
Abstract
Summary
This audit compared sexual histories taken by self-completed questionnaires (SQ) versus the ‘gold-standard’ of ‘traditional’ face-to-face interviews by health-care professionals (HP). It compared reporting of symptoms and sexual behaviour and looked at outcomes in terms of diagnoses of sexually transmitted infections. SQ were at least equal to HP and might therefore be a valuable tool in streamlining services.
Introduction
High levels of risk-taking behaviour and sexually transmitted infections (STIs) among HIV-positive men who have sex with men (MSM) continue to be reported.1,2 Services therefore need to respond by providing rapid access to sexual health services. Self-completed questionnaires (SQ) have previously been shown to be an acceptable and reliable tool for the screening of sexual risk. 3 We introduced SQ (Figure 1) in early 2006 to streamline the service. The aim of this audit was to determine the impact, in terms of clinical outcomes, of using sexual histories taken by SQ compared with health-care professionals (HP) among HIV-positive MSM.
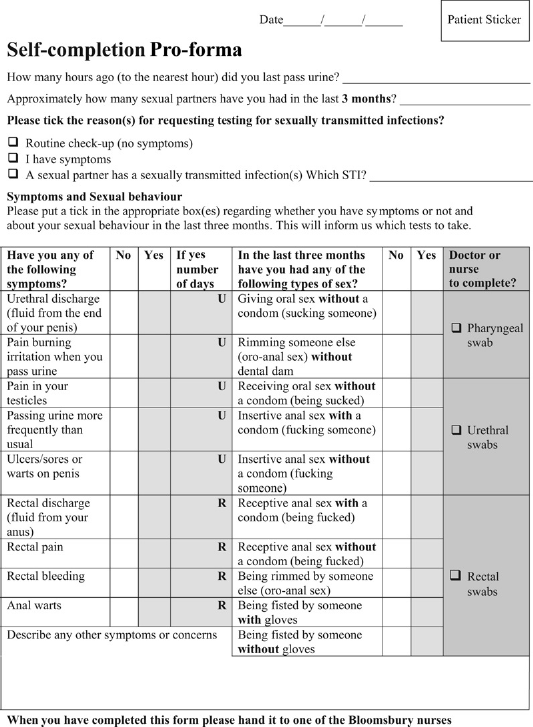
Self-history questionnaire
Methods
A retrospective case note review of all MSM requesting testing for STIs at the Mortimer Market Centre HIV outpatient service between 1 April 2006 and 30 June 2006 was undertaken. Details of sexual behaviour, presenting conditions, STI testing, diagnoses and health promotion were recorded and compared between SQ and HP.
Results
One hundred and five individuals underwent testing for STIs on 120 occasions (median 1; range 1–4). Sixty-six individuals had sexual histories taken using SQ (7 on more than one occasion, amounting to 75 total screens) and 44 individuals (one on more than one occasion, amounting to 45 total screens) using HP. Five individuals had sexual histories taken using SQ and HP on different occasions. Patients in both groups underwent similar number of STI screenings in the previous year (median 2; range 1–17).
Sexual behaviour
The median number of sexual partners in the previous three months was four in both groups (range 0 to >30), although this parameter was not recorded in 21 of 45 (45%) histories taken using HP. Of 105, 51 (49%) individuals reported at least one episode of unprotected insertive and/or receptive anal intercourse (UPAI) in the previous three months with rates being similar in both groups. Of these 51, 13 (25%) reported UPAI with potentially discordant partner(s). Of 105, 7 (6.7%) reported fisting without gloves. In the previous three months, sexual practices resulting in potential exposure to STIs at pharyngeal, urethral and rectal sites were documented in 96%, 96% and 86%, respectively, of the SQ group (compared with 72%, 72% and 63% of the HP group).
Symptoms
Overall, 45 of 120 (38%) patients were asymptomatic. Of those reporting symptoms, 38 of 120 (32%) reported urethral (discharge, dysuria), 23 of 120 (19%) rectal (rectal discharge pain or bleeding) and 7 of 120 (6%) both urethral and rectal symptoms. Documentation of presenting conditions was more detailed when sexual histories were taken using SQ (Figure 2).
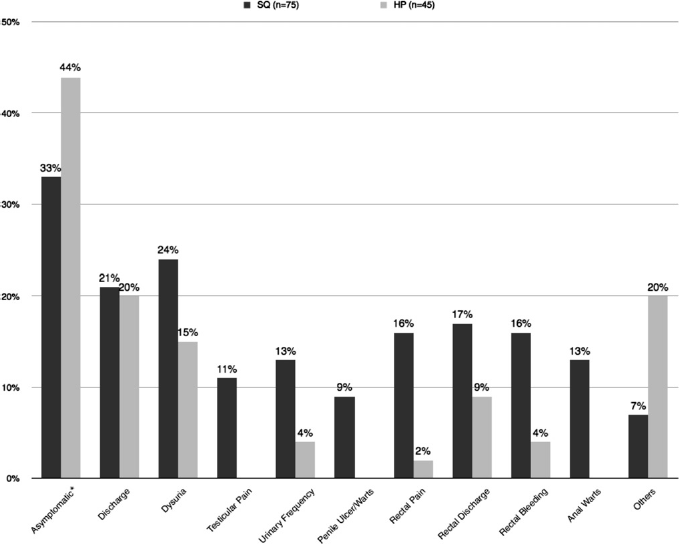
Reported/documented symptoms ∗Note: ‘Asymptomatic’ includes both the patients who were asymptomatic and those where no symptoms were reported or documented
Testing
In the SQ group, throat swabs were done in 97%, urethral swabs in 99% and rectal swabs in 91% (in HP group 96%, 93% and 87%, respectively).
Diagnosis
Overall, 52 of 105 (49.5%) had at least one STI within the threemonth observation period. The rate of STIs was similar in both groups (overall 48% vs. 49%).
Health promotion
Overall, a similar proportion of patients in both groups saw an Health Advisor (HA). Of those diagnosed with a bacterial STI, 83% saw the HA. Additional health promotion (advice on risk reduction, condom use, medication side-effects, general health, etc.) was documented in 71% where sexual histories were taken using SQ versus 51% taken using HP.
Discussion
The high rates of partner change, UPAI, fisting and STIs among this group of HIV-positive MSM is a cause for concern. Similar to previous work, we find that self-taken histories provide a detailed record of sexual behaviour and presenting conditions. 4 In our audit, more patients disclosed high-risk behaviour when using SQ. SQ may encourage answers to questions on sexual behaviour that might be missed on routine screening due either to health professional being unkeen to ask or due to the individual being less likely to disclose sensitive information in face-to-face interviews.5,6 In this audit, we showed that SQ did not identify adequate information on status of sexual partners. This has led to the proforma subsequently being modified.
SQ might only be acceptable to frequent users of the service who are familiar with the information required and terminology used. While there were no reported problems regarding completion of the SQ, we are aware that privacy is essential.
SQ affords the opportunity to optimize staff workload to allow more time to focus on issues such as health promotion and reduction of risk behaviour and STIs. SQ offers more patient choice and may help manage capacity issues with HIV services without compromising clinical outcomes and clearly merit further evaluation.