
Abstract
Women reluctant to undergo a per-speculum examination consider self-sampling more acceptable. The aim of this study was to compare self-collected vaginal swabs for detection of bacterial vaginosis (BV), candidiasis and trichomoniasis, with vaginal specimens obtained by the gynaecologist at per-speculum examination. Self-collected and provider-collected vaginal swabs were obtained from 50 women attending the gynaecological outpatients department. The Gram-stained smears and saline wet mounts prepared from the provider-collected vaginal swabs were examined by a microbiologist and a gynaecologist. We determined the validity and the inter-rater reliability of the overall BV score and the morphotype specific score using Kappa statistics. When compared with the provider-collected smear, the ability of the self-collected smear to diagnose BV had a sensitivity of 70% and a specificity of 97%. With specific instructions to help assure the depth of sampling, self-collected swabs can reasonably approximate specimens obtained by clinicians during speculum examination for the diagnosis of BV.
Introduction
Bacterial vaginosis (BV) is a vaginal condition involving a reduction in the normal amount of hydrogen peroxide-producing lactobacillus and an overgrowth of anaerobic and Gram-negative or Gram-variable bacteria, including Bacteroides spp., Mobiluncus spp., Gardnerella vaginalis and Mycoplasma hominis. 1 BV is one of the most common lower genital tract infections and the number one cause of vaginitis among women of childbearing age. 2 In developing countries, due to the absence of cheap, simple and accurate diagnostic tests or comprehensive laboratory services for microbiological diagnosis, World Health Organization (WHO) has developed syndromic management guidelines for treatment of sexually transmitted infections. 3 The syndromic approach uses clinical algorithms based on patients’ symptoms and clinical signs without offering any laboratory-based diagnosis. Concern has been raised about the use of syndromic management in vaginal discharge as it may lead to overtreatment. 4 The wide range of symptoms displayed in cases of BV and the high proportion of asymptomatic infections make it a difficult syndrome to diagnose. Also, there is a poor concordance between self-reported symptoms and laboratory confirmed reproductive tract infections (RTIs), limiting the usefulness of the syndromic approach to the management of RTIs. 5 Hence, it would be better to provide specific treatment based on the aetiological diagnosis obtained after subjecting these women to few simple laboratory tests. However, women may be reluctant to undergo a per-speculum/pelvic examination, which is required for collection of samples for lab tests because of lack of privacy, non-availability of a female doctor in a health-care facility, apprehension and discomfort. 6 Self-sampling the vagina seems to be very acceptable to women of multiple ethnic groups. 7 Self-obtained vaginal swabs have been successfully used for the diagnosis of several vaginal infections, including group B streptococcus 8 , Chlamydia trachomatis 9 and BV. 10 But only few studies 11 have compared the validity of self-collected with provider-collected swabs to diagnosis BV in a predominantly illiterate community coming to a tertiary centre.
The aim of this study was to evaluate the feasibility, acceptability and reliability of self-collected vaginal swabs for detection of BV, candidiasis and trichomoniasis when compared with vaginal specimens obtained by the gynaecologist at per-speculum examination.
Material and Methods
Fifty sexually active women between 20 and 45 years of age attending the gynaecological outpatients department of Lok Nayak Hospital, New Delhi, with a complaint of vaginal discharge were included in the study. Self-collected and provider-collected vaginal swabs were obtained from each participant during the same visit for preparation of smears and saline wet mounts.
For self-collection of vaginal swab, women were verbally instructed to hold a cotton tip swab between their thumb and index finger and insert the swab at least 0.025 M into the vaginal vault without causing any discomfort, as described by earlier investigators. 12 They were then instructed to rotate the swab while attempting to touch the vaginal sidewalls and withdraw it. The gynaecologist would then do a per-speculum examination and collect a vaginal swab. The self-collected and provider-collected vaginal swabs were immediately used on site to prepare smears for Gram staining and saline wet mounts by the microbiologist. Saline wet mounts were examined at 400 × for detection of Trichomonas vaginalis. The vaginal smears were stained by the Gram-staining method using crystal violet as the primary stain, acetone as the decolourizer and saffranine as counter stain. Gram-stained smears were examined at 1000 × magnification in oil immersion for the diagnosis of BV and candidiasis. The diagnosis of BV was made on the basis of criteria described by Nugent et al. 13 After specimen collection, participants were asked about their preference concerning either method of swab collection along with reasons, and the details were noted in a pre-designed proforma.
The Gram-stained smears and saline wet mounts prepared from the provider-collected vaginal swabs from each patient were read blind by a microbiologist and a gynaecologist.
We determined the validity (comparing results of self-collected to provider-collected swabs) and the inter-rater reliability (comparing results from a microbiologist and a gynaecologist) of the overall BV score and the morphotypespecific score using Kappa statistics.
Results
In this study, 50 patients were recruited from the Department of Obstetrics and Gynaecology, Lok Nayak Hospital. Samples were collected from the patients attending the gynaecology outpatient department, and the tests were performed at the department of Microbiology, Maulana Azad Medical College, New Delhi.
Since one smear prepared from the self-collected vaginal swab showed scanty material, 49 smears were considered valid for analysis.
Validity assessment
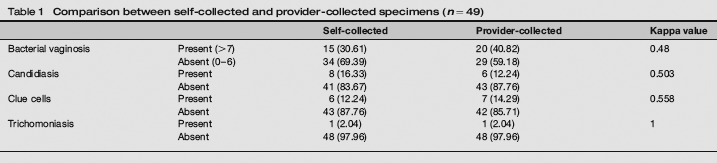
Table 1 shows the comparison between self-collected and provider-collected specimens for detection of BV, candidiasis, clue cells and trichomoniasis. BV was detected in 20 (40.82%) women in smears prepared from provider-collected swabs, whereas it was detected in 15 (30.61%) women in smears prepared from self-collected swabs (k = 0.48). However, candidiasis was more frequently detected in the self-collected swabs (16.33 %) when compared with provider-collected swabs (12.24%) (k = 0.503). The presence of clue cells as reported by both the techniques also showed moderate agreement (k = 0.558). When compared with the provider-obtained smear, the ability of the self-obtained smear to diagnose BV had a sensitivity of 70%, specificity of 97%, positive predictive value of 93%, negative predictive value of 83% and total predictive value of 86%. The wet mount findings in the self-obtained versus physician-obtained swabs showed complete agreement for T. vaginalis (k= 1.0).
Comparison between self-collected and provider-collected specimens (n = 49)
The vaginal-flora scores of vaginal smears prepared from self-collected and provider-collected specimens were cross-tabulated into three grades (0-3 = normal, 4-6 = intermediate, 7-10 = BV) and compared. The results (Table 2) showed a significant correlation (χ2 = 32.82, P = 0.00) between the two techniques in the ability to determine the grade of vaginal micro flora.
Comparison of Gram-stained vaginal fluid collected by the two techniques using dichotomous coding of vaginal-flora score (n = 49)
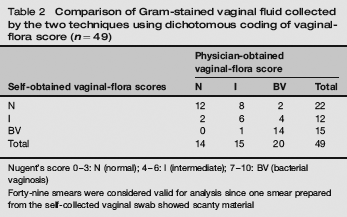
Nugent's score 0-3: N (normal); 4-6: l (intermediate); 7-10: BV (bacterial vaginosis)
Forty-nine smears were considered valid for analysis since one smear prepared from the self-collected vaginal swab showed scanty material
Inter-rater reliability
Table 3 shows the comparison between the results reported by a microbiologist and a gynaecologist.
Comparison between the results reported by a microbiologist and a gynaecologist in provider-collected swabs (n = 50)
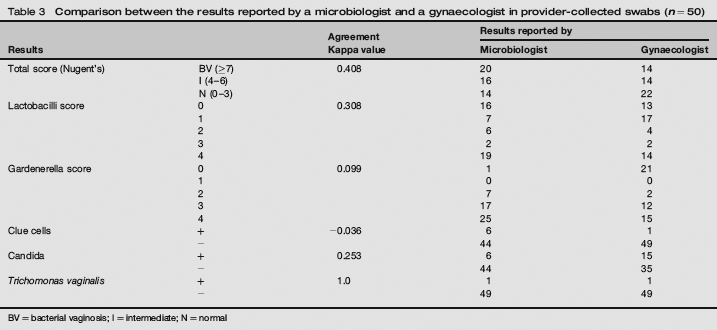
BV = bacterial vaginosis; l = intermediate; N = normal
We found moderate inter-rater agreement between the microbiologist and the gynaecologist in the ability to differentiate BV from non-BV cases (k = 0.408). The gynaecologist reported BV in 28% of cases, whereas the microbiologist reported it in 40% of cases. The inter-rater agreement for the scores of the individual morphotypes between the microbiologist and the gynaecologist was fair for lactobacilli morphotype (k = 0.308) but poor for gardnerella morphotype (k = 0.099). Clue cells were detected in 6 (12%) of the provider-collected specimens by the microbiologist, whereas it was detected in only 1 (2%) by the gynaecologist (k = -0.036). However, candidiasis was more frequently reported (30%) by the gynaecologist when compared with the microbiologist (12%) (k = 0.253). The wet mount findings for T. vaginalis showed complete agreement between the microbiologist and the gynaecologist (k = 1).
Self-collection of distal vaginal swabs was reported as easy to perform by majority of participants 45 (90%). Three (6%) preferred swabs collected by gynaecologists, and the most common reasons given were lack of confidence and pain while collecting swabs themselves. Two (4%) women felt that both methods were equally acceptable.
Discussion
Current RTI-control efforts are hampered by barriers, existing at the individual, provider and community levels, to the delivery of quality health care to those at risk. Once the individual has recognized the need to seek care, the decision whether and where to do so is often influenced by fear of undergoing a painful examination, concerns of confidentiality and the stigma associated with RTIs. Low participation rates for gynaecological examination and low reliability of clinical reporting of gynaecological examination findings are problems in community studies of gynaecological morbidity in India.
Vaginal discharge is the most common morbidity reported from the women with lower genital tract infections in our country. 2 Using syndromic approach, the management of vaginal discharge has been difficult owing to the number and diversity of pathogens, resulting in overtreatment. 4 Therefore, the recommended treatment is based on the most common causative organisms. Hence, an aetiological diagnostic method will be valuable to provide specific treatment to those who need it. Among the simple tests that can be done in the out-patient department to diagnose BV, such as the assessment of intra-vaginal pH and clinical signs 14 , the Gram-stain microscopic evaluation of vaginal secretions to assess the relative concentrations of bacterial morphotypes is the most commonly used.
Blind swabbing of the vagina appears to have a high degree of acceptability to women, and they can perform it themselves. Our data demonstrate that with specific instructions to help assure depth of sampling, self-obtained swabs can reasonably approximate specimens obtained by clinicians during speculum examination. Other authors have reported the ability of vaginal swabs to diagnose BV. Nelson et al. 1 have found that self-collected vaginal swabs have an excellent agreement for the overall diagnosis of BV among pregnant women compared with provider-collected swabs (k = 0.94), and in one report from India 11 , there was a high agreement between the two sets of specimens (k = 0.98, P < 0.001). Unlike the above reports, our study has found that the reliability of specimens collected using self-administered swabs for the detection of BV is moderate (k = 0.48) when compared with gynaecologist-administered swabs. Our study shows that when compared with the provider-collected smear, the ability of the self-collected smear to diagnose BV had a sensitivity of 70%, specificity of 97%, positive predictive value of 93% and negative predictive value of 83% comparable with earlier reports. 15 However, the low Kappa value obtained in our study comparing these two techniques could be because of the predominantly illiterate population our hospital caters to, because earlier studies, 11 which have reported high agreement between the two sets of specimens with a Kappa value of 0.98, had only 25% of their study population as illiterate. The ability of the self-collected smear to diagnose candidiasis had a sensitivity of 75%, specificity of 91.5%, positive predictive value of only 60% and a negative predictive value of 95.5% when compared with provider-collected smears.
In our study, we have also evaluated the inter-rater reliability of the overall BV score and the individual morphotype score between a microbiologist and a gynaecologist, which to the best of our knowledge, has not been previously reported from our country. When it comes to the ability to differentiate BV from non-BV cases, our study showed moderate agreement between a microbiologist and a gynaecologist (k = 0.408). Using the microbiologist observations as the reference gold standard, the diagnosis of BV and non-BV cases by the gynaecologist had a sensitivity of 76.9%, specificity of 96.8%, positive predictive value of 95.2% and a negative predictive value of 83.3%. Coming to the individual morphotypes, however, the lowest agreement was obtained for gardnarella morphotype and for the presence of clue cells. As far as the diagnosis of candidiasis was concerned, an over-diagnosis was made by the gynaecologist with a sensitivity of 75%, specificity of 80%, positive predictive value of 35.3% and a negative predictive value of 95.6%. In our study, the majority (90%) of the women attending a gynaecological outpatient department preferred self-administered swabs unlike one report from India 11 that showed a lower percentage (29%) of women who preferred self-sampling.
Though our study shows moderate agreement between self-collected and provider-collected swabs for the diagnosis of BV, self-collected swabs have a great potential for surveillance of RTIs in settings where either women do not wish to be examined, or cannot access gynaecological clinics. Although there have been reports of their use in Africa and in developed countries12,16,17, to the best of our knowledge, there is only one report of their use in India. 11 Also, our results suggest that it would be preferable if a microbiologist rather than a gynaecologist evaluates a Gram-stained smear for the diagnosis of BV and candidiasis to reach a correct interpretation and start appropriate treatment.