
Abstract
This study is a systematic literature review exploring the efficacy of antiretroviral therapy (ART) in Africa through a meta-analysis of immunological and virological outcome measures at baseline and six subsequent time points. A literature search was conducted through two databases and references of relevant papers searched. The inclusion criteria were papers with data from the African continent with predominantly an adult population, who were ART naïve and human immunodefieciency virus-1-positive, data on the CD4 count and/or percentage undetectable viral load (UDVL) at a subsequent time-point following ART initiation. The search identified 368 papers. Of these 320 were excluded by title and abstract, 48 papers were accessed with a further 19 papers then excluded. Twenty-nine papers from 12 countries were included in the meta-analysis. All papers showed evidences of Grade III or IV. The mean CD4 count (cells/mm3) at baseline was 141.0 and viral load was 5.2 log10. The mean CD4 count was 243.8, 248.9, 277.1, 274.1, 298.4, 374 at 3, 6, 12, 18, 24 and >24 months, respectively. The mean percentage with UDVL was 73.3, 74.7, 66.9, 68.1, 64.6, 73.5 at 3, 6, 12, 18, 24 and >24 months, respectively. In conclusion, the meta-analysis provides evidence that ART increases the CD4 count from three months until three years, and the majority of subjects had an UDVL (<400 copies/mL) at each analysed time-point. Though the grade of evidence is low, this analysis suggests that ART can be provided successfully within the continent of Africa even with the limitations of a resource-poor setting.
Introduction
Since the development and introduction of antiretroviral therapy (ART) over the last decade, the clinical course of the human immunodeficiency virus (HIV) infection in the developed world has been transformed from a terminal condition to a chronic disease requiring longterm management. 1 However, in developing countries ART remains inaccessible to the vast majority of their populations 2 resulting in continuing high morbidity and mortality. The number of people infected with HIV was estimated to be 39.5 million in 2006 of which approximately two-thirds of these people were living in sub-Saharan Africa. The HIV epidemic continues to grow with an estimated 4.3 million people in 2006 being newly infected and 2.1 million people dying from acquired immunodeficiency syndrome (AIDS) (72% of these people living in sub-Saharan Africa). 3 As of June 2006, 23% of those requiring ART within this region were receiving the appropriate treatment with the remaining 77% urgently requiring ART but having no access. 3
In 2003 Dr Lee Jong-Wook, the Director General of the World Health Organization (WHO) called the HIV epidemic a ‘catastrophe’ 4 and the WHO initiated a campaign called ‘3 by 5’ with the primary aim of providing three million people from low- and middle-income countries with highly active antiretroviral therapy (HAART) by the year 2005. 2 Since the initiation of this campaign and until June 2006, globally a four-fold rise in access to HAART was observed; in sub-Saharan Africa this increase was 10-fold (from 7% to 23%). 3 A new inter-agency initiative called ‘Universal access by 2010’ was established following the agreement of international goals (including those relating to HIV) at the G8 summit in summer 2005. 5 This is currently the driving force behind the efforts to scale-up access to HAART.
Successful treatment of HIV/AIDS is multifactorial. 6 Research data on ART are predominantly collected from the developed world; thus generalizing this data to developing countries would be problematic because of the wide disparity of physical, social, cultural and financial factors, which exist. This illustrates the necessity of gaining greater understanding of how ART affects the outcome of HIV in developing countries and particularly important is the analysis of data from Africa where the epidemic has led to the most devastating consequences.
Even with the involvement of internationally respected organizations such as the WHO and Joint United Nations Programme on HIV/AIDS (UNAIDS) emphasizing the urgency to scale-up HAART, voices have been raised with concerns about its effectiveness within Africa. 7 A major concern is the potential for poor adherence levels and the fear of a subsequent rise in the development and transmission of drug-resistant strains of HIV. Data from one study, which compared the effect of ART on Africans living in the UK with their Caucasian counterparts, reported poorer longterm response in the African population after an equal short-term response in the two populations. 8 This data suggest that a further cause for concern is the longterm outcome of using ART in an African population.
The aim of this study was to explore the efficacy of ART by observing its effect on immunological and virological outcome measures of HIV by the comparison of baseline data with data at subsequent predefined time-points following ART initiation. Currently, no systematic literature review or meta-analysis has been conducted to evaluate the efficacy of ART for the African continent. One literature review 9 was published aggregating data for resource-poor settings including 10 studies conducted in Africa. This present study will specifically focus on Africa and include the most recent data for analysis, thereby adding further evidence to the current knowledge base.
Methodology
A literature search was conducted using a preselected list of search terms to identify relevant literature through the OVID and PubMed databases. Search terms used were ‘human immunodeficiency virus’ or ‘HIV’ or ‘HIV-1’, or ‘acquired immunodeficiency syndrome’ or ‘AIDS’ and ‘Africa’ (or each African country stated separately) and ‘CD4 count’ or ‘viral load’. Both MeSH and text terms were used and limits set for ‘humans’, ‘adults’ and ‘English language’ (no translation facilities were available to allow inclusion of other languages). Each search strategy was saved and printed as evidence of the process undertaken. The references of any relevant papers were also searched to identify any further literature. The inclusion and exclusion criteria are shown in Table 1. The outcome measures used were CD4 count (cells/mm3) and viral load (copies/mL or percentage undetectable viral load [UDVL]). These were considered to be more objective outcome measures when compared with other alternatives (adherence, mortality rates, opportunistic infections) that involve subjective interpretation by a clinician or technician.
Inclusion and exclusion criteria

ART = antiretroviral therapy; UDVL = undetectable viral load
In >50% of sample size
Initially only papers of Grade 1 and 2 evidences were to be included, but this had to be extended to all grades of studies due to the paucity of high-quality study designs
All studies considered relevant after reviewing the title and abstract (when available) were accessed and evaluated. The researcher selected the papers using the inclusion/exclusion criteria illustrated in Table 1. The reason for exclusion was documented and later discussed with a clinical expert in the field to minimize selection bias.
A data extraction table was adapted for the study. 1 The data extracted were: publication details, demographics (country, setting, mean age, percentage female), sample size, percentage ART naïve, details of ART regimen, details on study design and ethics approval, data on CD4 count and viral load at baseline and at subsequent time-points after ART initiation. The weight of evidence associated with each study design was based on the hierarchy of evidence and not by assessment of the quality of each individual study. All data were extracted by Dr Hammond and repeated a second time-point to ensure accuracy of the initial extraction.
Statistical analysis
Statistical analysis was performed with ‘StatsDirect’ version 2.5.7 (StatsDirect Ltd, UK). In the analysis data provided for the CD4 count were assumed to be the mean even if described in the text as the median. UDVL was defined as <400 copies/mL because this parameter was used in the majority of papers. Four papers defined UDVL differently (<200 6 , <300 10 and <500 copies/mL).11,12 The data were UDVL was defined as <400 copies/mL was included in the analysis.
Sample size was calculated from the number of tests conducted at each time-point. If this data were not available, it was assumed that everyone was tested in the sample and this figure was used for the calculation. Baseline data and six subsequent time-points were used for analysis. Data were rounded to the nearest time-point used in the study. This was to ensure that the influence of the data was not exaggerated.
Results
The search, as illustrated in Figure 1, identified 368 papers. Of those, 320 papers were excluded by the title and abstract for reasons as follows: the topic not relevant (n = 309), the data not appropriate (n = 6), the setting not Africa (n = 3) or the data included HIV-2-positive people (n = 2). Forty-eight papers were obtained and a data extraction sheet was completed for each of these studies. During this process, a further 19 studies were excluded. Reasons for exclusion were data not appropriate (n = 7), ART not initiated (n = 3), unable to separate African data from other cohorts (n = 3), repeat of cohort data (n = 2), HIV-2 data included (n = 1), topic not relevant (n = 1), setting not Africa (n = 1) and paper not in English (n = 1). Twenty-nine papers were identified which met the criteria to be included in the meta-analysis.
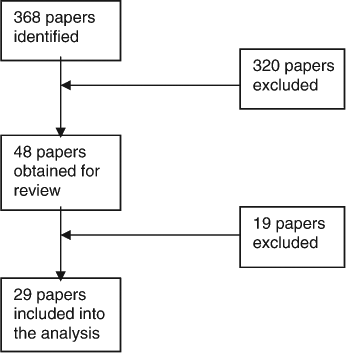
Flow chart of results of literature search
The papers analysed were from 12 different countries in Africa. Four countries had studies excluded because of the limited data published within the paper. No papers were found for 32 African countries. A variety of reasons may account for including this: the lower HIV prevalence in northern Africa; increased prevalence of HIV-2 in western Africa; a proportion of African countries’ first language is not English and data may be published in another language and therefore excluded from the study.
The papers included in the meta-analysis were either cohort studies or observational studies and were therefore Graded III or IV on the hierarchy of evidence. 1
The demographic and baseline data of the 29 studies is summarized in Table 2. The sample size ranged from 25 to 16,198 and the mean age was between 31 and 41 years. More than 50% of the population were women in 24 of the studies, which reflects the African epidemiological data where more women than men were found to be infected with HIV. 4
Demographic characteristics and baseline data of the studies
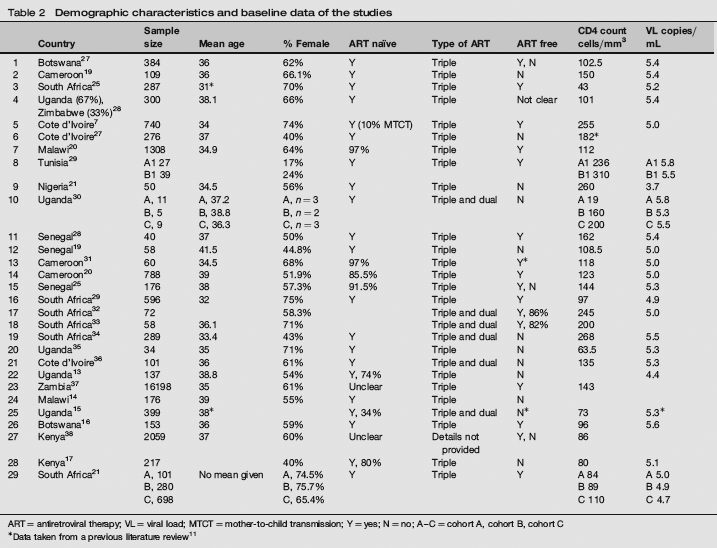
ART = antiretroviral therapy; VL = viral load; MTCT = mother-to-child transmission; Y = yes; N = no; A–C = cohort A, cohort B, cohort C
Data taken from a previous literature review 11
In two papers14,18 paediatric data were included with the adult population as it was not possible to separate this data. These studies were included because the population was predominantly adult. One paper 7 had 3% of participants who were dual-infected with HIV-1 and HIV-2. In 15 papers, all participants were ART naïve; in nine papers, 74% or more participants were ART naïve; one paper had only 34% 18 ART naïve and the ART status was not clear in four papers (Table 2). In six papers,13–18 the drug regimens included both dual and triple therapies and the outcome measure data analysed were the combined results of both dual and triple therapies. This decision was made because the demographic data reflected the entire population and not the subset of triple therapy. One paper did not specify the regimen used. A recent change in prescribing habits was evident from using dual therapy to the routine administration of triple therapy.
CD4 count outcome data were extracted from 27 papers for baseline data and 19 papers for subsequent time-points. Viral load at baseline was extracted from 23 papers and percentage UDVL was extracted from 19 papers. At baseline, the mean CD4 count was 141.0 cells/mm3. The WHO guidelines 3 stipulate the commencement of ART at a CD4 count of <200 cells/mm3 irrespective of the clinical stage and ART was considered for all patients with a CD4 count between 200 and 350 cells/mm3. The baseline CD4 count indicates the advanced nature of HIV in the subjects who took part in these studies. At baseline, the mean viral load was 5.2 log10, where 2.6 log10 is UDVL (defined as <400 copies/mL) again demonstrating the degree of immunosuppression of the subject prior to receiving ART.
The pooled data demonstrated a steady increase in CD4 count at all time-points except at 18 months (Figure 2). This time-point had only a small sample size and a large confidence interval (CI), which means that this result is less reliable. UDVL remained above 64% at all time-points reaching the highest measure of 74.7% at six months (Figure 3). The papers with data included at a particular time-point ranged from two to 28 papers for CD4 count and four to 23 papers for percentage UDVL. There were more studies with data included at six and 12 months. The sample size decreased from baseline. No paper provided data beyond three years following ART initiation.
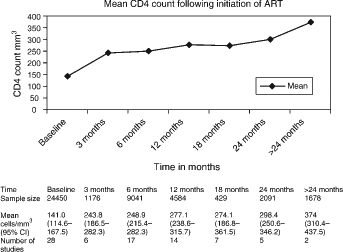
Mean CD4 counts at baseline and specified time-points
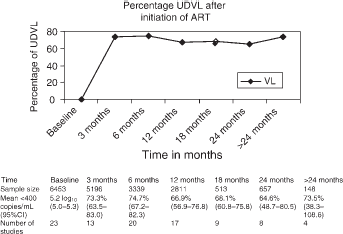
Mean percentage undetectable viral load (UDVL) at specified time-points
The CIs of the CD4 count widened from baseline. The baseline data and data collated at six and 12 months included the largest sample size along with the higher numbers of papers and narrower CIs.
Discussion
The data in this meta-analysis demonstrated positive effects on both the immunological and virological outcome measures used in this study. This is evidenced by an increasing CD4 count observed from three months until after 24 months after initiation of ART. During the same time frame, the majority of people treated with ART maintained their UDVL (<400 copies/mL).
This analysis presents supporting evidence that ART can be provided successfully within the continent of Africa even with the various limitations attributable to a resource-poor setting. Using laboratory data to evaluate the efficacy of ART, reduced interpreter bias as these measures provide a more objective measurement than using other clinical measures (for example clinical improvement or mortality rates). However, a variety of machines with different sensitivities were used to measure the CD4 count and viral load, which could influence the compatibility of the data.
Unfortunately, the weight of the evidence associated with the study design is weak, with all studies being categorized as either Grade III or IV on the hierarchy of evidence. This will have an impact on both the reliability and generalizability of these results. The interpretation of this data is further effected by the different limitations of the studies included in the meta-analysis, through the confounding factors introduced by the programme design and the setting, the bias introduced by the study design and application, as well as the limitations of this review itself.
None of the studies were either randomized or did they have any control group. Three of them were cohort studies19–21 comparing different ART regimens, and the others were observational studies, either prospective or retrospective (with one-third of the papers not providing a clear explanation of the study design). The strength of evidence associated with these study designs is less than the aforementioned randomized controlled trials (RCT) or an unrandomized controlled trial. 22 The study would be improved through the assessment of the quality of each individual study. Weighing the evidence in this way, rather than only upon the study design without considering the quality, has not allowed adjustment of any error in the implementation of an individual study.
Each programme researched in these papers provided insight into the complexity of scaling-up ART in developing countries and the logistical challenge that is incurred. Many of the programmes established to distribute ART were unique and implemented in isolation, making it difficult to compare the studies or to draw conclusions from the extracted data, which can be generalized to future programmes.
These differences introduced confounding factors into the individual studies and into this analysis. Some confounding factors influenced many of the studies, while others impacted on only one or two of them. For example, the measures established to improve adherence within a programme had potential to influence the number of participants retained and therefore the number receiving follow-up CD4 count and viral load tests.
To improve the longterm outcome of people living with HIV, programmes administering ART often provided other services, which could confound the data. Treatment was frequently provided for opportunistic infections, which in turn impacted on the choice of ART as well as having the potential to cause interactions or conversely improvement in the individual's overall health. Other programmes offered nutritional support, an important factor in Africa, where nutritional needs are often not adequately met but a factor, which could impact on the outcome of HIV. Another difference was the use of brand formulations of ART in a proportion of trials, generic ART in others, whereas no mention of the manufacturer of ART in others.
The cost of ART and the laboratory tests were noted to influence adherence in studies where the participants had to pay for the ART. 13 The authors also suggested that financial constraints influence doctor's choice of drugs and in those paying there was a greater chance of using dual therapy over triple therapy. Two papers were excluded because only clinical outcomes were measured, of which one of the papers cited financial constraints as the reason for non-availability of laboratory data. 23
The settings of the studies were also different ranging from rural locations to urban; privately funded clinics to nongovernmental organizations or governmental institutions. The logistics of each programme therefore brings with it a different set of challenges and influences on the interpretation of the results. For example, a rural location may have more difficulty in maintaining a reliable drug supply, but an urban location may have more difficulty in retaining the population because of the transitory nature of urban living.
Early ‘pioneer cohorts’ included within this analysis had limited ART regimens and no official guidance from organizations such as the WHO. 7 The data in these studies were often accumulated with the aim of comparing efficacies of dual over triple therapy. There is no longer an emphasis in this direction as evidence supports the use of triple therapy as superior to dual therapy 24 and therefore the dual regimens may confound the result of this analysis.
The duration of the studies were often short-term, extending from only three months follow-up to a maximum of three years, with most studies ending between six and 12 months. This meta-analysis does not enable conclusions to be drawn for the longterm use of ART. CIs were noted to widen as the duration of time from the initiation of ART increased, indicating a need for greater caution in drawing conclusions for these later figures (Figures 2 and 3). This makes it essential for data to be collated on the longterm outcome of ART including its ongoing efficacy, virological failure rates, development of drug resistance, adherence levels, use and availability of second-line regimens. Studies in developed countries have shown escalating problems in management with increasing duration of therapy (for example increased toxicity, decreased adherence, drug resistance and treatment switches). 25
The efficacy of ART measured by CD4 count and viral load outcome measures is influenced by a multitude of individual variables, which were not accounted for within this review. For example, their socioeconomic status, family contacts and support, access to other health services and educational attainment. This alongside the disease profile of the area (for example frequency of TB, prevalence of HIV-1 and HIV-2 status) will all have an impact on the data collated from each study but cannot be specifically accounted for.
Alongside the limitations of the individual studies included within the meta-analysis, account of the limitations to this particular review needs to be made. The search only attempted to uncover published material on the subject but not unpublished data including conference papers and ‘black literature’. This introduces publication bias into the study because papers are more likely to be published where there is a statistically significant outcome (in this study a change in CD4 count and/or viral load). 18 Only a small number of databases were used and therefore all available papers may not have been identified.
As explained earlier, many of these programmes involved a comprehensive and complex system of adherence measures, counselling, medical follow up and lifestyle advice requiring the involvement of many health professionals. The outcome of such programmes may be excellent in terms of CD4 count and percentage UDVL, but the replication of such programmes may not be realistic within the resource constraints of many African countries. Design and evaluation of simple programmes involving minimal laboratory measures and simplified drug regimens are required for scale-up to reach all the people who potentially require ART. Such a programme will require a difficult and intricate balance to be made in the structure of its design. Advice for such programmes has been established by the WHO 26 but supportive evidence appears to be limited. Research would be valuable in evaluating the outcomes of small programmes against those of larger programmes, and simplified against complex programmes to help define an evidence-based approach.
This study has not compared the data from each of the different drug regimens used within these papers. Further analysis would be important to establish if there is a particular ART regimen, which has greater efficacy within the continent of Africa, both in terms of the complexity of the regimen itself as well as any particular genetic susceptibility to the toxicity of the drugs. The number and quality of the available studies would not be suitable at the present time for such an analysis.
This study would be enhanced if the researcher had extracted the data on both primary and secondary virological failures and the need for second-line regimens. This data would have been useful to provide insight into those patients who did not have an UDVL, giving some understanding of treatment failure within the African continent. Contacting authors for missing data would also have improved this study.
Conclusion
The meta-analysis indicates that ART can be effective in the continent of Africa, which is evidenced by the increasing CD4 count levels noted over the three-year time period of the study; and the high percentage of subjects with UDVL at each time-point of the study. This study has highlighted the many confounding factors and biases introduced into the studies included in the analysis both from the individual papers and from this review. The low grade of evidence attributed to the study designs reduces the confidence that can be placed in the conclusions drawn. This study emphasizes the growing urgency to implement robust, RCT in a variety of different settings. With the escalating epidemic and the international effort to provide universal access to ART, there is never a greater need for a strong evidence base to identify and support effective HAART regimens for the millions who urgently require this treatment, as well as ensuring the appropriate allocation of the limited resources available.
Footnotes
Acknowledgements
Dr R Hammond designed and researched the papers. Dr T C Harry supervised, edited and performed statistical analyses.