
Abstract
Summary:
Blood lipids and high-sensitivity C-reactive protein (hsCRP) are used to assess cardiovascular disease (CVD) risk. We evaluated in a cross-sectional design the relationship of hsCRP to markers of liver function (aspartate and alanine transaminases [AST and ALT, respectively]), CVD risk factors and HIV-disease progression markers in 226 HIV-1 seropositive drug users. hsCRP showed a significant inverse relationship with ALT and high-density lipoprotein, independent of age, gender, viral load, CD4 cell-count and antiretroviral (ARV) use, and was not significantly associated with HIV-disease progression markers. Serum markers of liver damage, AST and ALT, were associated with lower hsCRP, total cholesterol, low-density lipoproteins and triglycerides. Elevated liver enzymes (≥40 IU/L) were predictive of hsCRP levels that are considered a low risk for CVD. In conclusion, hsCRP may not be a reliable marker of CVD risk in populations with HIV at-risk for elevated liver enzymes due to high hepatitis B virus/hepatitis C virus prevalence and ARV use.
Introduction
High-sensitivity C-reactive protein (hsCRP) is a prototypical acute phase protein produced in the liver that responds to tissue damage and microbial infection by rapidly increasing from trace amounts in the blood to several hundred micrograms per microlitre, as part of the innate immune response. 1 Beyond its role as a useful marker of inflammation and infection, 2 increases in hsCRP also appear to play an independent role in predicting cardiovascular disease (CVD), 3 6 as atherosclerosis is principally an inflammatory disease. 7
HsCRP may be used in conjunction with several standard measures to assess CVD risk. hsCRP adds prognostic information of subsequent CVD event risk at all levels of severity of the metabolic syndrome, 8 a cluster of risk factors for developing CVD and to low-density lipoproteins (LDL), the primary targeted treatment parameter in the clinical setting. hsCRP may even be a stronger predictor of CVD events than LDL. 9
The improved clinical course and survival of HIV-positive patients with the advent of antiretrovirals (ARV) are associated with increased CVD risk. 10 Metabolic syndrome occurs at a higher rate in HIV-infected patients, 11 especially those receiving protease inhibitors, 12 and populations with HIV have shown increased hsCRP over time. HIV infection has been associated with increased inflammatory markers (hsCRP, interleukin-6), high triglycerides, low high-density lipoprotein (HDL) and impaired glucose tolerance, and these were strongly related to body composition parameters, particularly waist-to-hip ratio (WHR). 13 Increased hsCRP marks intercurrent infections in HIV, but sustained abnormal hsCRP values have also been described in those without a diagnosis of opportunistic infection. 14 HsCRP has been associated with parameters of HIV disease progression, CD4 cell-count and HIV viral load (VL), as well as a decreased time to AIDS, 15 and it is an independent predictor of survival. 16 Low-sensitivity C-reactive protein (CRP) was found to be a predictor of HIV mortality independent of CD4 cell-count, VL, serum albumin and body mass index (BMI). 17
The relationship of hsCRP to CVD risk factors has not been well studied in populations with HIV who abuse drugs. This population has an increased prevalence of liver damaging conditions such as hepatitis B and C. To further evaluate the value of HsCRP as a predictor of CVD risk in people with HIV, we examined the relationship of hsCRP levels to risk factors for CVD and markers of liver function in an HIV-positive population of drug users.
Methods
Study design
A cross-sectional study was conducted on a cohort of 226 HIV-infected drug users. The study protocol was approved by the Florida International University Internal Review Board. The inclusion criteria for this study were documented HIV-seropositive status, age 18 or older, active drug use and informed consent.
Participant examination protocol
Physical examination and medical history were performed and venous blood was drawn after a 12 h fast for CD4 cell-count, VL, hsCRP and chemistry including aspartate transaminase (AST) and alanine transaminase (ALT). All biochemical assays were performed using standard laboratory techniques. Hepatitis C virus (HCV) and hepatitis B virus (HBV) infections were confirmed by medical documentation with participants’ written permission.
Statistical analysis
Descriptive statistics were used to assess the data for normality, and transformations performed on variables when appropriate. Analysis of variance, chi-square and the Mann-Whitney U test were used to compare means between participants with ALT <40 IU/L and ≥40 IU/L. Univariate Pearson's correlations between CRP and lipid parameters, transaminases and anthropometric measures were calculated. Those parameters showing correlations with a significance level of P < 0.25 were included in the linear regression analyses.
A multiple linear regression was performed to analyse for independent predictors of CRP in the entire cohort, and in the portion of the cohort with ALT <40 IU/L. Age, gender, HIV VL, CD4 cell count and ARV use were controlled in the final model. The value of liver enzymes, as predictors of CRP (≥3 mg/L) and LDL (≥100 mg/dL) levels, considered a risk for CVD was evaluated using logistic regression.
Results
The population was 73% male, 80% African-American and had a mean age of 42 ± 7.4 years. Sixty-four percent received ARV therapy and 40% had a CRP ≥3.0 mg/L. The prevalence of HBV and HCV in this cohort was previously shown to be 38%. 18 A comparison of population characteristics between participants with and without elevated ALT (<40 or ≥40 IU/L) showed that those with elevated ALT were significantly older, had a higher prevalence of ARV use and significantly lower LDL and CRP levels (Table 1). Prevalence of HBV and/or HCV co-infection was higher in those with ALT ≥40 IU/L. Similar differences were found between those with and without elevated AST (<40 or ≥40 IU/L), except for those receiving ARV. Total cholesterol was significantly lower in those with elevated AST (172 vs. 158 mg/dL, P = 0.008).
Population characteristics and comparison by aspartate transaminase (AST) level

Comparison by AST level
Analysis of variance
Chi-square test
Mann-Whitney test
HAART = highly active antiretroviral therapy; HIV VL = HIV viral load; CRP = C-reactive protein; HDL = high-density lipoprotein; LDL = low-density lipoprotein;
BMI = body mass index
Correlation coefficients
We evaluated the relationship of lipid parameters, anthropometrics, liver transaminases, HIV-disease progression parameters and blood pressure with CRP in the entire cohort, and in those with ALT <40 IU/L. Correlations with significance of P ≤ 0.25 were included in the initial regression analysis. In the entire cohort, HDL (r = -0.161, P = 0.016) and LDL (r = 0.116, P = 0.089), waist circumference (r = 0.101, P = 0.141), and both AST (r = -0.269, P < 0.001) and ALT (r = -0.276, P < 0.001) met the criteria for inclusion into the regression. As the two liver enzymes were highly correlated, ALT was selected for use in the regression analysis because it was more specific for hepatic injury 19 and had the stronger correlation with CRP. These variables were included in the linear regression, as well as age, gender, HIV VL, CD4 cell count and ARV use. Diastolic and systolic pressure, BMI and WHR were not significantly correlated with CRP.
In the group with ALT <40 IU/L, HDL (r = -0.216, P = 0.006), WHR (r = 0.125, P = 0.122) and waist circumference (r = 0.129, P = 0.111) were correlated with P ≤ 0.25, and included in a second regression analysis that included age, gender, HIV VL, CD4 cell count and ARV use.
Linear regression analysis
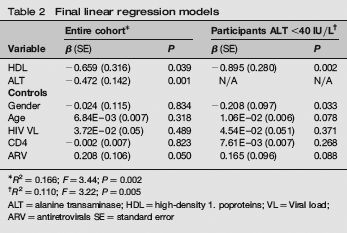
Linear regression for the entire cohort was performed with lipid variables entered first, followed by anthropometrics, liver enzymes and control variables. The final regression model included HDL, ALT, gender, age, VL, CD4 count and ARV use (R2 = 0.166, F = 3.44, P = 0.002). HDL (β = -0.659, P = 0.039) and ALT (β = -0.472, P = 0.001) had inverse relationships with CRP and ALT had the greatest effect (standardized β = -0.290). ARV use was significantly (β = 0.208, p = 0.05) related to CRP.
The final regression model for those with ALT <40 IU/L included HDL, gender, age, VL, CD4 count and ARV use (R2 = 0.110, F = 3.22, P = 0.005). HDL (β = -0.895, P = 0.002) and gender (β = -0.208, P = 0.033) were significant contributors and age (β = 0.011, P = 0.078) approached significance. HDL and male gender showed inverse relationships with CRP, and HDL had the greatest effect (standardized β = -0.256). ARV use was not significant. WHR and waist circumference were non-significant contributors to the final model (Table 2).
Final linear regression models
R2 = 0.166; F = 3.44; P = 0.002
R2 = 0.110; F = 3.22; P = 0.005
ALT = alanine transaminase; HDL = high-density 1. poproteins; VL = Viral load; ARV = antiretrovirals SE = standard error
Logistic regression of AST on CRP and LDL
Variables to be included in the logistic regression were recorded as bivariate variables. CRP was categorized according to the American Heart Association designation of low/average (<3 mg/L) and high risk (≥3 mg/L) for CVD. 20 ALT and AST were categorized as <40 and ≥40 IU/L, and LDL as <100 and ≥100 mg/dL, respectively, according to the Adult Treatment Panel III classification. 21 Participants with normal ALT and AST levels (<40 IU/L) were three times more likely than those with elevated levels (≥40 IU/L) to have CRP ≥3 mg/L, (odds ratio [OR] = 3.28, 95% confidence interval [CI] = 1.61-6.68 and OR = 2.85, 95% CI = 1.5-5.42, respectively), and twice as likely to have LDL levels ≥100 mg/dL, considered a risk for CVD (OR = 2.08, 95% CI = 1.04-4.15 and OR = 2.38, 95% CI = 1.24-4.56, respectively), independent of gender, age, HIV VL, CD4 cell count and ARVs.
AST had a significant inverse relationship with total cholesterol (r = -0.21, P = 0.002), LDL (r = -0.225, P = 0.001) and triglycerides (r = -0.156, P = 0.021) independent of ARV use, HIV VL, CD4 count, age and gender. The relationship of ALT with total cholesterol (r = -0.115, P = 0.091) and LDL (r = -0.127, P = 0.067) was weaker and approached significance. No relationship between AST or ALT and HDL was found.
Discussion
The relationship of markers of inflammation to CVD has been studied extensively in populations without HIV-1 disease. These studies demonstrate a significant association between hsCRP and risk of CVD, as well as other risk factors for CVD. 4 6 In addition, CRP adds predictive value to the metabolic syndrome and LDL.8,10 Since the advent of highly active antiretroviral therapy, the risk of CVD has become a concern in the HIV-infected population. The higher incidence of infectious diseases associated with liver damage, HBV and HCV and the use of liver-toxic ARV medications22,23 by this population requires a reevaluation of the efficacy of some of the traditional and more recent parameters for CVD risk evaluation.
Blood CRP is predominantly produced by hepatocytes, and its production in response to bacterial infection is attenuated in patients with liver dysfunction.24,25 A blunted acute-phase response, including reduced peak hsCRP concentrations, has been associated with impaired liver function 26 and an unresponsiveness of liver hepatocytes to CRP producing stimuli was shown in HCV-positive haemodialysis patients who had higher ALT when compared with HCV-negative patients. 27 The effect of elevated transaminases on hsCRP, however, has not been studied in HIV infection.
Our study shows a high prevalence (27%) of elevated liver transaminases in HIV-positive drug users. There was no significant difference in CRP levels between those with and without HBV or HCV. ALT and AST, however, were significantly higher in the HIV/HBV and/or HCV co-infected participants. In participants with normal ALT, the effects of other CVD risk factors (gender and age) on CRP became manifested. In those with elevated ALT and AST, commonly used lipid parameters for the assessment of CVD risk were lower, and they were more likely to have CRP levels that would be considered ‘low risk’ for CVD (CRP< 3 mg/L).
These data indicate that there is a danger of underestimation of CVD risk in populations with a high prevalence of conditions leading to elevated transaminases including co-infection with HBV and/or HCV and ARV use, if liver status was not taken into consideration. The predictive value of CRP as a biomarker of CVD risk is especially compromised in the assessment of HIV-positive drug users. HBV and HCV status alone does not necessarily affect CRP levels; however, when accompanied by evidence of liver damage, including elevation of transaminases, hsCRP may not be a reliable marker of CVD risk.
Footnotes
Acknowledgments
This work was supported by the National Institute on Drug Abuse (Grant R01-DA-14966). We thank all participants in this study, without whom advancement in the management of HIV would not be possible.
Appropriate informed consent was obtained and clinical research was conducted in accordance with guidelines for human experimentation as specified by the US Department of Health and Human Services and/or authors’ institutions.