor was calculated. SPSS® (SPSS Inc., Chicago, IL, USA) version 1.4 software was used for statistical analysis.
Results
There were 302 patients with two or more episodes of attendance to the department within the nine years of study period. This included 24 (8%) men and 278 (92%) women. Those patients were re-screened for STI at least once within a median of 2.9 (1.6–5.3) years. Table 1 summarizes the demographical features of study patients.
The demographical and clinical features of study patients
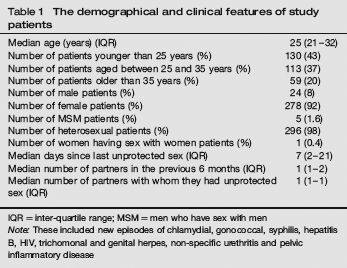
IQR = inter-quartile range; MSM = men who have sex with men
Note: These included new episodes of chlamydial, gonococcal, syphilis, hepatitis B, HIV, trichomonal and genital herpes, non-specific urethritis and pelvic inflammatory disease
At baseline, 70 (23%) patients had STI. Study patients were followed up for 1045.54 person-years. The incidence density of STI at the end of follow-up period was 15.69/100 person-years. The incidence of STI was 9.44/100 person-years in men, 8.74/100 person-years in women and 10.42/100 person-years in MSM. There was no significant difference between the incidences of STI among men and women (P = 0.759). The density incidence of condom use among study patients was 19.03/100 person-years.
In Cox's regression analysis, testing positive for an STI in subsequent screening episodes was significantly associated with patients younger than 25 years (HR 2.70 [95% CI 1.70–4.57]; P = 0.000). Being counselled by health advisors (HR 1.01 [95% CI 0.67–1.54]; P = 0.936) or being diagnosed with an STI in the last attendance (HR 1.06 [95% CI 0.68–1.66]; P = 0.780), however, did not significantly impact the subsequent risk of STI. Although there was a trend for reduced risk of STI and condom use, this was not significant [HR 0.72 (95% CI 0.40–1.30); P = 0.723].
Reduced possibilities for subsequent STI were noted among men and those delaying screening after unprotected sex; none of which was statistically significant. Table 2 summarizes the HR for different factors for a positive STI in each attendance in Cox regression analysis.
Associated risk factors for sexually transmitted infection episodes ∗ among patients reattending the department of genitourinary medicine in Cox's regression analysis
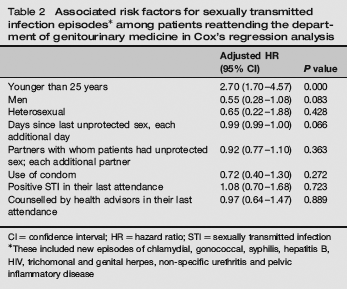
CI = confidence interval; HR = hazard ratio; STI = sexually transmitted infection
These included new episodes of chlamydial, gonococcal, syphilis, hepatitis B, HIV, trichomonal and genital herpes, non-specific urethritis and pelvic inflammatory disease
Discussion
The majority of patients reattending our centre were female, younger than 35 and heterosexual. The incidence of STI among them was 15.7/100 person-years over the follow-up period of 2.9 years. High rates of reinfection with bacterial STI after 12 months have been reported in other studies.3,4
These data suggest that a proportion of patients may continue to practice high-risk sexual behaviour and to be reinfected with STI after their first visit to GU medicine centres. The fact that those patients opted for rescreening is a positive sign of their knowledge on the risk of STI following such behaviour. Their inability to change their behaviour despite their knowledge deserves further investigation.
In the present study, patients younger than 25 years were 2.7 times more likely to test positive for STI in subsequent screening when compared with older patients. In general, patients younger than 25 years have the highest rate of most of STI in the UK. 1 The rate of reinfection among the same age group was 6.8 times higher than that of other age groups in a retrospective study on patients rescreened in USA over a 30-month period. 5
Although being diagnosed with an STI or counselled for STI in the last attendance were each associated with lower probability of STI, none were statistically significant. Absence of association of behavioural variables with reinfections with STI in the present study has been reported elsewhere.6,7
There was a trend for reduced STI and use of condoms that was not significant. This was unlike that reported previously among 3568 patients in whom 41% were women. 5 Inconsistent use of condoms and predominance of female patients might have been the cause of this discrepancy in the present study.
Consistent use of condoms among women has been reported to depend on the existence of relative sexual equality in their relationships and on women's self esteem. Relationships based on exchange of money for sex may be associated with less use of condoms. 8 In addition, the degree of adolescent females’ perceived parental monitoring has been shown to be inversely associated with high-risk sexual activities among adolescent females. 9
Consistent condom use has also been directly associated with anticipation of a positive response to requests for condom use and by partner support of condom use. 10
Patients’ education and counselling for STI and safe sexual behaviour may be the most effective method for reduction of transmission of STI. Lack of significant impact of counselling on subsequent incidence of STI in the present study highlights the need for the use of novel and robust counselling techniques for this group of patients. For example, a social skills intervention programme that focused on HIV risk-reduction information, sexual self-control, ethnic and gender pride, sexual assertiveness and communication skills, proper condom use skills and developing partner norms supportive of consistent condom use has been reported to be associated with increase in condom use. 11 Similarly, another randomized study has also reported a reduction in the rate of gonorrhoea and syphilis following behavioural interventions over a six-year period. 12
A recent meta-analysis however has not found any of the behavioural interventions successful in reduction of STI. 2 Because of high incidence of reinfection and lack of effect of counselling strategies, some authors have instead proposed rescreening of all patients with STI after a year. 3
The present study suffered from several shortages; it was a non-randomized retrospective study. Use of a less sensitive assay for diagnosis of chlamydial infection in the first five years of study period may have under-estimated cases of reinfection.
A small proportion of patients reattending our service were MSM and they had a high STI incidence. Further studies are needed to investigate the reasons for under-representation of this group of patients among those reattending GU medicine services.
We did not investigate acquisition of new sexual partners or failure to treat all previous partners as reported to be associated with reinfection with chlamydial infection.13,14 Those conclusions however have not been supported by other studies. 15 Because of such discrepancy, neither of those variables was investigated in the present study.
The other potential problem of the study was that behavioural counselling offered by health advisors was not standardized. Also, we did not investigate patients’ ethnicity which may have been associated with re-testing positive for STI. 6
Despite above shortages, the present study offered an insight into the demography of patients reattending one GU medicine centre. Also, unlike other studies that have used reduction in the frequency of high-risk sexual activity, the present study used the incidence of STI as its primary endpoint for the effectiveness of counselling for high-risk sexual activity.
In conclusion, our study confirmed a high incidence of STI reinfection among a group of patients reattending a GU medicine centre. Young age was significantly associated with STI reinfection. History of counselling for a previous episode of STI or condom use did not reduce the risk of re-testing positive for an STI at subsequent screening. Improvement in access to GU medicine services, encouragement of patients with an STI for rescreening on regular basis and use of novel STI counselling strategies, especially for younger patients may reduce the incidence of subsequent STI.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr Grace Kawai's contribution for data collection.