
Abstract
Summary:
The aim of the study was to compare the antimicrobial resistance pattern of Neisseria gonorrhoeae isolates from urban and rural peripheral health centres and from sexually transmitted disease (STD) clinic attendees. Antimicrobial susceptibility testing of 191 N. gonorrhoeae isolates (165 isolates from STD clinic attendees and 26 from peripheral health centres) was carried out in Delhi, India, using the calibrated dichotomous sensitivity technique for penicillin, tetracycline, ceftriaxone, ciprofloxacin, spectinomycin and nalidixic acid, and minimum inhibitory concentrations were determined using E-test. Penicillin-resistant, ciprofloxacin-resistant, penicillinase-producing N. gonorrhoeae and tetracycline-resistant N. gonorrhoeae strains were higher in STD clinic attendees than in peripheral health centres, probably because of less antibiotic pressure in the peripheral areas. High-level resistance to ciprofloxacin and multiresistant strains were also higher in STD clinic attendees. The present study emphasizes the importance of surveillance of antimicrobial resistance of N. gonorrhoeae in different population subgroups in order to monitor the spread of multiresistant strains and to update the national treatment recommendations.
Introduction
Gonorrhoea is one of the most common sexually transmitted diseases (STDs) in India and is also a global public health problem. The incidence/prevalence rates of gonorrhoea are difficult to ascertain because resources are mostly lacking where the disease is concentrated. 1 Some available estimates of incidence suggest that approximately 62 million new cases of gonorrhoea occur globally each year. 1 Despite a high prevalence of gonorrhoea, no regular monitoring of antimicrobial susceptibility of Neisseria gonorrhoeae is carried out in India and many other countries, the reasons being invasive specimen collection procedures, fastidious nature of the organism, need for specialized culture media and trained personnel. Moreover, as a consequence of emphasis on syndromic management of STDs and the introduction of non-culture-based diagnostic tests, there is decreased availability of N. gonorrhoeae isolates for susceptibility testing. 2 There has been a remarkable increase in antimicrobial resistance among N. gonorrhoeae isolates in many developing countries, throughout the southeast Asia Region in recent years, 3 8 but these studies were limited to the isolates from specialized populations, i.e. from sex workers or STD patients.
In India, most of the studies on antimicrobial susceptibility testing are limited to isolates obtained from patients attending STD clinics in tertiary care centres and isolates collected during a short period. 9 13 So far, no data on antimicrobial susceptibility on gonococci isolated from patients attending peripheral health centres are available.
The present study was undertaken to characterize the antimicrobial resistance profile of N. gonorrhoeae isolates from rural and urban peripheral health centres and to compare the antimicrobial resistance pattern of these isolates with that of isolates from STD clinic attendees of a tertiary care centre.
Methods
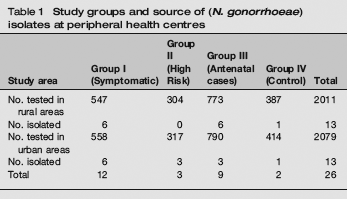
The study was carried out from March 2002 to April 2004 in women attending one urban and one rural government peripheral health centre each in four zones of Delhi. Hospital ethics committee approval was obtained. Endocervical swabs were collected from 2011 women from rural areas and 2079 from urban areas recruited under four study groups, e.g. Group I: symptomatic (women with symptoms of current vaginal/cervical discharge); Group II: high risk (women comprising of one or more sex partners/bad obstetric history/infertility/commercial sex workers); Group III: antenatal clinic attendees; Group IV: control group with patients from other clinics without any symptoms of STDs or reproductive tract infections (Table 1). In the peripheral health centres, swabs were collected in transport media (Stuart's) and were inoculated directly on chocolate agar and saponin-lysed blood agar with VCNT (vancomycin, colistin, nystatin, trimethoprim) inhibitors that were placed in a candle jar in a moist atmosphere immediately in the field and were transported to the STD Reference laboratory at Vardhman Mahavir Medical College and Safdarjang Hospital, New Delhi, within 4-6 hours. During the same period, urethral swabs from a total of 279 consecutive male patients clinically presenting with acute gonococcal urethritis and urethral and endocervical swabs from 1518 female patients with cervical/vaginal discharge were taken. These swabs were collected from the patients attending the male and female STD clinics, respectively, of Regional STD Teaching, Training and Research Centre of the same hospital taken. Gram-stained smears were examined for the presence of intracellular Gram-negative diplococci. The swabs were inoculated immediately on both the above media and the inoculated culture plates immediately transported to the same STD Reference laboratory, adjacent to the STD clinic of the Centre. Concurrent chlamydia infection was detected by enzyme-linked immunosorbent assay for antigen detection (BIO-RAD kit [BIO-RAD Laboratories, Redmond, WA, USA]).
Study groups and source of (N. gonorrhoeae) isolates at peripheral health centres
In the laboratory, the swabs in transport media, collected from the periphery, were inoculated on both the media and the plates were incubated in 5% CO2 jar in a moist atmosphere at 36°C for 24-48 hours. N. gonorrhoeae were identified on the basis of colony morphology, Gram staining, oxidase, superoxol and rapid carbohydrate utilization test. 14 β-lactamase production was detected by the chromogenic cephalosporin method using nitrocefin freeze-dried powder (Oxoid [OXOID Ltd, Basingstoke, Hants, UK]). 14
Susceptibility testing of 26 N. gonorrhoeae isolates, 13 from urban women and 13 from rural women, from peripheral health centres (Table 1) and 165 isolates from STD clinic attendees was carried out by the disc diffusion method based on calibrated dichotomous sensitivity technique for penicillin (0.5 IU), tetracycline (10 μg), ceftriaxone (0.5 μg), ciprofloxacin (1 μg), spectinomycin (100 μg) and nalidixic acid (30 μg). The strains were defined as susceptible, less sensitive and resistant.14,15 Multiresistant isolates were defined as quinolone-resistant N. gonorrhoeae (QRNG) and penicillinase-producing N. gonorrhoeae (PPNG); QRNG and tetracycline-resistant N. gonorrhoeae (TRNG); QRNG, PPNG and TRNG. 16 The minimum inhibitory concentrations (MICs) of penicillin, tetracycline, ciprofloxacin, spectinomycin and ceftriaxone were determined by the E-test method following the manufacturer's instructions (AB Biodisk, Solna, Sweden). World Health Organization reference strains A to E were used as controls.
Statistical analysis was carried out by comparing the differences in percentages statistically, tested for significance by using the chi-square test and P values were determined.
Results
Isolation rate of N. gonorrhoeae from the transport media and from the direct inoculation of culture plates in peripheral health centres was identical. It may be due to the fact that all the samples and culture plates were transported to the laboratory within 4-6 hours. N. gonorrhoeae was isolated from women from all groups, predominantly from women with current symptoms of STI. However, antenatal cases and asymptomatic controls also harboured the organism (Table 1). Concurrent chlamydia infection was detected in one case each from peripheral health centres and STD clinic attendees.
Table 2 shows the antimicrobial resistance pattern of 26 N. gonorrhoeae isolates from peripheral health centres of different study areas. It is difficult to interpret the difference between urban and rural areas as the numbers of isolates from both the areas were very few. However, there was no remarkable difference in the resistance pattern of isolates from different zones in urban and rural areas except ciprofloxacin resistance, which was more in urban areas (12 out of 13) than in rural areas (8 out of 13).
Antimicrobial resistance pattern in different study areas
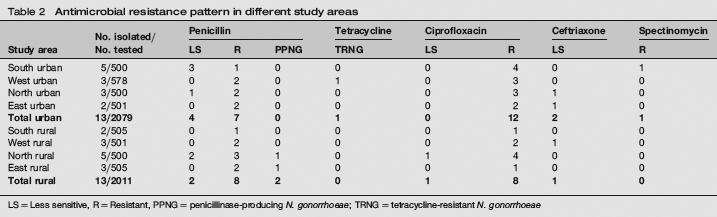
LS = Less sensitive, R = Resistant, PPNG = penicillinase-producing N. gonorrhoeae; TRNG = tetracycline-resistant N. gonorrhoeae
Comparison of the antimicrobial resistance patterns of N. gonorrhoeae isolates from peripheral health centres and 165 isolates from STD clinic attendees by the disc diffusion method is shown in Table 3. Penicillin-resistant (χ2 = 0.27, P > 0.50), penicillin less-sensitive strains (χ2 = 0.57, P <0.50), PPNG (χ2 = 3.79, P > 0.05), TRNG (χ2 = 1.25, P < 0.50) and ciprofloxacin less-sensitive strains (χ2 = 0.41, P > 0.50) were observed to be higher in STD clinic attendees than in peripheral health centres but the differences were statistically insignificant. Ciprofloxacin resistance was significantly higher in STD clinic attendees (χ2 = 4.49, P < 0.05). Significant high-level resistance (HLR) to ciprofloxacin (MIC ≥ 4 μg/mL) was observed in 46 (27.9%) isolates for STD clinic attendees, whereas none of the isolate was HLR from peripheral health centres (χ2 = 9.56, P < 0.01). In contrast, ceftriaxone less-sensitive strains were significantly higher in peripheral health centres (χ2 = 13.09, P < 0.001). Only one strain was resistant to spectinomycin as reported earlier. 17
Antimicrobial susceptibility pattern of N. gonorrhoeae isolates from peripheral health centres and sexually transmitted disease (STD) clinic attendees

HLR = High-level resistance (minimum inhibitory concentration [MIC] of ≥ 4 μg/mL); LS = less sensitive; R = resistant; PPNG = penicillin-producing N. gonorrhoeae; TRNG = tetracycline-resistant N. gonorrhoeae
Only two strains (7.7%) were observed to be multiresistant from peripheral health centres, i.e. one QRNG and TRNG from West urban area and one QRNG and PPNG from North rural area, whereas 37 (22.4%) strains from STD clinic attendees were multiresistant (χ2 = 2.27). Of these 37 strains, 20 (12.1%) were QRNG and PPNG, six (3.6%) QRNG, PPNG and TRNG and 4 (2.4%) were QRNG and TRNG.
Discussion
The present study is the first report from India comparing antimicrobial resistance patterns of N. gonorrhoeae isolates from peripheral health centres and STD clinic attendees contemporaneously. The number of isolates collected varied between the two types of set-ups. The tertiary health centres cater to clients of commercial sex workers, whereas the women attending the peripheral centres have almost always acquired the strains from their spouses. Fortunately, antimicrobial resistance to all the antimicrobials except ceftriaxone was lower in the strains in the peripheral health set-ups, than in the isolates from STD clinic, probably because of less antibiotic pressure in the peripheral areas. The study also confirms the absence of dissemination of multidrug-resistant strains to the periphery. It has been reported earlier that there is a diversity of gonococcal subtypes in different patient subgroups and geographical areas, often with differing antibiotic resistance profiles.2,18 The higher percentage of ceftriaxone less-sensitive strains from peripheral health centres could be because of the indiscriminate use of injectable antimicrobials by private practitioners in peripheral areas.
To conclude, antimicrobial resistance is much higher in STD clinic attendees than in peripheral health centres. Therefore, periodic surveillance of antimicrobial susceptibility of N. gonorrhoeae is essential to monitor the dissemination of drug-resistant strains from the high-risk individuals to the general population.
Footnotes
Acknowledgements
The authors acknowledge Indian Council of Medical Research, New Delhi, for providing financial assistance for carrying out the study in the peripheral health centres. The authors are indebted to Professor John W. Tapsall and Ms Athena Limnios, WHO collaborating centre for STD and HIV, Department of Microbiology, The Prince of Wales Hospital, Sydney, Australia for supplying low-concentration antibiotic discs and WHO Reference strains. We thank the Medical Superintendent, VMMC and Safdarjang Hospital for permitting us to carry out this study and Smt Leelamma Peter for technical assistance.