
Abstract
Doppler tissue imaging (DTI) is a useful tool for the detection of subtle systolic function abnormalities related to the longitudinal contraction. We assessed left ventricular (LV) systolic function with DTI in 45 human immunodeficiency virus (HIV)-infected patients without any heart-related symptoms and in 30 healthy control subjects. Although conventional echocardiography showed no differences between groups, DTI revealed lower peak systolic velocities in group A patients when compared with group B ones (Sms: 8.84 ± 0.94 cm/s vs. 9.42 ± 0.84 cm/s, respectively, P < 0.001 and Sml: 9.58 ± 1.86 cm/s vs. 10.78 ± 2.07 cm/s P = 0.003). In group A patients, both peak systolic myocardial velocities at the septal (Sms) and lateral mitral annulus (Sml) correlated with CD4 lymphocyte count (P = 0.034 and 0.009, respectively). We conclude that pulse wave DTI reveals subtle and non-otherwise detectable abnormalities of the longitudinal LV contractile function in asymptomatic patients with positive HIV serology. DTI study should potentially be expanded in the population of HIV-infected patients, aiming at an early identification of LV systolic dysfunction.
Keywords
Introduction
Cardiac involvement in human immunodeficiency virus (HIV) seropositive patients is relatively common and is associated with increased morbidity and mortality.1–3
Cardiovascular manifestations in HIV infection have two clinical patterns: 6–7% of HIV-infected patients have significant cardiac disease while the remainder is asymptomatic. 4 Among asymptomatic patients, 8–10% develop symptomatic heart failure over a two- to five-year period, which constitutes an independent predictor of mortality. 5 This underscores the importance of the detection of systolic dysfunction early in the course of the disease which, if prematurely detected, in many cases, can be effectively treated. 1
The purpose of our study was to assess both; radial left ventricular (LV) contraction with conventional echocardiography and longitudinal contraction with Doppler tissue imaging (DTI) in HIV-infected patients. We performed the later modality taking into account that DTI renders possible the estimation of longitudinal function, which may be more sensitive than radial contraction to minor disturbances of LV function.6,7
Methods
Study design
Our study population consisted of 45 patients (aged 40.48 ± 10.23 years, 33 men – group A) with positive HIV serology and absence of any heart-related symptoms. The mean time from the diagnosis of HIV infection was 30.44 ± 36.31 months (range 2–144 months). Among them, 11 were in clinical stage A (two in A1, seven in A2 and two in A3), 14 in clinical stage B (four in B2 and 10 in B3) and 20 in clinical stage C (one in C2 and 19 in C3), according to the Centers for Disease Control and Prevention criteria. 8 All patients included were receiving highly active antiretroviral therapy (HAART), including two nucleoside analogues as backbone (with one of them being zidovudine in all cases) plus either a non-nucleoside analogue (nevirapine or efavirenz) or a protease inhibitor (elfinavir or indinavir).
Antibody levels against HIV were measured by an enzyme-linked immunosorbent assay and confirmed by Western blot analysis. CD4+ cell counts were determined within three days of the echocardiographic study (Facscan flow cytometer, Becton Dickinson, San Jose, CA, USA). Furthermore, 30 apparently healthy, age-matched individuals (aged 39.93 ± 9.71 years, 20 men – group B) with negative HIV serology were enrolled as control subjects.
Patients with atrial fibrillation, ischaemic, hypertrophic, congenital or rheumatic cardiomyopathy, ethanol abuse (>50 g/day), diabetes mellitus, moderate to severe hypertension or significant valvular disease were excluded from the study.
The ethics committee of our institution approved the study and all patients gave written informed consent.
Echocardiographic methods
Standard transthoracic examination
Conventional echocardiographic examination was performed with a commercially available imaging system (SSA-380A, Toshiba Power vision, Toshiba Corp., Tokyo, Japan) using a 2.5-MHz phased-array transducer employing second harmonic imaging by a single experienced operator, who was unaware of the subgroups condition. The following echocardiographic-Doppler variables were determined: ejection fraction using the Simpson's rule (EF), end-diastolic (EDD) and end-systolic diameter (ESD) of the LV, the peak velocity of early transmitral diastolic flow (Emax), the peak velocity during atrial contraction (Amax), the deceleration time (DT) of the early diastolic flow, and the LV isovolumic relaxation time (IVRT). All measurements were made in five cardiac cycles and averaged in order to minimize the variability induced by respiration.
Pulsed-wave DTI
After establishing the resting baseline measurements, using the DTI software of the same system, a pulse wave DTI study was accomplished. From the apical four-chamber view, a 5 mm pulsed Doppler sample volume for DTI was positioned just apical to the septal and lateral mitral annulus. Every effort was made to obtain a Doppler angle of incidence close to 0°, between the interrogating Doppler beam and the longitudinal motion of the LV. The following parameters were measured: Peak systolic velocities in the septal (Sms) and lateral mitral annulus (Sml), early peak diastolic velocities in the septal (Ems) and lateral mitral annulus (Eml), late peak diastolic velocities in the septal and lateral mitral annulus (Ams and Aml respectively), and the ratios Emax/Ems and Emax/Eml. The value assigned to each parameter was the average of five cycles.
Reproducibility for a single examiner was analysed in 10 randomly selected recordings. Intra-observer variability of DTI velocities measurement ranged from 3 to 4%.
Statistical analysis
Based on a statistical power calculation, we found that the number of participants was adequate to evaluate >0.5 two-tailed standardized differences in the peak myocardial velocities investigated between the groups studied. In particular, we achieved a statistical power >0.90 at <0.05 probability level (P value). Values are presented as mean ± SD. The differences between the groups were explored with Student's t-test for continuous variables. Mann-Whitney U test and χ 2 test were used to compare non-parametric and categorical variables, respectively. Linear correlations were analysed by Pearson's and Spearman's bivariate two-tailed method. Multinomial logistic analyses (stepwise procedure) were performed to investigate the independent and relative importance of peak myocardial velocities in the groups studied. The limit of statistical significance was set at P < 0.05.
Receiver-operating characteristic (ROC) curves were plotted from the results of peak myocardial velocities and were used to identify the best possible cut-point that gave optimal sensitivity and specificity.
The SPSS software (version 9.0, Chicago, IL, USA) was used for statistical analysis.
Results
The clinical characteristics of our study population are summarized in Table 1 and the results of the echocardiographic indices are presented in Table 2.
Clinical characteristics of the study population
HR = heart rate; SAP = systolic arterial pressure; DAP = diastolic arterial pressure
Values are expressed as mean values ± SD
P values <0.05 were regarded as statistically significant
Comparison of conventional echocardiographic and Doppler tissue imaging variables between the groups studied
EF = ejection fraction; EDD = end-diastolic; ESD = end-systolic; Emax = the peak velocity of early transmitral diastolic flow; Amax = atrial contraction; DT = deceleration time; IVRT = isovolumic relaxation time; Sms = systolic myocardial velocities at the septal; Sml = systolic myocardial velocities at the lateral mitral annulus
Values are expressed as mean values ± SD
P values <0.05 were regarded as statistically significant
The conventional two-dimensional echocardiographic examination did not show any difference for all the variables studied between groups. Indeed, no difference was found between HIV-infected patients and control individuals concerning the systolic performance (EF: 61.44 ± 8.06% vs. 64.26 ± 6.65%, respectively, P = ns) and the LV dimensions (EDD: 47.8 ± 5.69 mm vs. 45.76 ± 3.7 mm and ESD: 31.88 ± 4.06 mm vs. 30.76 ± 2.64 mm, respectively, P = ns for both comparisons). Similarly, Doppler study did not reveal any differences in the diastolic function of group A and B patients, including LV relaxation (IVRT: 85.91 ± 11.2 ms vs. 82.03 ± 11.21 ms, respectively, P = ns) and LV filling (DT: 186.55 ± 34.56 ms vs. 177.6 ± 35.61 ms, Emax: 68.13 ± 15.23 cm/s vs. 73.63 ± 13.6 cm/s, Amax 57.15 ± 12.66 cm/s vs. 52.96 ± 14.46 cm/s, respectively, P = ns for all comparisons).
DTI at the septal mitral annulus showed a peak Sms of 8.84 ± 0.94 cm/s in group A patients and of 9.42 ± 0.84 cm/s in group B individuals (P < 0.001) (Figure 1). Similarly, a statistically significant difference was found when peak systolic velocities at the lateral mitral annulus were compared (Sml: 9.58 ± 1.86 cm/s vs. 10.78 ± 2.07 cm/s in group A and B subjects, respectively, P = 0.003) (Figure 1).
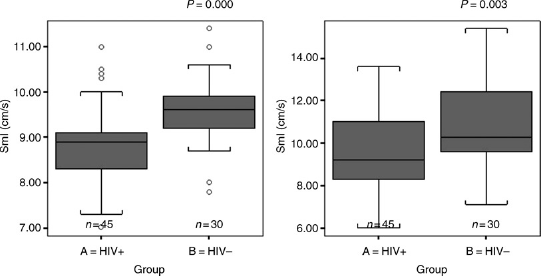
Peak systolic velocities range measured with pulse wave Doppler tissue imaging at the septal and lateral mitral annulus (Sms and Sml, respectively) in both groups. Interquartile ranges (box length), median values and outliers
As far as diastolic function was concerned, no differences were found between groups in both lateral and septal mitral annulus regarding peak Em and Am velocities: At the lateral mitral annulus DTI showed an Eml of 14.68 ± 4.07 cm/s in group A versus 16.41 ± 3.79 cm/s in group B (P = ns), whereas the values of Aml were 10.45 ± 1.46 cm/s and 9.84 ± 1.39 cm/s, respectively (P = ns). At the septal mitral annulus DTI showed an Ems of 13.52 ± 2.37 cm/s in group A versus 14.37 ± 2.23 cm/s in group B (P = ns) and an Ams of 9.83 ± 1.39 cm/s and 9.3 ± 1.04 cm/s, respectively (P = ns). Moreover, the Emax/Ems ratio was 5.21 ± 1.61 in group A patients versus 5.25 ± 1.31 in group B ones (P = ns), while the Emax/Eml ratio was 5.24 ± 3.07 and 4.76 ± 1.55, respectively (P = ns).
In group A patients the CD4 lymphocytic count was 293.6 ± 264.5 cell/μL. When the whole HIV-infected study population was taken into account, only peak systolic myocardial velocities were positively correlated with CD4 lymphocyte count (Sms: P = 0.034, r = 0.316 and Sml: P = 0.009, r = 0.386) (Figure 2).
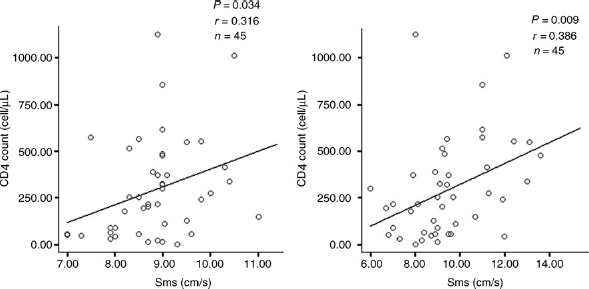
Correlation between peak systolic velocities measured with pulse wave Doppler tissue imaging at the septal and lateral mitral annulus (Sms and Sml, respectively) and CD4 count in HIV-positive patients
In multiple logistic regression analysis after the adjustment for age and sex, the odds ratios (OR) for Sms, Sml and CD4 count concerning the identification of the disease are presented in Table 3.
Contribution of selected variables to the identification of the disease in the population studied
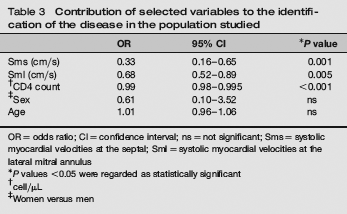
OR = odds ratio; CI = confidence interval; ns = not significant; Sms = systolic myocardial velocities at the septal; Sml = systolic myocardial velocities at the lateral mitral annulus
P values <0.05 were regarded as statistically significant
cell/μL
Women versus men
According to the results of the ROC curves, the best possible cut-off point for discrimination between HIV-positive patients and controllers was 9.15 cm/s for Sms (area under the curve [AUC]: 0.761) with the sensitivity and specificity being 76 and 77.7%, respectively. Concerning Sml, the best cut-off point was 9.85 cm/s (AUC: 0.708), a value which achieves a sensitivity of 71% and a specificity of 66.7% (Figure 3).
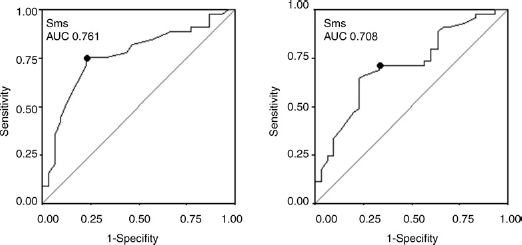
Receiver operator characteristic curve showing peak systolic velocities measured with pulse wave Doppler tissue imaging at the septal and lateral mitral annulus (Sms and Sml, respectively). The optimal cut-off points selected are indicated by the superimposed bullet
Discussion
Myocardial involvement of HIV-infected patients is well established on clinical data, echocardiographic studies, macropathological findings and histological studies on autopsy or endomyocardial biopsy specimens. 9 Cardiac abnormalities can be detected in 40–60% of patients in necropsy series although clinical symptoms are infrequent. 10
HIV-associated cardiovascular manifestations may be detected even in the early stages of the disease, and are often clinically occult or attributed (incorrectly) to other disease process. 1 Cardiac pathological abnormalities in HIV disease are complex and most probably multifactorial and have been attributed to a direct myocardial effect of the virus (HIV infection of myocytes or dendritic cells), opportunistic infections, neoplasms, effects of treatment, autoimmunity and abnormalities in nutritional status.10–12
There is a wide variability concerning the incidence of systolic dysfunction in HIV patients, with the range being between 10 and 40%. 13 There is evidence from some retrospective studies that HAART might reduce the incidence of HIV-associated heart disease and improve its course by preventing opportunistic infections and reducing the incidence of encephalopathy. 14 The great divergence in the reported incidence of systolic dysfunction is presumably due to the various definitions of systolic dysfunction, in the differences in the disease stage of the patients studied, and in the inhomogeneity of the patients enrolled in each investigation.
Recent studies have identified a growing number of HIV-infected patients who develop unexplained LV dysfunction and congestive heart failure. 15 The incidence of dilated cardiomyopathy in the above patients is approximately 1.6% before the introduction of HAART and it is associated with a poor prognosis (median survival 101 days when compared with 472 days in patients with normal hearts who are at a similar stage of disease, with an adjusted hazard ratio of cardiac death of 5.86).3,11,16 The aetiology of dilated cardiomyopathy in HIV-infected patients is presently poorly understood. Clinical characteristics associated with severe symptomatic cardiac dysfunction include a low CD4 T-cell count, myocarditis associated with non-permissive cardiotropic virus infection on endomyocardial biopsy and persistent elevation of antiheart antibodies. 17
In this study, we found that patients with positive HIV serology, all in HAART, conventional echocardiography did not disclose any impairment in the global systolic function. The intensive medical treatment of our patients and the stage of the disease might have contributed to this finding. However, when DTI was applied, a significant reduction of the peak systolic myocardial velocities was found in HIV-infected patients, which correlated positively with CD4 lymphocyte count. As already mentioned, DTI estimates contractility in the longitudinal axis and reveals contraction abnormalities earlier when compared with the conventional echocardiographic study. 18 By applying the best possible cut-off point for Sms and Sml, we managed to discriminate patients from controls with a sensitivity and specificity of 76 and 77.7%, respectively, for the former parameter and 71 and 66.7%, respectively, for the later. In addition, with multiple logistic regression analysis both, Sml and Sms, were identified as independent disease predictors, with the OR being 0.33 and 0.68, respectively. Thus, DTI study has been proved able to unmask subtle and non-otherwise detectable systolic function abnormalities.
As cardiac involvement in HIV-infected patients affects negatively prognosis (in terms of both morbidity and mortality), an early recognition of systolic function abnormalities is crucial. Indeed, even subclinical echocardiographic abnormalities independently predict adverse outcomes and identify high-risk groups to target for early intervention and therapy. 3 Under this point of view, DTI, with its ability to reveal subtle systolic function abnormalities, might be used as a useful tool in the follow up of asymptomatic HIV-infected patients, aiming at identify precocious cardiac involvement and begin appropriate treatment. Long-term follow up will show whether patients with the lower velocities by DTI are more likely to develop overt LV dysfunction or signs of congestive heart failure. The impact of therapy to reduce progression (or cause regression) of systolic dysfunction, and whether this translates into improved survival remains, however, to be established from prospective studies.
Diastolic function abnormalities have also been described in HIV-infected patients with a very wide variability in its incidence in the various reports. These consisted of a reduced Emax, an increased peak of Amax, and an increased IVRT and early filling duration.10,19 Doppler-derived parameters of diastolic function have been found to be altered even in the asymptomatic HIV patients when compared with control subjects, while the LV diastolic indices were similar in symptomatic and asymptomatic HIV patients, except for posterior wall thinning, which was lower in the in the symptomatic HIV group. 19 In this investigation, although there was a trend for abnormality in TDI diastolic velocities, however, no statistical significant differences were found between groups, either with conventional echocardiography or DTI. A possible explanation is that the relatively small-sized study sample may have prevented us from reaching significant differences, or that impairment of long-axis LV contraction as detected with DTI, could precede the development of diastolic function abnormalities.
Study limitations
In our study population, the time from the diagnosis of HIV infection was different for each patient, and as a result the time period under therapy (or the period without therapy) differs among them. It would be of interest to study prospectively with serial DTI studies individuals with a recent exposition to HIV and assess in the long-term the impact of HIV infection and therapy to the longitudinal LV function.
Pulsed-wave TDI is angle dependent and is also affected from both, translation and rotation of the heart. However, as previously mentioned, every effort was made to obtain a Doppler angle of incidence close to 0°.