
Abstract
We conducted a cross-sectional study with 385 HIV-positive women in Bangkok to assess the prevalence and predictors of cervical abnormalities on Papanicolaou (Pap) smear. Low-grade squamous intraepithelial lesions (LSIL), high-grade SIL (HSIL) and invasive cervical cell cancer (ICC) were assessed by cytological examination after Pap smear and logistic regression models were used to assess associations with patient characteristics. Overall prevalence of LSIL, HSIL and ICC were 11.2% (95% confidence interval [CI] 8.2-14.7%), 4.7% (95%CI 2.8-7.3%) and 0.5% (95%CI 0.06-1.9%), respectively. In multivariate models, only the nadir CD4 count and income remained significantly associated with cytological abnormalities, whereas smoking, hormonal contraceptive or antiretroviral use, condom use, parity and number of lifetime sexual partners were not associated. The odds ratio for having cytological abnormalities was 2.6 (95% CI 1.24-5.34) in those with a nadir CD4 count <200 cells/mm3 compared with those with a higher nadir CD4 count, and 1.99 (1.11 -3.57) in those with an income of <125 US dollars/month compared with those with higher incomes. In settings where access to affordable treatment is improving, this study reinforces the importance of regular Pap smear screening in HIV-positive women, particularly those with low nadir CD4 counts and lower incomes.
Introduction
Among the world's poor, cervical cancer kills more women than any other cancer.1,2 Morbidity and mortality associated with HIV-1 infection is also a serious problem in many resource-limited settings, and women are disproportionately affected. 3 The immunodeficiency that arises from HIV-1 infection increases the risk of a number of different cancers, including invasive cervical cell cancer (ICC) and its precursors, squamous intraepithelial lesions (SILs) of the cervix.4–6 Other factors that are associated with an increased risk of cervical cancer include smoking, multiple sexual partners and young age at first sexual intercourse. 7
Fortunately, SILs detected early are treatable. Therefore, because of the higher prevalence of SILs and ICC in HIV-infected women, screening and prevention programmes are vitally important for early detection and treatment. Early cervical cytological changes are easy to detect using Papanicolaou (Pap) smear screening, and this technique is a cost-effective screening methodology when women present for follow-up. 2 With increasing access to effective antiretroviral (ARV) regimens, HIV-infected women in Thailand live longer, with fewer HIV-related complications. For this reason, it is important to identify those at high risk for SIL and cervical cancer.
To date, there are limited data guiding clinical care of HIV-infected women in resource-limited settings in Asia. In Thailand, National Treatment Guidelines recommend initiating therapy when the CD4 count is approaching 200 cells/mm3, but many patients present late in the course of their illness when CD4 counts are low. We conducted this cross-sectional study to examine associations between demographic, behavioural and clinical features and the presence or absence of cervical cytological abnormalities on Pap smear in HIV-positive women in Bangkok, Thailand. The aim of our study was to identify factors that may predict which women are at highest risk for having cytological abnormalities on Pap smear, and who might most benefit from monitoring and early treatment interventions.
Methods
The study was conducted from January 2002 until December 2005. We enrolled women attending the Anonymous Clinic of the Thai Red Cross AIDS Research Centre in Bangkok, Thailand and women participating in clinical trials at the HIV-Netherlands-Australia-Thailand Research Collaboration, Thailand which is on the same campus.
The protocol was approved by the Institutional Review Board of Chulalongkorn University, and all participants gave informed consent before participating. Women of any age were eligible to participate if they had no gynaecological symptoms. Gynaecological examination was performed by a gynaecologist who collected a Pap smear using a wooden Ayre spatula. Specimens were smeared onto a single slide, fixed immediately in 95% alcohol and air-dried before being sent for cytological examination to the Division of Cytopathology, Department of Obstetrics/Gynecology, Faculty of Medicine, Chulalongkorn University. Cytopathologists were blinded to the participants’ HIV serostatus, and specimens were graded according to the Bethesda System for reporting results of cervical cytology. 8 All patients whose results were associated with cervical cancer were referred to as a colposcopist to define the point of abnormality and collect a tissue biopsy. In most cases, a CD4 count was performed on the day of the Pap smear. CD4 counts were determined by standard flow cytometry. All women were interviewed by the gynaecologist who conducted the Pap smear to collect demographic data, a sexual and obstetric history and a history of HIV infection and treatment. Untreated HIV infection results in a steady decrease in CD4 count and because of this progressive decline in CD4 count, we defined the nadir CD4 count as the most recent CD4 count before starting antiretroviral therapy (ART) for patients who had started highly active ART (HAART), or the CD4 count at the time of Pap smear for patients who were ART naive and presenting for voluntary counselling and testing. Income was assessed as a categorical variable and presented as greater than or less than 5000 Thai Baht, which corresponded to approximately 125 US dollars (USD) at the time the study was conducted, and represents the average monthly income for unskilled workers in Thailand. The average per capita monthly income for all Thais in 2004 was approximately 215 USD per month. 9
Statistical analysis
All statistical analyses were performed using SAS version 9.1 (SAS Institute, Cary, NC, USA). Prevalence of low-grade and high-grade squamous intraepithelial lesions (LSIL and HSIL) and ICC was determined and logistic regression models were used to estimate associations with patient characteristics using women with normal Pap smear as a reference group. We used a combined endpoint of both LSIL, HSIL and ICC (hereafter referred to as ‘cytological abnormalities on Pap smear’), since women with HSIL and ICC require urgent follow-up with colposcopic examination and biopsies and women with LSIL should have regular follow-ups. A chi-square test or Fisher's exact test was used to screen dichotomous variables. A Mantel-Haenszel chi-squared test was used to screen ordered categorical variables. Variables with a P < 0.2 in univariate analysis were included in a multivariate logistic regression model to determine odds ratios (OR) and 95% confidence intervals (CIs).
Results
A total of 385 HIV-positive women underwent Pap smear screening in this study. The prevalence of LSIL was 11.2% (43/385 women; [95% CI] 8.2-14.7), the prevalence of HSIL was 4.7% (18/385 women; 95% CI 2.8-7.3) and there were two cases (0.5%; 95% CI 0.06-1.9) of ICC, a combined prevalence of Pap smear abnormality (LSIL, HSIL and ICC) of 16.4% (95% CI 12.8-20.4).
The median age was 34 (interquartile range [IQR] 30-40) years, and there was no difference in age distribution between women with an abnormal Pap smear and those with a normal Pap smear. Forty-two percent of patients were ART naïve at the time of their Pap smear. The proportion of women with LSIL, HSIL or ICC did not differ between the women who were ART naïve compared with those who were ART experienced (P = 0.41, 0.46 and 1.0, respectively). Sixty percent were taking oral contraceptives (OCs) and 16% had smoked. The median duration of knowing HIV-positive serostatus was five (IQR 1-5) years.
One hundred and ninety-five (51%) patients reported having a previous pap smear, and the median duration of time since last Pap smear was three (IQR 2-6) years; 179 (92%) of these women had a normal Pap smear, seven (4%) reported a previous abnormal Pap smear and nine (4%) patients did not know the result of their previous Pap smear. For the seven patients reporting an abnormal Pap smear at the previous test, the result of the current test was normal in four patients and abnormal in three patients (two LSIL and one HSIL).
Neither age, route of transmission, smoking, age at first intercourse, ART use, oral or injectable hormonal contraceptive use, number of lifetime sexual partners, parity, whether the patient had intercourse in the previous year, nor known duration of HIV infection were associated with the presence of cytological abnormalities.
In univariate models, monthly income (P = 0.01), CD4 count at time of test (P = 0.01) and a nadir CD4 count (P = 0.0003) were associated with cervical abnormalities on Pap smear (Table 1). After adjusting for other variables in multivariate models (Table 2), only a nadir CD4 count (P = 0.0002) and monthly income (P = 0.02) were associated with the presence of cervical abnormalities. Compared with patients with a nadir CD4 count greater than or equal to 200 cells/mm3, the adjusted OR for having cervical cytological abnormalities in those with a nadir CD4 count < 200 cells/mm3 was 2.6 (95% CI 1.24-5.34). Compared with patients with a monthly income greater than or equal to 125 USD/month, the OR for having cervical cytological abnormalities in those with monthly income <125 USD was 1.99 (95%CI 1.11-3.57).
Univariate analysis of risk factors in women with and without cervical cytological abnormalities (LSIL, HSIL and ICC) detected in Pap smears. Significant associations are shown in bold
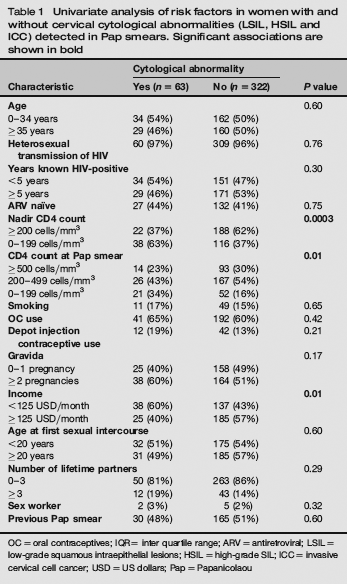
OC = oral contraceptives; IQR= inter quartile range; ARV = antiretroviral; LSIL = low-grade squamous intraepithelial lesions; HSIL = high-grade SlL; lCC = invasive cervical cell cancer; USD = US dollars; Pap = Papanicolaou
Multiple logistic regression analysis of factors risk factors for cervical cytological abnormalities (LSIL, HSIL and ICC) detected in Pap smears. Significant associations are shown in bold
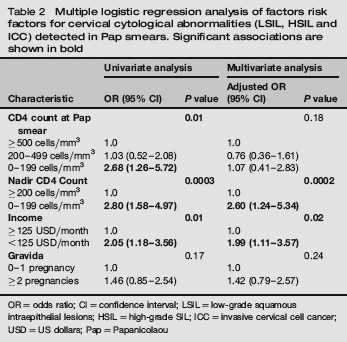
OR = odds ratio; CI = confidence interval; LSIL= low-grade squamous intraepithelial lesions; HSIL = high-grade SIL; ICC = invasive cervical cell cancer; USD = US dollars; Pap = Papanicolaou
Discussion
In this cross-sectional study, we found that the most important predictors of cytological abnormalities on Pap smear are a nadir CD4 count < 200 cells/mm3 and low-income level of <125 USD per month. In univariate models, CD4 count at the time of test of < 200 cells/mm3 is associated with the presence of cytological abnormalities, but after adjusting for a nadir CD4 count and other variables in multivariate models, this is no longer a significant predictor.
The relationship of cervical cancer and cervical cytological abnormalities to a degree of immunodeficiency has been well established in western cohorts. Studies have found that the incidence of abnormal cervical cytology was highly associated with HIV infection, and also demonstrated that the incidence of LSIL, HSIL and cancer increased as CD4 count decreased.4,10,11 Studies in resource-limited settings have also demonstrated a relationship between CD4 counts and cytological abnormalities on Pap smear. Levi et al. 12 reported a significantly higher prevalence of cervical intraepithelial neoplasia grades 1-3 in Brazilian women with CD4 counts < 200 cells/mm3 compared with those with higher CD4 counts. 12
Infection with HIV is also associated with an increased risk for persistent infection with oncogenic strains of human papillomavirus (HPV), which have a central role in the pathogenesis of SIL and ICC. More recently, investigators have shown that the presence of high-risk HPV types is the most important predictor of cytological abnormalities.13,14 Our study did not include testing for HPV, and this test is not routinely available in most resource-limited settings as part of routine clinical care. Nevertheless, our study adds new information by suggesting that the risk of SIL detected on Pap smear is related to the lowest CD4 count, and that immune reconstitution evidenced by CD4 count recovery following ART may not abrogate this risk. This may help to explain why the incidence of cervical cancer has not decreased in the HAART (highly active antiretroviral therapy) era. 15
The links between lower socioeconomic status and poor health outcomes have been well documented. 16 Low income can lead to poor health because of poor nutrition, unhealthy living or working conditions, and the inability to access and pay for medical care.7,17,18 In our study, a monthly income of <125 USD per month is an independent predictor of cytological abnormalities on Pap smear. It is possible that there may be a selection bias associated with low income, since treatment at our study sites is free of charge and these women may not have been able to afford access to some other health-care facilities where payment was required. However, there is no significant difference in the proportion of women who had a previous Pap smear, who had ever smoked, whether ARV naive or experienced, age at first intercourse, OC use and number of lifetime partners between those women with monthly income <125 USD compared with those with higher incomes.
The overall prevalence of SIL and ICC on Pap smear in our cohort study is 15.9% and 0.5%, respectively. These figures are comparable with other Thai studies in HIV-positive women where the overall prevalence of SIL and ICC on Pap smear is 10.5% and 2.2%19 versus 15.7% and 1.5%, respectively. 20 The higher prevalence of ICC in these latter studies may relate to different sexual, behavioural or HIV-disease characteristics between the populations studied.
There are several limitations to our study. First, as previously noted, we were unable to examine the effect of HPV infection on SIL and cancer prevalence. Secondly, we were unable to include HIV viral load in our models, as many patients who were not on ART treatment programmes did not have viral load tests. Although other studies have demonstrated that viral load is a strong predictor of abnormal cervical cytology 4 , it is not widely available in resource-limited settings. Thirdly, for the 40% of women in our study who were ART naive, the CD4 count at test was the same as the nadir CD4 count. We did, however, test the robustness of the model, limiting the analysis to those who had begun treatment with ART, who had different CD4 nadir and ‘at test’ CD4 counts, and the same multivariate model was selected. Fourthly, user bias may influence reporting of Pap smear results. However, in our unit, slides are reviewed by the same group of cytopathology technicians and abnormal results are confirmed by two cytopathologists. Quality control procedures, including random review of the normal Pap smear slides is undertaken by the cytopathologists, and the unit is accredited by the National Cytopathology Organization. Finally, this point prevalence estimate study was conducted at one centre in Bangkok, and the characteristics of these women with health seeking behaviour leading them to present for HIV testing at the anonymous testing clinic, as well as those already enrolled on treatment programmes, may not be representative of the entire at-risk population of HIV-positive women in Thailand.
Despite these limitations, this study has important public health implications for HIV-positive women in Thailand and other resource-limited settings where ART access is increasing, and a disproportionate number of infected individuals are women, who may present with advanced disease and low CD4. In contrast to other AIDS-defining neoplastic diseases that decrease in incidence as the CD4 count increases in response to HAART, cervical cancer does not appear to decrease in a similar manner. All women with HIV need more intensive cervical screening and follow-up than their immunocompetent counterparts. However, our study suggests that this is most important in women whose CD4 counts decline to below 200 cells/mm3 before initiating HAART, and these women, as well as those with low incomes, should have frequent Pap smear screening for the early detection of preneoplastic changes that may lead to cervical cancer.