
Abstract
The aim of this study was to detect the sensitivity and specificity of rapid syphilis diagnostic tests (immunochromatographic strip [ICS] test and rapid test device [RTD]) performed by low-skilled paramedics in field clinics and by highly-skilled technologists in laboratories and compare them with the gold standard (rapid plasma reagin [RPR] and Treponema pallidum haemagglutination [TPHA]) tests for diagnosis of syphilis. A cross-sectional study was conducted among female sex workers (FSWs) in Dhaka, Bangladesh, from August 2004 to July 2005. Blood specimens were tested for syphilis using (i) ICS, (ii) RTD, (iii) RPR tests performed by low-skilled paramedics; and (i) ICS, (ii) RTD, (iii) RPR and (iv) TPHA tests by highly-skilled technologists. The sensitivity and specificity of the ICS and RTD test performed by low- and highly-skilled personnel were compared with the gold standard. A total of 684 FSWs were enrolled and the prevalence of syphilis among FSWs was 20.8% as determined by the gold standard. There was no significant difference in the performance of ICS test done by paramedics in the field when compared with the gold standard performed by highly-skilled technologists in the laboratory (sensitivity, 94.45%; specificity, 92.6%). The ICS test could fulfil the need for a non-invasive, rapid screening test for syphilis.
Introduction
Syphilis is one of the most common sexually transmitted infections (STI) in developing countries. Although the prevalence of syphilis has declined during the last two decades in Europe and North America, recent data indicate a rising incidence of syphilis worldwide, including Europe and North America. The World Health Organization (WHO) global estimates show that there were approximately 12 million new cases of syphilis in 1999 of which one-third were in south and south-east Asian countries 1 including Bangladesh.
Public health consequences of untreated syphilis are greater for females than males because it can be vertically transmitted to the fetus during pregnancy. Infectious syphilis in pregnancy commonly results in spontaneous abortion, stillbirth, intrauterine growth restriction, prematurity and congenital syphilis of the newborn. 2 Congenital syphilis has a wide array of serious manifestations including meningitis and meningovascular syphilis in newborn infants. In 30–60% of cases, vertical transmission of syphilis occurs from mother to fetus. However, the risk of transmission diminishes as maternal syphilis advances. 3 Vertical transmission of syphilis is preventable if detected and treated in the first or early second trimester of pregnancy; however, to prevent fetal wastage and congenital anomalies, treatment must be provided early in pregnancy.4,5
In Bangladesh, the prevalence of syphilis in groups vulnerable to HIV infection is 18–43%.6,7 Several studies conducted in women from the general population and from rural and urban Bangladesh showed that the prevalence of syphilis ranged between 1% and 6%.8–12 Recent studies reported that prevalence of syphilis in pregnant women attending urban primary healthcare (PHC) clinics for antenatal check up (ANC) was 1.5–3.0%.13,14
Identification and treatment of syphilis among pregnant women to prevent complications and vertical transmission to fetus is a challenge. Most pregnant women with syphilis neglect to seek medical care because the primary lesions are often painless and unseen, as they are located inside the vagina or cervix. Secondary syphilis is also often characterized by nonspecific signs and symptoms. Serological tests for screening and subsequent confirmation can assure detection of syphilis. Screening and treating syphilis has been shown to be inexpensive and cost-effective. 15 It has been documented that syphilis screening in pregnant women is cost-effective even if the prevalence is lower than one per 1000. 16
The WHO guidelines for the serological diagnosis of syphilis recommends the use of rapid plasma reagin (RPR) or venereal disease research laboratory and Treponema pallidum haemagglutination assay (TPHA) for screening and confirmation of diagnosis, respectively. 17 All three processes require collection of blood through venous puncture, specimen transport to laboratory, serum separation, appropriate equipment and trained human resources for diagnosis and interpretation of results. This usually takes several hours from specimen collection to test result. The scarcity of laboratories and trained man power in PHC settings, cost associated with testing, and delay in the delivery of results are a few of the major obstacles in the implementation of universal screening of syphilis in developing countries. The result is untreated syphilis or delayed treatment. The ability to obtain on-site rapid syphilis test results using locally available staff and resources could greatly enhance public health efforts to treat syphilis.
Although several different manufacturers developed rapid tests using lateral-flow technology and recombinant antigens in the late-1990s, there are few published evaluations of these tests. 18 Most of these evaluations are laboratory-based, using serum specimens and performed by highly-trained technologists, which is not applicable for developing country settings where trained manpower rarely exists. Immunochromatographic strip test (ICS) and a rapid test device (RTD) to identify serum antibodies to a recombinant T. pallidum-specific antigen are two recently developed and commercially available rapid diagnostic tests for syphilis produced by ACON Laboratories, Inc, USA. These tests might be good candidates for use in PHC settings in developed countries because they have minimum steps, can be used on whole blood, require no specialized equipment and only minimal technical training. The kits can be stored at room temperature and performed in 10–15 min. The ICS and RTD tests are commercially available and costs range from US$ 0.31 to 0.41/test. However, neither of these tests has been evaluated in the PHC settings in developing countries.
We have evaluated these two rapid tests (ICS and RTD) in a PHC setting and in the laboratory using whole blood. The performance of the tests done by low-skilled paramedics in clinics and highly-skilled technologists in the laboratory was compared with the gold standard (both RPR and TPHA).
Materials and Methods
The study was cross-sectional in nature and conducted among FSWs attending a PHC clinic of International Centre for Diarrhoea Disease Research, Bangladesh (ICDDR,B) in Mirpur, Dhaka, Bangladesh. All FSWs between 18 and 45 years of age attending the clinic were eligible for enrolment in the study irrespective of RTI/STI symptoms. All eligible women were requested to participate in the study after receiving a brief description of the study purpose and procedures. Informed written consent was obtained from all participants. Participants were interviewed by a female social worker obtain sociodemographic and behavioural information including sexual and medical history. A physician interviewed the FSWs about symptoms suggestive of present or past syphilis (ulcer in genital region) and performed a gynaecological examination including a speculum examination. From all enrolled subjects 10 cm3 of venous blood was collected. All enrolled women were asked to contact the clinic after 72 hours to collect the test result and those who were positive for syphilis were treated according to the national STI management guidelines. 19 The study was approved by ICDDR,B's ethical review board.

Flow chart of sample collection and testing. *TPHA-Treponema pallidum haemagglutination assay
The blood specimen was divided into two portions. The first portion was further divided into three aliquots and given to three paramedics in the clinic for performing the ICS and the RTD using whole blood, and the RPR tests using serum. The second portion was sent to the reference laboratory at ICDDR,B in a tube containing anticoagulant and was further divided into four aliquots which were used by four technologists in the laboratory to perform four diagnostic tests: the ICS and the RTD using whole blood and RPR, and TPHA test using serum (Figure 1). All rapid tests and RPR were done on the same day, and TPHA test was done in batches.
ICS and RTD were carried out with whole blood as recommended by manufacturers. Briefly, an ICS and RTD were removed from the foil pouch and two drops (100 μL) of whole blood was transferred onto the specimen pad or test strip and device and one drop (50 μL) of buffer was added. The test results were read after 15 min. A positive reaction was characterized by the appearance of two pink lines on the cellulose strip or device, while a negative reaction was characterized by only one visible line. If no pink line was seen, the test was considered as invalid.
RPR (BioMerieux BV, USA) and TPHA (Fujirebio, Tokyo, Japan) tests were carried out as recommended by the manufacturer. A participant was considered to have syphilis if both RPR and TPHA results from the laboratory were positive (gold standard used for comparison). An active case was defined as a patient who had a positive TPHA test and an RPR titre ≥1:8.
Three low-skilled paramedics (completed three-year paramedic's diploma course) and four highly-skilled laboratory technologists (microbiologist with one year serology experience) were recruited for the study. All paramedics and laboratory technologists were trained on ICS, RTD, RPR and TPHA test procedures for one week before the study. The tests were performed simultaneously by paramedics in the clinic and technologists in the laboratory, and each was unaware of the test results of others. The tests performed by low-skilled paramedics in the clinic and highly-skilled technologists in the laboratory were randomly assigned (randomized for each day and for each person) to avoid an individual's bias towards a specific test. Each individual noted their result in a separate form and delivered the test results to study supervisor immediately after the test was done.
Behavioural and clinical data were collected on standardized questionnaires, entered and analysed by Statistical package for Social Science (SPSS, Chicago, IL, USA) version 12.0. Univariate analyses were performed for behavioural and clinical data and for calculation of syphilis prevalence using different tests. We used McNemar's χ2 test to compare the performance between low-skill paramedics and highly-skilled technologists for RPR, ICS and RTD.
Results
A total of 684 FSWs were enrolled in the study from August 2004 to July 2005. Sociodemographic characteristics of the participants are shown in Table 1. More than half of enrolled FSWs were between 18 and 25 years of age, had been married, did not have any education and had no history of genital ulcer.
Sociodemographic characteristics, obstetric and clinical history of female sex workers (n = 684) enrolled in the study
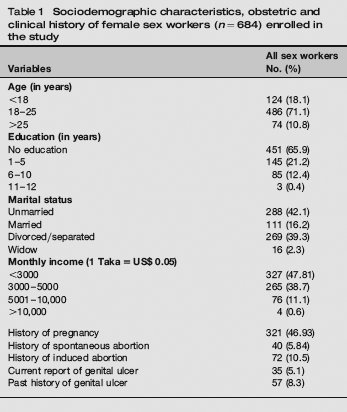
The prevalence of syphilis among enrolled FSWs was 20.8% as determined by gold standard (both RPR and TPHA-positive) and the prevalence of active syphilis was 6.4%. Among the FSWs, 35 (5.1%) were currently diagnosed and 57 (8.3%) already had a history of genital ulcer. There was no significant association between the present or past history of genital ulcer and syphilis infection. The prevalence of syphilis as determined by ICS and RTD performed by paramedics in the clinic and by technologists in the laboratory are shown in Table 2.
The prevalence of syphilis among female sex workers (n = 684) as determined by the gold standard and by ICS and RTD when performed by technologists in the laboratory and paramedics in the clinic
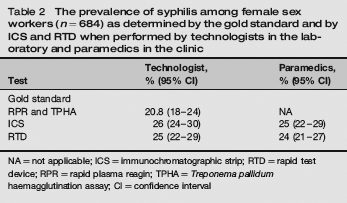
NA = not applicable; ICS = immunochromatographic strip; RTD = rapid test device; RPR = rapid plasma reagin; TPHA = Treponema pallidum haemagglutination assay; CI = confidence interval
Table 3 shows the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of the RPR, ICS and RTD for the technologists and paramedics when compared with gold standard. When performed by technologists, the sensitivity of all the three tests was similar ranging from 95.1% to 100%. The sensitivity of the RPR and RTD tests performed by paramedics in the clinic was significantly lower than the test performed by the technologists in the laboratory (P < 0.005 for RPR and P < 0.05 for RTD). There was no significant difference in the sensitivity of the ICS test performed by technologists in the laboratory and paramedics in the clinic when compared with gold standard (97.2% vs. 94.4%, P = 0.13, respectively).
The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of rapid plasma reagin (RPR), immunochromatographic strip and rapid test devices when performed by highly-skilled technologist and low-skilled paramedics when compared to both RPR- and Treponema pallidum haemagglutination-positive cases as a ‘gold standard’ (n = 684)
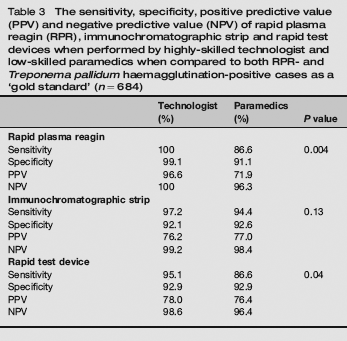
The sensitivity of ICS and RPR tests was further compared with test results indicating active syphilis infection (serum with RPR titre <1:8). The ICS test has a higher sensitivity than RPR (92.9% vs. 81.6%, data not shown) and was able to detect more active syphilis cases when performed by paramedics in the clinic.
Discussion
Despite recommendations from WHO for testing all pregnant women for syphilis as part of routine ANC, syphilis remains a major cause of avoidable perinatal death in developing countries including Bangladesh. Contributing factors include poor ANC practices, limited availability of syphilis testing facilities, costs associated with diagnostic testing, delays in the availability of test results. Difficulty in obtaining appropriate specimens and a lack of well-trained laboratory personnel may also contribute to the failure to make a timely diagnosis that would influence appropriate therapy.
The currently recommended RPR test for diagnosis of syphilis is available in many ANC clinic and health facilities in developing countries, including Bangladesh, and is done either by paramedics or nurses. Information on the performance of RPR tests as well as the treatment provided in such clinics is limited. We found that RPR tests appear to loose sensitivity when performed by paramedics in the clinic. This is consistent with earlier studies showing that the RPR ‘teardrop’ test, when performed in the field had 69.7% sensitivity and 96.5% specificity when compared with the standard RPR and TPHA tests. 20 The sensitivity of RPR further drops if the antibody titre is low, i.e. <1:8.21,22 The nonspecific nature of the cardiolipin antigens used in RPR contributes to the nonspecificity of the RPR test, as biological false-positives occur; these can be due to viral infections, malaria and pregnancy. 23 In addition, false-negatives may occur both in early primary cases 23 and in patients with secondary syphilis, as a result of prozone reactions. 24 Although RPR is inexpensive (about US$ 0.11/test), it requires equipment for storage (refrigerator), serum separation (centrifuge) and tests (pipette, rotator), which are not easily available in resource-poor settings. The test takes more than 40 min to complete; and requires certain skills to ensure the correct results and interpretations are reached. In addition, confirmatory tests such as TPHA are required because of the nonspecificity of the RPR test.
In our study, ICS appeared to perform better than RPR when performed by paramedics in clinics compared with gold standard. RPR is used as a screening test in the PHC clinics before a confirmatory test with TPHA. In a pilot study, a laboratory-based evaluation of the ICS test when compared with those of the standard RPR and FTA-ABS tests has been conducted and shown that the agreement between the ICS and FTA-ABS test results was 100%. The sensitivity, specificity, PPV and NPV of the ICS test were all 100%. The ICS test appears to be more sensitive than the RPR test. 25 Another study showed that the Abbott Determine TP rapid treponemal antibody test was easy, accurate and inexpensive which could facilitate rapid detection of syphilis in at-risk patients. 26
One limitation of the treponemal tests, such as the ICS and RTD used in this study, is that they can remain positive even after treatment27–29. Therefore, someone previously treated for syphilis may be misdiagnosed as having a new, untreated case of syphilis if only treponemal tests are used. In our study, we have seen that the sensitivity of ICS and RTD was 90.2% and 81.0% when compared with only TPHA-positive, but the sensitivity was 94.4% and 86.6% (performed by paramedics), respectively, when compared with RPR- and TPHA-positive as a gold standard. In our study, we have estimated that if the clinics were to rely on the paramedic performing RPR test (screening test for confirmatory TPHA), 13.4% of infected women would not be identified and 8.9% of non-infected women would be incorrectly treated as positive. In contrast, when the ICS test is used by paramedics only 5.6% of infected women would not be identified and 7.4% of non-infected women would be incorrectly treated as positive.
Our study suggests that the ICS could fulfil the need for an inexpensive, non-invasive, rapid screening test for syphilis. In this field evaluation, we have documented its consistent performance when compared with the serum RPR- and TPHA-positive cases. As a result of its accuracy, low cost and ease of use, it could be an effective rapid diagnostic test that can be easily carried out at the PHC level clinics by paramedics for the diagnosis of syphilis and can be used as routine antenatal screening for syphilis in the national ANC programme.
Footnotes
Acknowledgements
This study was conducted at the ICDDR,B with the support of cooperative agreement: 388-A-00-97-00032-00 from USAID. ICDDR,B acknowledges the commitment of USAID to the Centre's research efforts. We thank Dr Dipak K Mitra for statistical analysis.