
Abstract
The World Health Organization estimates that at least 12 million people are infected with syphilis in the world. Southeast Asia accounts for 5.8 million; Africa accounts for 3.5 million. There has been controversy in using the two kinds of antibiotics for early syphilis. A systematic review comparing these antibiotics could affect treatment guidelines. The aim of this study was to evaluate the efficacy and safety of azithromycin vs. penicillin G benzathine for early syphilis and a meta-analysis to compare these two kinds of antibiotics for early syphilis. Four randomized controlled trials met the inclusion criteria; 476 patients were evaluated for their cure rate. Cure rates were 95.0% (227/239) for azithromycin and 84.0% (199/237) for penicillin G benzathine. After pooling the data, the difference in efficacy was computed. Cure rate (OR = 1.37), 95% CI (1.05, 1.77) and the risk difference for cure rate between the two drugs were statistically significant. Although the gastrointestinal adverse effect of azithromycin is five times more than the adverse effect of penicillin G benzathine, the differences are not significant. Azithromycin achieved a higher cure rate than penicillin G benzathine in a long follow-up.
Introduction
Syphilis is a complex systemic disease with protean manifestations and virtually any organ in the body can be involved. It has been described in medicine as the great imitator or the great imposter in view of the multiple possible clinical tests. It is certain that syphilis is caused by the spirochete, Treponema pallidum (T. pallidum).1,2 Syphilis is usually transmitted by sexual contact and, unfortunately, it is difficult to kill through isolation and characterization of the causative organism. 2 The World Health Organization estimated that at least 12 million people are infected with syphilis worldwide. Southeast Asia accounts for 5.8 million; Africa accounts for 3.5 million. 2
There is limited cure with antibiotics other than penicillin G benzathine for early syphilis. 3 Erythromycin has been associated with a high failure rate. 2 Doctors usually use penicillin benzathine G, erythromycin, cephamycin, ambramycin to treat early syphilis. 4 According to the epidemic prevention bureau of the Ministry of Public Health, if procaine benzylpenicillin, bicillin G, benzathine penicillin G are hypersensitive and not suitable for use, ambramycin or azithromycin will be used instead. Although hospitals often make use of procaine benzylpenicillin for early syphilis, the efficacy of penicillin G benzathine is not steady and is ineffective where patients are co-infected with AIDS. The disadvantages of benzathine penicillin G include the need for large volume (4 mL), deep, intramuscular injection equipment and medically trained personnel, which may be lacking in countries with few health resources. 4 Fortunately, some pilot studies have suggested that efficacy of azithromycin is superior to benzathine penicillin G in the treatment of early syphilis and that azithromycin can overcome the disadvantages of benzathine. Notwithstanding, in 2007, Lukehart published a study in the New England Journal of Medicine that found almost 90% of samples taken in Dublin, Ireland, and nearly 40% of samples of T. pallidum taken in San Francisco, USA, contained a genetic mutation making it resistant to azithromycin. 5
With the increasing incidence of syphilis including early syphilis and reports of apparent non-response to current antibiotic regimens, questions have been more frequently raised about whether the standard regimens to treat early syphilis are optimal and effective. 3 A review 11 in 2001 also showed no significant difference between the mentioned regimens; however, this review did not include all trials comparing azithromycin with benzathine, did not account for study size or quality and did not include other patients besides pregnant women; the included study types were non-randomized trials. In addition to antibiotic efficacy, safety must be considered in determining an appropriate therapy. The reported frequency of adverse events is similar for both medications.
In the current study, we used formal statistical methods (meta-analysis) to determine whether azithromycin or benzathine penicillin G is more efficacious and safe in the treatment of early syphilis.
Methods
Study selection
The study protocol was approved by the Evidence-Based Medicine Centre of LanZhou University. The methodology was conducted by the China Cochrane Centre.
One of the studies included had two azithromycin groups and one benzathine penicillin G group, so the data were extracted as two reviews.7,10
Published English language studies were identified by an exhaustive computer search with use of the following databases: MEDLINE and Pre-MEDLINE (1975–October 2006), COCHRANE-LIBRARY (2006, third issue), EMBASE (1974–October 2006), CBM (1978–October 2006), Journal at Ovid Full Text (October 2006), Evidence-Based Medicine (EBM) Reviews. Bibliographies of computer-identified articles were searched manually for additional trials for inclusion. Cochrane Sexually Transmitted Infection Group's Register of Controlled Trials (August 2006), The Reproductive Health and Research Department, Family and Community Health cluster at WHO, Geneva, National Center for HIV, STD and TB prevention, Centers for Disease Control and Prevention, conference recording and grey literature were also searched. Cochrane Pregnancy and Childbirth Group search strategy. The search was developed iteratively for synonyms of ‘syphilis’, ‘benzathine penicillin G’, ‘azithromycin’.
Three authors (ZHGB, KHY, JHT) independently evaluated all trials comparing benzathine penicillin G with azithromycin for treatment of early syphilis. Criteria for inclusion in the analysis were: (1) randomized trial design; (2) medication regimens of oral azithromycin; (3) age >18 years; (4) evaluation of cure rate in follow up. The cure was defined as rapid plasma reagin (RPR) remaining negative in serological examination after treatment. Studies were excluded if they did not fulfil all of the aforementioned criteria.
For follow-up, the last available time slots were selected. The most commonly reported follow-up times were three, six and nine months. Two studies reported that the presented data are from primary syphilis. Four studies presented data from different dosages of azithromycin. Also, there was cumulative data from undifferentiated follow up and primary syphilis.
Data extraction
Data were extracted from selected studies. Serological cure at the different available follow-up times and number of patients who had adverse effects were tabulated. Attrition rates based on last available follow-up were calculated with the intention-to-treat analytical approach.
Statistical methods
For each trial, the odds ratio (OR) of treatment success for azithromycin vs. benzathine was computed. The numerator and treatment success were defined as the number of subjects assigned to a particular antibiotic group who complied with the treatment regimen and were serologically cured at follow up. The denominator for computing treatment success comprised all subjects assigned to an antibiotic group who began the medication. To pool dichotomous outcomes (serologic cure vs. no serologic cure), an overall weighted average of the OR from each trial was calculated by assigning each one a weight derived from the standard error of the OR. Thus, each trial's contribution to the pooled estimate of OR is directly proportional to the amount of information provided.
Subjects lost to follow-up were excluded from the analysis. Each pooled OR was tested for statistical significance, and 95% CI were computed. In computing the pooled estimates, it was assumed that OR was uniform across trials and that differences in results of individual trials could be attributed to chance. Hence, a fixed effects model was used. A chi-square test of homogeneity was used to test the assumption of uniform OR.
A stratified meta-analysis was performed to assess possible bias in the results. Data were stratified by various subgroups: types of follow-up (three, six and nine months); different staging of early syphilis (primary syphilis); different dosages of azithromycin (0.5, 2.0 and 4.0 g). To increase statistical power, a P value of 0.05 was used as the criterion for determining statistical significance of the tests for publication bias.
Results
Five trials fulfilling the inclusion criteria were identified. One was excluded because the data for the benzathine treatment group were not segregated from those for several other antibiotic treatment groups. Four of the five included studies, three were masked and one was open-label. Adverse event data were provided from two trials. Publication dates ranged from 1999 to 2005, and two studies were conducted in 2005. For evaluation of serology cure, four studies used RPR.
A total of 476 patients were evaluated for serology cure. In the azithromycin group, serology cure occurred in 227 of 239 patients (95.0%). In the benzathine penicillin G group, serology cure occurred in 199 of 237 (84.0%). Figure 1 specifies the selection of the studies. Table 1 contains specific information on study design, random methods, samples size, sex of patients, serology cure rate and follow up.

The flow chart of this paper
Attributes of the studies used for meta-analysis of genital azithromycin treatment

Figure 2 shows the pooled OR for serology cure of azithromycin vs. benzathine penicillin G. The pooled OR is 1.37 (95% CI: 1.05, 1.77). This result is statistically significant (Z = 2.36; P = 0.02). The test for homogeneity shows that results for individual trials are consistent with the overall pooled OR (χ 2 = 8.67; df =10; P = 0.56, I2 = 0%).
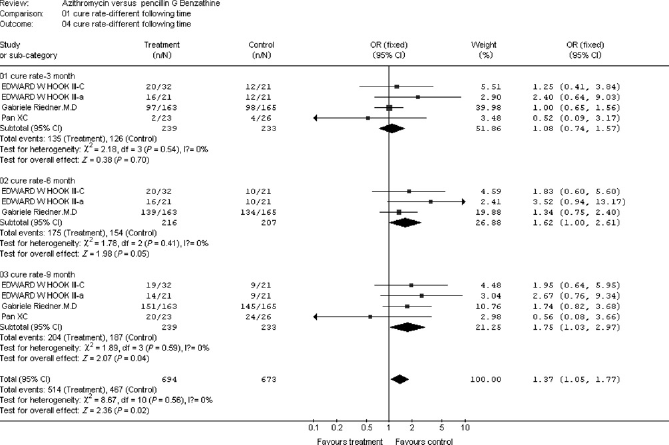
Cure rate of syphilis at different follow-up times
The OR for primary syphilis with administration of azithromycin vs. benzathine penicillin G was shown in Figure 3. The pooled OR is 0.69, (95% CI: 0.09–1.61). This result is not statistically significant (Z = 0.87; P = 0.38). The test for homogeneity shows that the results are consistent across trials (χ 2 = 0.19; df = 1; P = 0.66, I2 = 0%).
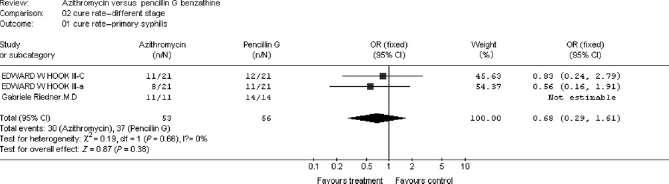
Cure rate of primary syphilis
The analysis result of different dosage drug was demonstrated in Figure 4. The pooled OR is 1.76 (95% CI: 0.92–3.33). This result is not statistically significant (Z = 1.69; P = 0.09). The test for homogeneity shows that the results are consistent across trials (χ 2 = 1.67; df =3; P = 0.64, I2 = 0%).
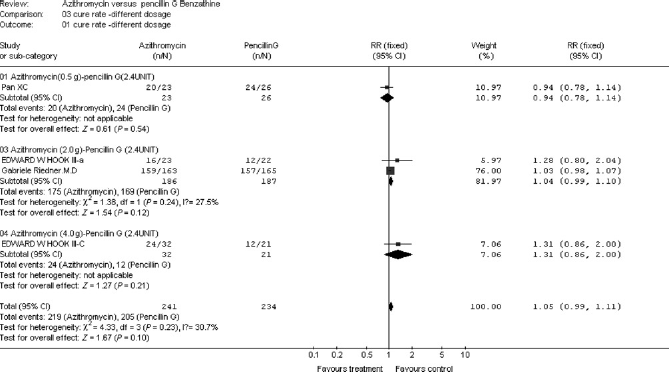
Cure rate at different dosages
We stratified the data by various subgroups to assess possible bias in the results. Results showed no evidence of bias by type or by follow-up time (three, six, nine months), different staging of disease, or different dosages of azithromycin.
Discussion
In this review involving four papers,4,7,8,10 it was found that azithromycin had a higher cure rate than benzathine penicillin G for early syphilis. All meta-analyses are subject to potential bias because of systematic and random errors. However, our results show no evidence of systematic bias by assay follow-up time, different staging of the disease, or different dosages for azithromycin. Estimates of pooled effects are homogenous, indicating that the magnitude of random error is not greater than expected.
Azithromycin has a higher cure rate than benzathine penicillin G. Riedner's results 4 were similar to this study, since there were no investigations reporting the cure rate of the second stage of syphilis and latent syphilis. It is important to perfect these two kinds of staging of syphilis in the later clinical trial.
There was no report of a randomized trial that by directly comparing azithromycin with benzathine penicillin G gave adverse events. The eligible randomized clinical trials enrolled were few, owing to three studies4,7,10 referring to the adverse events. The adverse events include Jarisch–Herxheiner reactions and gastrointestinal problems. Three reviews4,7,10 reported that the adverse events with azithromycin are five times the benzathine penicillin G side-effect, but the difference is not significant (OR = 4.75; 95% CI, 0.67–33.9; P = 0.09).7,10
Compliance of patients is a critical consideration in treatment decisions. Administration of benzathine penicillin G involves a twice-daily regimen, whereas azithromycin is given as a one-time dose. Because patients are more likely to take azithromycin as prescribed and there is no difference in cure rates, one might conclude that azithromycin is the treatment of choice. Moreover, the 60-hour half-life of azithromycin suggests that adequate serum consent ratios will be maintained with a once-daily protocol. Of course, the pool OR for different dosages of azithromycin illustrate that there is no difference in effect between azithromycin and benzathine penicillin G for early syphilis. Although observational studies suggest that partial compliance with benzathine penicillin G is sufficient to effect cure, quality dose–response trials are needed to evaluate these findings.
The marked cost differential between single-dose and multidose therapy makes the medication choice a central issue in the current environment of limited resources. Hence, there is controversy about the regimen of choice for uncomplicated genital syphilis infection. Generic supplies of the drug, made in India, have been available for some years at a cost of approximately $1.20 for a 2 g dose. 12 Azithromycin came off patent in the USA in November 2005. Although penicillin G benzathine is an inexpensive drug, the cost of administering it has to include the cost of the needle and syringe. Two major cost-effectiveness studies comparing the antibiotics concluded that azithromycin is more cost-effective. Unfortunately, not all of the eligible studies illustrated the cost of the two targeted antibiotics. Since these assumptions are unlikely to be accurate, a comprehensive cost-effectiveness analysis should be performed.
Finally, azithromycin is more effective than benzathine penicillin G at a dosage of 2.4 million units, which is similar to the latest American studies reporting that the resistance of azithromycin is greater than benzathine penicillin G. No difference in adverse event rates was found. Dose–response trials may also be needed to evaluate less complicated azithromycin regimens. According to other research, it seems that azithromycin is a good choice, especially when the usage of benzathine penicillin G is problematic or where patients are intolerant of the drug. Further study on the utility of benzathine penicillin G for early syphilis is warranted.
Footnotes
Acknowledgements
Our thanks to all co-authors for their significant contributions. All authors are in agreement with the content of the manuscript. We are grateful to the Cochrane Center for China for their help and support.