
Abstract
Summary
We present a 40-year-old woman who presented to the genitourinary medicine department with a two-year history of recurrent non-painful vulval lumps. She was in a stable relation with one male sexual partner over the preceding 20 years and her sexual health screen was negative. Clinical examination of these lumps was suggestive of anogenital warts for which she has been treated on numerous occasions over the last two-year-period with liquid nitrogen cryotherapy and podophyllotoxin 0.15% cream. As the lumps were not responding to conventional wart treatment, a biopsy from these lesions was performed. The histological appearance showed focal fibrin thrombus formation within dilated vascular channels consistent of a subepidermal cavernous haemangioma.
This case demonstrates that the clinical diagnosis of anogenital warts is not always straightforward. It highlights the importance of obtaining a tissue diagnosis from the resistant or atypically looking warty lesions to avoid making the wrong diagnosis.
Introduction
Benign tumours and tumour-like conditions that occur in the vulva include haemangioma, lipoma, angiokeratoma, lymphangioma, neurofibroma, rhabdomyoma and schwannoma. 1 Cavernous haemangioma is rare on the vulva. To our knowledge, this is the first case that reports a subepidermal cavernous haemangioma of the vulva that mimics clinically anogenital warts. A vulval biopsy in this case was invaluable to obtain the correct diagnosis.
Case Report
In 2005, a 40-year-old woman attended the genitourinary medicine (GUM) clinic complaining of recent lumps on the vulval area. These lumps were not painful or itchy and appeared on the mons pubis and both labia majora. Past medical history included cervical spondylosis, right torticollis, capsulitis of the right shoulder and one seizure following a head injury. She was also allergic to nickel. She had one male sexual partner in the preceding 20 years and her sexual health screen was negative. However, the examination of the lumps was suggestive of anogenital warts. These were treated with liquid nitrogen cryotherapy, and home treatment with podophyllotoxin cream 0.15% was recommended. Over the following two years, the patient received treatment at the GU medicine clinic on numerous occasions for recurrent vulval warts. However, these lesions were not subsiding and the patient returned to clinic with a history of infected vulval lumps. Swabs from these lumps were negative for viral herpes simplex and bacterial infection. A full sexual health screen performed at the GU medicine clinic was also negative. Genital examination showed smooth-walled, dome-shaped papular rash at the mons pubis. The left labia majora appeared hypertrophic with warty-looking lesions (Figure 1). Punch biopsies from the papular rash at the mons pubis and the warty-looking lesions at the labia majora were carried out. The histological picture from both sites was identical and showed focal fibrin thrombus formation within dilated vascular channels consistent of a subepidermal cavernous haemangioma (Figure 2). The patient was referred to the dermatologist for further management.

Vulval lumps with warty-looking appearance
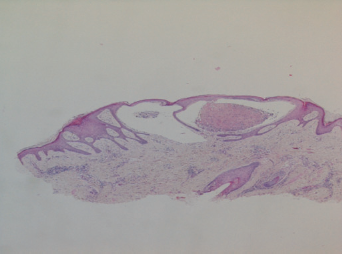
Fibrin thrombus within dilated vascular channels in subepidermal cavernous haemangioma. Haematoxylin and eosin stain, ×4 objective magnification
Discussion
Cavernous haemangioma is rare on the vulva. This benign vascular lesion may be relatively large, complex and deep in comparison with capillary haemangioma. 2 It consists of slowly flowing haemodynamically inactive vascular malformations, which are present at birth and slowly, but progressively worsen throughout the lifetime of the patient. 3 Vulval cavernous haemangioma usually affects the labia majora, but may rarely be localized to the clitoris. 4 Distortion of the vulva may be present and clitoral involvement may resemble clitoral hypertrophy. 2 Other benign tumours and tumour-like conditions that occur in the vulva include lipoma, angiokeratoma, lymphangioma, neurofibroma, rhabdomyoma and schwannoma. The histological features are similar to their appearance in more common sites. 1
Cavernous haemangioma may ulcerate and bleed, and on rare occasion may require therapy. 2 If treatment is necessary, corticosteroids are the mainstay of therapy, which may be used topically, intralesionally or systemically. Interferon-α, vincristine, cyclophosphamide and laser therapy are therapeutic options for complicated haemangiomas that do not respond to corticosteroids. 5
Although it can be present in isolation, subepidermal cavernous haemangioma may form part of two distinct syndromes, the ‘blue rubber bleb’ nevus syndrome and Maffucci's syndrome. In the former, it is associated with haemangiomas of the gastrointestinal tract and possibly iron deficiency anaemia due to gastrointestinal haemorrhage. 6 Hyperhidrosis in the region of the tumours may be associated. 7 In Maffucci's syndrome, the skin lesions are associated with multiple enchondromas of bone, particularly of the long bones resulting into variable shortening and deformity of the extremities. 8 Our patient had no features of either syndrome, except that the history of infected lumps may represent infection of the dermal sweat glands, which can be intimately related to the vessels forming the cavernous lesions. 7 The hypertrophic areas caused by the cavernous lesions as in this case, seem to give the affected areas of the vulva this papular or more confluent lumpy appearance that mimic anogenital warts.
To our knowledge, this is the first case that reports a subepidermal cavernous haemangioma of the vulva that mimics clinically the appearance of anogenital warts. This case demonstrates that the clinical diagnosis of anogenital warts is not always straightforward. It highlights the importance of obtaining a tissue diagnosis from the difficult to treat or a typical looking warty lesions to avoid getting it wrong again!