
Abstract
HIV/AIDS epidemic is crucial in China; however, few studies were performed on youths. This study was performed to examine the effectiveness of peer-led HIV prevention intervention on HIV-related knowledge, attitudes and behaviour intention in senior high-school students in San-ming, a medium-sized city in Fujian province. Three thousand and sixty-eight students completed self-administered questionnaires before and after intervention, of which 981 students (the intervention group) accepted peer-led HIV/AIDS prevention intervention and others (the control groups) continued the usual teacher-led health education curriculum. Significant increases were observed in the intervention group in HIV-related knowledge, in attitudes and in behaviour intention after intervention. The results of this research also indicated an inconsistent level of HIV/AIDS knowledge and attitude among students, with a significant gender, health education history and style difference in session delivery. More concerted efforts in HIV prevention are needed to improve young people's sexual health.
Introduction
The HIV/AIDS epidemic is crucial in China as the number of HIV-positive cases detected increases rapidly. 1 The epidemic of HIV/AIDS greatly threatens Chinese youths, as many of them were increasingly exposed to high-risk sexual behaviours. However, awareness on HIV/AIDS prevention remains to be low. A number of studies demonstrated that most of them lack basic sex information and remain to be HIV-related stigma.2–4 Meanwhile, their attitude towards sex become more open, as studies showed that 5–20% of college students5–7 and 3–8% of senior high-school students had sexual experience.3,4,6,8 Studies showed that increases in HIV transmission was associated with changes in sexual behaviours. 9 Increasing percentage of new HIV cases is reported by sexual transmission. 1 There is a concern that the epidemic might spread further.
The situation is worrisome in the coastal areas of China. By the end of 2006 in the Fujian province, it was reported that 1150 citizens lived with HIV/AIDS and 67.8% were in their twenties. It is necessary to find out an effective prevention intervention method to promote sexual health of young people, as neither a cure nor an effective vaccination for AIDS is available. 10 Peer education has become an increasingly popular method of health promotion over the past decade, particularly with respect to sexual health issues of young people and substance misuse.11,12 School-based peer education on HIV prevention has been approved to be effective in China.6,13 However, most interventions targeted college students in big cities.5,6,14 Little attentions has been paid to youths in senior high schools in medium-sized cities. So what is going on in senior high-school students in medium-sized cities, with the Chinese government's ongoing efforts to improve school health education? What is the proper way to deliver the knowledge to those groups?
We initiated and piloted a peer-led HIV prevention intervention programme in senior high schools in San-ming, a medium-sized city in Fujian province, to investigate the effectiveness of peer-led versus the usual teacher-led health curriculum in enhancing the knowledge of HIV, attitudes and behaviour intention.
Subjects and Method
Sample
The study samples were from schools of San-ming by cluster-classification, using socioeconomic situation, population density and school type (model, ordinary and vocational school) as criteria. The study samples included a total of 3068 senior students (from 7071); out of which 981 students were randomized into the peer-led HIV/AIDS prevention group (the intervention group), and another 999 and 1088 students were randomized into the usual teacher-led heath education curriculum (the internal and external control groups, respectively) (Figure 1).

Sampling framework
The 3068 sampled students completed a self-administered questionnaire before and after the intervention in all study groups in 2006, at a three-month intervention. The students were informed that participation in the survey was voluntary and the survey was anonymous.
Peer educator selection and training
Peer educators were selected by teachers, later verified in an interview participated by the experts. The selection criterions included charismatic personality, credibility, ability in communicating and establishing relationship with the other students, and good school performance. Forty-six peer educators, aged 16.5–17.7 years old, were chosen and given a four-day training on educational protocol design, resources identification and anchoring classroom sessions to improve the knowledge, attitude and behaviour of their classmates on HIV/AIDS.
Intervention
Intervention was conducted to: (1) increase knowledge about the transmission and prevention of HIV; (2) improve behaviour and behaviour intentions to abstinence and build life skills; (3) eliminate prejudice and stigmatization towards people living with HIV/AIDS (PLWHA). The intervention was integrated into the regular school health education schedule to avoid disruption in schools, and the intervention was delivered one session per week for four weeks. The sessions emphasized on the basic knowledge and attitude towards HIV/AIDS, sexually transmitted diseases (STDs), pregnancy and related skills. These sessions replaced the usual health curriculums taught by health teachers to the intervention group.
There were small and large sessions of the intervention groups, 470 and 511, respectively. According to the facility of the schools, usually a small session contained 44–66 students and a large session contained 100–150 students.
Process evaluation
To monitor the implementation of the intervention, the participating students were required to complete a questionnaire during the intervention. The questionnaire included the quality of the peer educator driving classes, the arrangement of the content, the performance and attitude of the peer educators, and suggestions.
Outcome measures
The questionnaire included questions on the following issues. Knowledge – 41 items on knowledge of reproductive health, STDs and HIV/AIDS to which the students responded with yes, no or not sure; attitudes – nine items on attitudes towards PLWHA, premarital and extramarital affairs for which the students responded with a five-point scale ranging from agreement to disagreement; behaviour intention – five items where students responded with sure, maybe or not sure. Information on individual social-demographic characteristics was also collected.
For each item included in the scales for measuring knowledge, attitudes and behaviour intention, a score was designed for each response. Total scores were computed as a sum of each item score and then standardized to a range of 0–100. The higher the score, the better the related knowledge, attitudes and behaviour intention.
Statistical analysis
The comparison of demographic characteristics and behaviour intention within study groups was performed by chi-square tests. Changes in knowledge, attitudes and behaviour intention before and after intervention within each group were evaluated by Student's t-tests, and comparison of knowledge before and after intervention among study groups were done by analysis of variance (ANOVA). Analysis of covariance (ANCOVA) was used to assess the impact of delivery style of education. All statistical analyses were performed using SPSS for windows 11.0 (SPSS Inc., Chicago, IL, USA). In the presentation of the results, the statistical significance level was set at P < 0.05 (two-tailed).
Results
Demographic characteristics
A total of 3068 and 2901 students completed the questionnaires before and after intervention. The attrition rate was 5% for the intervention group, 6% for the internal control group and 6% for the external control group, because of absenteeism in schools.
In this section, variances such as age, gender and school type were compared by study group. Major differences were found in school type (P < 0.001). Compared with the external control group, the internal control group had more characteristics in common with the intervention group and the confounding factors were more easily controlled (Table 1).
Demographic characteristic for students by study group
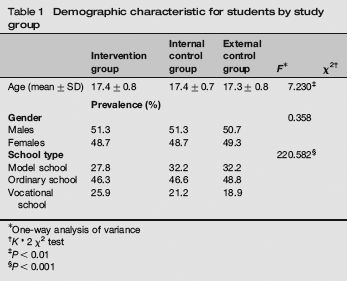
One-way analysis of variance
K* 2 χ2 test
P < 0.01
P < 0.001
Process evaluation
The median duration of the interventions was 4 h. Eighty percent of students reported to be actively involved in the sessions and 92% of the students showed their appreciation for peer-led education.
Changes in knowledge and attitudes
There were statistically significant increases in HIV/AIDS-related knowledge and attitude towards PLWHA from pre-test to post-test in the intervention group (P < 0.001), but no significant increase was observed in the control groups (including internal and external). The attitude towards premarital and extramarital affairs did not change significantly both for the intervention and control groups during the intervention (Table 2).
HIV/AIDS-related knowledge and attitude scores of pre-test and post-test by group (mean ± SD)
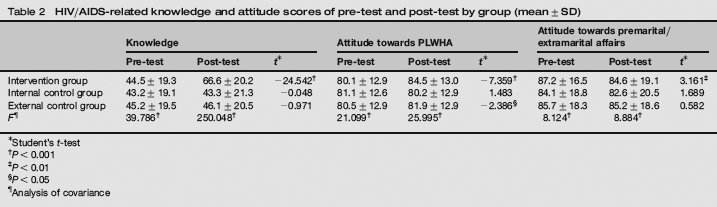
Student's t-test
P < 0.001
P < 0.01
P < 0.05
Analysis of covariance
Gender, history of school health education and the style of delivered session had an impact on the scores of baseline knowledge and attitude towards PLWHA. All students had increased scores in related knowledge and attitudes, and the increases were found to be more obvious in females, in students who had education history and delivered in small session (Table 3).
HIV/AIDS related knowledge and attitudes scores of pre-test and post-test in the intervention group (mean ± SD)

Student's t-test
P < 0.01
P < 0.05
Analysis of covariance with school type as covariant
P < 0.001
Behaviour and behaviour intention
Data show that 23.3% of students had loving experience and 3.6% had sexual intercourse, in which 59% of the students did not take any contraceptive measures. The ratio of intercourse was 4.6% for vocational schools and 1.5% for model schools, a significant difference across school style at baseline (P < 0.01).
Intervention affected students’ behaviour intention remarkably, keeping them abstinent during school years and condom use in case of premarital intercourse (P < 0.05). Differences were not found in keeping abstinence till marriage and rejecting drug (Figure 2).
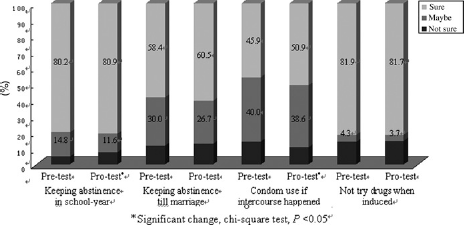
Changes in behaviour intention pre-test and post-test in the intervention group. (Note: Significant differences were found in the ratios of students who intend to abstain themselves in the school years and use condoms in the event of premarital intercourse happening after intervention (P < 0.05), but not in the ratios of those who intend to abstain until marriage and reject the drug.)
Discussion
Peer-led HIV prevention interventions have been tested as pilot studies among many school populations and become increasingly popular, especially, as a method of imparting health information to schools.15,16 Our study also showed that the interventions could improve youths’ knowledge of HIV/AIDS, their attitude towards PLWHA and behaviour intention. More improvements were found in knowledge, just as the previous short-term intervention showed.3,17 Compared with their counterparts in Shanghai,3,17 youths in the study generally perceive a low level of baseline knowledge and improvement during the intervention. Study samples from four colleges in Fujian province also indicated that students there were susceptible to HIV infection.7,18
The results of this research indicated an inconsistent score level of AIDS knowledge and attitude towards PLWHA among students, with a significant gender, health education history and style difference in session delivery. Previous researches similarly found that male students were more likely to have higher scores before intervention,3,19,20 while the increase was more obvious in female students during intervention, 20 which suggested that gender difference should be considered in the future interventions.20,21 We found that students in small-size session experienced greater increase in knowledge, attitude and behaviour intention than those in large-size session. Studies illustrated that small groups created cooperative learning situation and thus enabling the participants to discuss and communicate. 22 This could partly explain the differences mentioned above and the proper size of sessions should be investigated further.
Researches indicated that school-based HIV education intervention reduced the reported risky sexual behaviours.10,16 We found significant changes in behaviour intention after intervention, but the data on sexual behaviours were unavailable after intervention for a short duration. Nevertheless, our study was in agreement with the result of a study, which indicated that school-based health education did not encourage the behaviour. 23 Our survey found that there was no difference in the ratio of sexual intercourse between those who had and had not school-based health education experiences. The ratios of school-based health education acceptation in model, ordinary and vocational schools were 62.7%, 48.9% and 47.8%, respectively. However, higher ratio of intercourse was found in the vocational schools.
There are several limitations that should be considered in interpreting these results. First, the questionnaire of the participants was unable to be identified and compared before and after the intervention, as an anonymous questionnaire survey was adopted, which may lead to the loss of some information. The second limitation exists in the mechanism under which the peer educators are selected, trained and supported. In this research, some peer educators were chosen by teachers based on their academic skills, instead of their ability in communicating and establishing relationships, which may prejudice the trustfulness and communication in the intervention, and different selection strategies could be used. 24 And intervention training and support should be consistent with the end task. Finally, the duration of the study may not be long enough to let us observe changes in behaviours. Long-term follow-up study should be conducted in a long run.
Conclusion
The peer-led education of HIV/AIDS, especially provided in small-sized session, is more effective in improving the knowledge, attitude and behaviour intention among high-school students, than the usual teacher-dominated health education. To improve the sexual health of adolescents, effective strategies and secured supports from the schools and the communities are needed. Further research has to be conducted to assess the longterm impact of peer-led HIV prevention intervention in sexual health of youths.
Footnotes
Acknowledgements
This research was funded by the Foundation of Project HOPE, Hong Kong (04PH21005). Our sincere gratitude is due to other members of the research team and all the youngsters and the schools participating in this research.