
Abstract
Summary
A retrospective electronic database study was conducted to determine any differences in time to virological failure and percent of virological failure among HIV-infected patients concurrently receiving H2-blockers versus patients not receiving these agents while receiving atazanavir (ATV)/ritonavir (r) or lopinavir (LPV)/r-containing antiretroviral treatment regimens. Data were culled from October 2003 (when ATV became commercially available) through February 2006. Virological failure was defined as (1) two plasma HIV-1 RNA levels >400 copies/mL after at least one HIV-1 RNA level below the level of detection or (2) failure to achieve an HIV-1 RNA <400 copies/mL within 24 weeks. Data from 267 ATV/r-treated patients who met the case definition were compared with data from 670 LPV/r-treated patients. Approximately 10% of the ATV/r group received concurrent H2-blockers when compared with 20% of the LPV/r group. Multivariate analysis showed no statistically significant differences regarding time to virological failure between or among the four subgroups, adjusting for differences in baseline characteristics (P = 0.79, log-rank test). At 750 days following treatment initiation, the proportion of patients not experiencing virological failure was 56% in the ATV/r-blocker subgroup, 48% in the ATV/r-alone subgroup, 45% in the LPV/r-alone subgroup and 42% in the LPV/r-blocker subgroup.
Introduction
The therapeutic benefits of protease inhibitor (PI)-containing combination antiretroviral regimens are often accompanied by adverse events, with one-eighth of patients stopping or seeking a switch in therapy due to gastrointestinal (GI) side-effects. 1 In a prospective survey involving 200 patients 18-70 years old receiving highly active antiretroviral therapy (HAART) (110 receiving PIS), 62% reported episodes of heartburn, 30% reported gastroesophageal reflux disease and 13% reported ulcers after starting HAART therapy. 2 To relieve GI symptoms, 51% of those surveyed treated themselves with over-the-counter H2-receptor blockers or proton pump inhibitors.
Acid-reducing agents, such as H2-receptor blockers, have been documented in pharmacokinetic studies to significantly reduce atazanavir (ATV) plasma concentrations and exposure following simultaneous co-administration.3,4 In view of this, the ATV label contains a recommendation to maintain a 10-hour interval between H2-blocker and ATV dosing to allow gastric acid normalization prior to ingesting ATV. 5 To date, no study has compared ATV with other PIS regarding time to virological failure in a large population of HIV-infected patients concomitantly receiving or not receiving H2-receptor blockers.
Materials and Methods
A retrospective database study was conducted at the Parkland Health and Hospital System HIV Database (Dallas, TX, USA), which contains the medical records of more than 10,000 HIV-infected patients, to evaluate any differences in time to virological failure and percent of virological failure among patients concurrently receiving H2-blockers (cimetidine, ranitidine, famotidine or nizatidine) versus patients not receiving these agents while being treated with ATV/ritonavir (r) or lopinavir (LPV)/ r-containing antiretroviral treatment (ART) regimens.
Data were culled from October 2003 (when ATV became commercially available) through February 2006. Virological failure was defined as (1) two plasma HIV-1 RNA levels >400 copies/mL after at least one HIV-1 RNA level below the level of detection or (2) failure to achieve an HIV-1 RNA <400 copies/mL within 24 weeks. Data elements abstracted from patient records included demographics, viral load (VL), CD4+ cell counts, HIV disease and treatment history, hepatitis B/C status, HIV-related and non-HIV-related conditions and their drug treatment, inpatient and outpatient resource utilization and prescription refill history.
Results
Data from 267 ATV/r-treated patients who met the case definition were compared with data from 670 LPV/r-treated patients (Table 1). Approximately 10% of the ATV/r group received concurrent H2-blockers when compared with 20% of the LPV/r group. Most of the 937 patients (85%) evaluated were male. The patient population was racially/ethnically diverse, with over half of the patients being either Black or Hispanic. In the ATV/r-alone, LPV/r-alone and LPV/r-blocker subgroups, 78-82% of patients were treatment-experienced, whereas this proportion was smaller (57%) in the ATV/r-blocker subgroup. For the total population from whom data were accessed, baseline median VL was ≥5.13 log10 copies/mL and CD4+ cell count was ≥ 208 cells/mm3.
Demographics and baseline disease characteristics
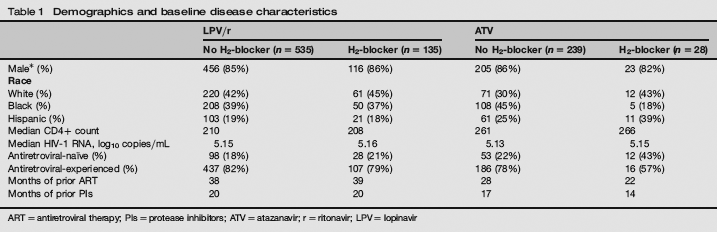
ART= antiretroviral therapy; Pls= protease inhibitors; ATV = atazanavir; r= ritonavir; LPV= lopinavir
No statistically significant differences (P < 0.05) were observed between or among the ATV/r-alone, ATV/r-blocker, LPV/r-alone or LPV/r-blocker groups with regard to gender, baseline CD4+ cell count or months of prior ART.
Multivariate analysis showed no statistically significant differences regarding time to virological failure between or among the four subgroups, adjusting for differences in baseline characteristics (P = 0.79, log-rank test) (Figure 1). At 750 days following treatment initiation, the proportion of patients not experiencing virological failure was 56% in the ATV/r-blocker subgroup, 48% in the ATV/r-alone subgroup, 45% in the LPV/r-alone subgroup and 42% in the LPV/r-blocker subgroup.
Time to virological failure. P= 0.79; log-rank test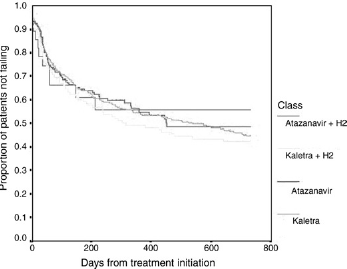
Discussion
The slightly higher proportion of patients who did not fail in the ATV/r-H2-blocker subgroup when compared with the ATV/ r-alone subgroup (56% vs. 48%) possibly could have been related to the H2-blocker-treated patients having better GI tolerability or adherence. However, patient adherence cannot be verified by our use of only prescription refill records. The virological failure rates in our largely treatment-experienced population were consistent with the failure rates reported in this type of study population, who had received ATV/r-containing regimens for at least 48 weeks in AI424-045 4 and LPV/r-containing regimens for up to 144 weeks in Study 765. 6
These results suggest an absence of a difference in clinical efficacy between H2-blocker recipients and non-recipients. These findings should be interpreted with caution for several reasons. The study was retrospective and the impact of several possible confounding factors (concurrent use of other CYP 3A4 inhibitors or inducers, different nucleoside reverse transcriptase inhibitor backbones, concurrently administered non-nucleoside reverse transcriptase inhibitor) on the results of the study cannot be ruled out. This was not a randomized trial and patients who were treated with LPV/r were more likely to have received a H2-blocker since labelling for LPV/r does not contain any recommendation to space LPV/r and H2-blocker dosing. 6 Thus, there was a significant potential for selection bias in this study. Finally, the size of the ATV/r and LPV/r arms was quite different, with 2.5-fold more patients receiving LPV/r-containing regimens.
Conclusion
Data from this HIV observational database study suggested no significant difference between ATV/r and LPV/r treatment arms whether or not patients received concurrent H2-receptor blocker therapy.