
Abstract
Summary
The aims of the present study were to explore aspects of sexually transmissible infections (STI) prevention in general practice and to examine general practitioners' (GPs) perceived barriers to sexual-health promotion. The data from a postal survey of 409 GPs practising in New South Wales, Australia (response rate 45.4%) are analysed to explore the prevention of STI in general practice and to examine practitioners' perceived barriers to sexual-health promotion. About 49% of GPs reported having STI leaflets/pamphlets for patients in their clinic, while 21% had posters on STI displayed in their waiting room. Two-third (67%) of GPs provided STI-specific printed materials/leaflets to patients with STI. Female GPs were more likely to be proactive in STI prevention. Time and funding appear to be the major barriers to sexual-health promotion, followed by inadequate access to counselling. One-fifth (22%) of GPs felt that they had little influence in changing patients' risk behaviour, while about 28% emphasized the need for further preventive care training. The present study identifies inconsistencies in STI-prevention activities in general practice along with barriers to undertake sexual-health promotion. This area warrants further attention if GPs are to contribute fully to the control of STI.
INTRODUCTION
Sexually transmissible infections (STI) are endemic throughout the world and continue to be a challenge for public health. Surveillance data found that new diagnoses of chlamydia and gonorrhoea doubled in the United Kingdom over a period of five years (1997–2002), while diagnoses of syphilis increased eight-fold. 1 A recent study estimated that approximately 18.9 million people in the United States became infected with one or more STI in the year 2000. 2 In Australia, the population rate of reported diagnosis of chlamydia increased from 91.4 per 100,000 population in 2000 to 217.2 per 100,000 population in 2005. 3 These increases, which may partly be due to improved diagnostic tests, continue to pose a threat to individual wellbeing and public health as the infection, if untreated, can cause serious long-term consequences. 4
Available evidence suggests that health practitioners, as primary care providers, are not consistently involved with the promotion of sexual health for their patients. A Canadian study found that only about one-third of physicians reported routinely discussing high-risk sexual practices during consultations about contraceptives with adolescents. 5 This study showed that while 59% of general practitioners (GPs) discussed the benefits of consistent use of condoms, only 40% discussed the consequences of STI for women's health. Another study conducted among 541 primary care providers in Pennsylvania reported that about 43% of physicians believed that they were not responsible for STI prevention, while 70% believed that their counselling was ineffective. 6 A more recent qualitative study conducted with 22 GPs and 35 practice nurses in Sheffield, UK documented that preventive care provision for sexual-health issues was problematic in primary care because of their sensitivity, complexity and constraints of time and expertize. 7
In Australia, a number of studies have reported lack of adequate sexual-health promotion activities in primary care settings. 8,9 A recent study based on information from an ongoing research project involving GPs (the Bettering the Evaluation and Care of Health database) revealed that while the management of patients with symptoms of STI was common in general practice, health promotion activities were suboptimal. 10 For example, of the 448 women with the symptom of vaginal discharge, pathology tests were ordered for 92% of the patients, but only 21% were given advice, education and/or counselling. Similarly, a survey of 520 Victorian GPs found that only a quarter (26%) offered leaflets on STI to their patients, although 97% believed they would do so if they were provided with leaflets. 11
Given that many of the most common STI are asymptomatic, it is important to explore how GPs are involved with STI care, particularly in prevention and promotional activities and to examine whether such promotional activities were hindered by any factors that they perceived to be barriers. The aims of the present study were to explore some aspects of STI prevention in general practice and to examine GPs' perceptions about factors that facilitate or impede their involvement in sexual-health promotion.
METHODS
This study used data extracted from a cross-sectional postal survey on the management of STI by GPs practising in New South Wales (NSW), Australia in 2002. The study sample was drawn from a database of medical practitioners maintained by the Australian Medical Publishing Company (AMPCo). At the time of sample selection, there were 6800 GPs in NSW listed on the AMPCo database, and a 15% stratified random sample of GPs was drawn based on sex and area of practice. An additional 2% stratified random sample of GPs was used for a pilot study to field test draft questionnaires.
A nine-page self-administered STI questionnaire along with a covering letter, an information sheet and a self-addressed-reply-paid envelope was mailed to 1020 GPs across NSW in October 2002. Of the 900 eligible GPs, a total of 409 returned the completed questionnaire, giving a response rate of 45.4%. The survey explored various curative and preventive issues in STI care by GPs, while the present paper examines some issues relating to prevention of STI and sexual-health promotion. Results and discussion of issues associated with sexual-risk assessment through sexual history taking are presented elsewhere. 12
Measures
A number of outcome measures of interest were considered for the present analysis. The study participants were asked:
1. Do you have any of the following in your clinic? The response caterories included: (i) STI posters displayed in the waiting room; (ii) STI leaflets/pamphlets in the waiting room; (iii) leaflets about needle-syringe exchange; (iv) condoms for patients and (v) other, with response options being: yes and no.
2. What type of information do you give to STI patients? The response categories included: (i) brief verbal advice; (ii) give printed materials/leaflet; (iii) ask to read printed materials and make another appointment; (iv) where to get counselling support and (v) other, with response options being: yes and no.
3. In a patient with suspected or confirmed STI, do you usually provide information on: (i) mode of transmission; (ii) importance of partner treatment; (iii) preventive measures against future STI and (iv) Other, with response options being: yes – always, yes – as per request/need and no.
4. How would you prioritize your role in helping patients to understand issues in safe sex? The response options being: high, moderate and low priority.
5. What do you perceive as barriers to sexual-health promotion in general practice setting? The response categories included: (i) lack of time; (ii) lack of Medicare reimbursement; (iii) lack of privacy/confidentiality; (iv) lack of access to counselling; (v) lack of access to education resources; (vi) not the role of primary care provider; (vii) little influence on changing patient's lifestyle; (viii) further preventive care training could benefit the practice and (ix) other, with response options being: yes and no.
Statistical analysis
Logistic regression analysis was used to find possible correlates of aspects of STI prevention. Explanatory variables initially considered for the analysis were: GPs' age, sex, place of graduation, postgraduate training in medicine, postgraduate training in STI, duration of practice, type of employment (part-time vs. full-time), area of practice (metropolitan vs. rural), type of practice (solo vs. group), number of patients seen per week and diagnosis of an STI in the month preceding the survey. Because of considerable association between age and duration of practice, age was dropped from the analysis. Results are presented in the form of odds ratios (OR) and their 95% confidence intervals (CI). Goodness of fit for the fitted models was assessed using Hosmer–Lemeshow goodness of fit. The analysis was carried out using the statistical package SPSS Win V15.0 (SPSS Inc., Chicago, IL). 13
RESULTS
Study participants
Forty-three percent were women. Half (51%) were aged between 40 and 54 years, while nearly 25% were 55 years of age or over. About three-quarters (73%) graduated in Australia. Half (51%) reported having postgraduate training in medicine, while 20% had postgraduate training in STI. Nearly two-thirds (65%) practised in metropolitan areas and 22% worked in solo practices. About 20% reported practising medicine for up to 10 years, while 47% had been in practice for more than 20 years. Two-thirds (67%) worked more than 35 h per week (full-timers). The median number of hours worked by GPs was 43. The median number of patients seen by GPs was 120 per week, while the median number of STI cases diagnosed by GPs in the month prior to the survey was two.
Availability of STI materials at clinic
About half (49%) of GPs reported having STI leaflets/pamphlets for patients in their clinic waiting room, while leaflets on needle-syringe exchange were available to 15% of GP clinics. Posters on STI were displayed in the waiting room of 21% of GP clinics, and condoms for patients were available in 10% of GP clinics. Multivariate logistic regression analysis showed that having STI leaflets/pamphlets at clinic waiting room was positively associated with having postgraduate training in medicine, low patient load and a recent STI diagnosis experience (Model A, Table 1). For example, after adjusting for other factors, GPs who had postgraduate training in medicine had 1.6 times the odds of having STI pamphlets/leaflets in their clinics than their counterparts who did not have such training (OR = 1.60, 95% CI = 1.03–2.47).
Logistic regression estimates of factors associated with having STI leaflets/pamphlets in clinics and offering the STI printed materials/leaflets to patients in general practice
STI = sexually transmissible infections; aOR = adjusted odds ratio; CI = confidence intervals; Ref = reference category, NS = not significant at multivariate analysis; df = degrees of freedom
Significance level, *P < 0.10
Significance level, † P < 0.05
Significance level, ‡ P < 0.01
Significance level, § P < 0.001
Significance level, **P < 0.0001
††Mantel-Haenszel (trend) chi-square, P value
Approaches used to offer informationto STI patients
In response to the question on approaches used to provide STI patients with information on STI, 83% of the GPs reported giving brief verbal advice, 67% provided printed materials/pamphlets on STI and 55% advised their patients about where to get counselling. Just over one-third (37%) reported that they asked their patients to read the STI printed materials and to make another appointment. After adjusting for other factors, multivariate logistic regression analysis revealed that offering STI printed materials/pamphlets to patients was inversely associated with duration of practice, and positively associated with a recent STI diagnosis experience and practising in non-metropolitan area (Model B, Table 1). Furthermore, female GPs had 2.8 times higher odds of offering STI printed materials/pamphlets to their patients compared with their male counterparts (OR = 2.81, 95% CI = 1.68–4.70).
Information provided to patients with suspected or confirmed STI
In order to examine whether GPs usually provide information on certain aspects of STI care to patients with suspected or confirmed STI, the analysis showed that just over three-quarters (78%) of GPs always provided their patients with suspected or confirmed STI with information on: (i) mode of transmission of STI; (ii) preventive measures against future STI and (iii) importance of partner treatment. However, 14% provided information on preventive measures against STI when requested and/or needed. Logistic regression analysis showed that metropolitan GPs had nearly double the odds of always offering information to patients on mode of transmission of STI compared with their non-metropolitan counterparts (OR = 1.92, 95% CI = 1.11–3.30). It was also found that compared with local graduates, GPs who graduated overseas had 3.7 times higher odds of offering information on preventive measures against STI (OR = 3.71, 95% CI = 1.55–4.92) and importance of partner treatment (OR = 2.94, 95% CI = 1.29–6.71).
Priority in helping patients to understand safe sex
While asked about how GPs prioritize their role in helping patients to understand issues in safe sex, about 80% reported their high priority in such activities in STI care, while the remaining (20%) considered moderate to low priority. Multivariate logistic regression analysis showed that GPs who graduated overseas, compared with their local graduate counterparts, had double the odds of considering helping patients to understand safe sex to be a high priority in STI care (OR = 2.15, 95% CI = 1.06–4.35). Female GPs, compared with their male counterparts, had 2.4 times higher odds of considering high priority in helping patients to understand safe sex (OR = 2.42, 95% CI = 1.35–4.36).
Perceived barriers in sexual-health promotion
When asked about barriers, if any, in sexual-health promotion in general practice, the most commonly cited constraints were lack of time and lack of Medicare a reimbursement, respectively reported by 83% and 55% of GPs (Figure 1). Inadequate access to counselling and education resources was reported by over a quarter of GPs. About 28% of GPs emphasized that further preventive care training could benefit their practice of sexual-health promotion, while 22% felt that they had little influence in changing patients' risk behaviour (Figure 1).
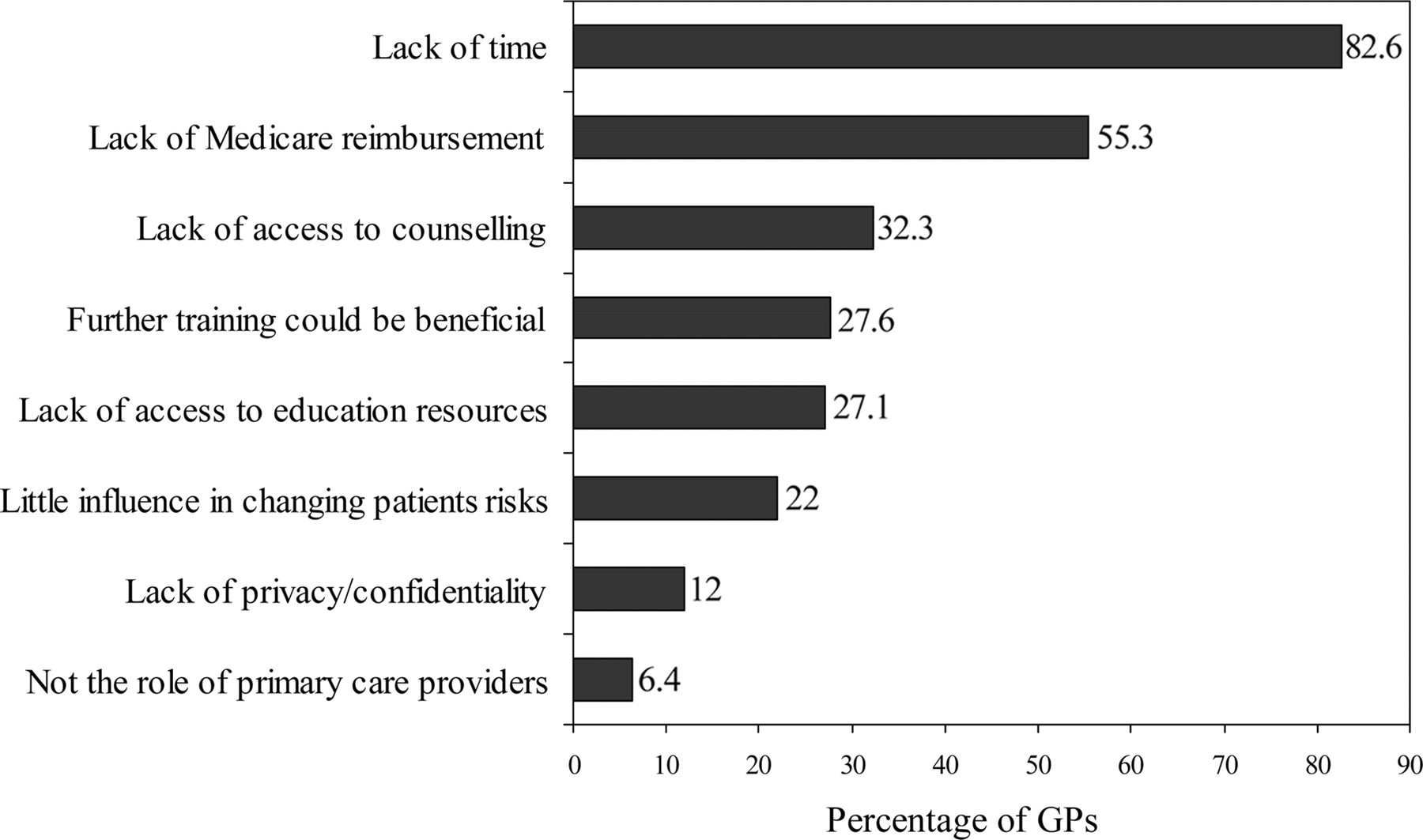
Perceived barriers to sexual-health promotion in general practice (some general practitioners [GP] provided more than one response)
DISCUSSION
As a first point of one-to-one contact with patients, GPs have the advantage of being able to offer preventive advice to patients on an opportunistic basis. 14 However, the present study revealed that practitioners were not fully capitalizing on the available opportunities for STI prevention in general practice. Although two-thirds of GPs would like to provide STI-specific printed materials/pamphlets to their patients, about half did not have any STI pamphlet/leaflet available in their clinics. While continued promotion and widespread availability of condoms are considered to be one of the key elements of any successful STI strategy 15 , the present study found that one in 10 GPs reported having condoms in their clinics for patients. The present study also revealed that female GPs were more proactive in STI-prevention activities, which has been reported elsewhere. 10,16,17 GPs practising in non-metropolitan areas were more likely to offer STI materials to patients, while metropolitan GPs were more proactive in providing patients with information on mode of transmission of STI. Earlier research showed that metropolitan GPs were more inclined to offer sexual-risk assessment in general practice. 12 However, further research is needed to explore how area of practice is associated (if any) with the care in general practice. While older GPs were found to be more comfortable in dealing with STI patients, 12 the present study found that GPs who were in practice for over 20 years were less likely to offer STI printed materials to their patients with STI. It was however, beyond the scope of the present study to investigate whether such reluctance was due to lack of access to printed materials or lacking motivation.
Appropriate health promotion materials in waiting rooms of surgeries are useful means of engaging the patients' attention and improving their awareness of prevention. 18 This strategy is particularly useful for those who feel embarrassed in discussing sexual matters with their care providers. 19 In the present study, one in five GPs reported having posters on STI displayed in their waiting room, while this percentage was even lower in the case of leaflets on needle-syringe exchange (a practice that is both legal and supported by Australian governments). This may be considered to be a missed opportunity as a poster indicating that the practising GP is comfortable in discussing sexual-health issues can act as a non-threatening prompt for patients to seek medical attention.
It is not surprising that most, though not all, GPs reported lack of time as a barrier to sexual-health promotion, which has also been reported elsewhere in other areas of health promotion. 20 As primary care providers, GPs have many demands on their time and can only consider prevention activities if there is time. However, it has been suggested that if patients are informed of the importance of prevention, they are more likely to return and have the issues addressed in follow-up visits. 19
Inadequate Medicare reimbursement is another major barrier to sexual-health promotion, as identified by the study participants. Health promotion requires longer consultations that are often less financially rewarding for a GP than are brief consultations. 14 The current Medicare Benefit Schedule primarily rewards episodic treatment rather than preventive care, which places considerable limitations on the extent and type of health promotion that can be undertaken in one clinical consultation. 8 Therefore, funding arrangements need to be reviewed to facilitate prevention activities in general practice.
Lack of access to counselling services was also identified as a barrier to sexual-health promotion in general practice. Counselling service has been less well integrated into Australian health services compared with other western countries; for instance, around one-half of GP surgeries have onsite counselling services in the UK. 21 The present study underscores the need to better inform GPs about the availability of national registers of accredited counselling practitioners as well as familiarize them with the benefits of specialized counselling services.
Although physician advice has been shown to change patients' risk behaviour 22 , one in five GPs in the present study felt that they had limited influence in changing patients' behaviour. This finding is of some concern because disease prevention is thought to be more effective when physicians perceive their efforts as useful. 23 Therefore, efforts should be made to help practising GPs to be more proactive in advocating strategies to modify patient risks. However, to be successful, GPs need to be fully convinced that such efforts would influence population health without being detrimental to their relationship with patients. 24
One in four GPs were in favour of further training in preventive care in order to offer proactive sexual-health promotion. This finding suggests that GPs may be under-equipped to deal with prevention of STI, but would like to contribute in prevention of STI. This cohort of GPs could benefit from in-service training to use brief but effective counselling strategies that may be administered over a series of visits. 20 The undergraduate curriculum, which is generally deficient in educating medical practitioners about sexual health 25 , needs to be revisited to include appropriate training in prevention and counselling related to STI.
In Australia, the Royal Australian College of General Practitioner (RACGP)'s Guide to Preventive Care in General Practice recommends which preventive activities are to be performed and how often they should be undertaken. 26 These guidelines, however, do not include any preventive measures for STI or even HIV/AIDS. It is important that STI-specific preventive measures be included in the RACGP's preventive care guidelines. The first National Sexually Transmissible Infections Strategy 2005–2008 provides the framework to deal with STI. 27 Also the NSW Sexual Health Promotion Guidelines are in place for the delivery of sexual-health promotion by health workers with a common goal of improving the sexual-health of the population. 28 However, a supportive environment needs to be created to follow these holistic and population focused guidelines to promote sexual health in general practice.
Certain limitations of the study must be acknowledged. The response rate for the present study was 45.5%, which can be considered a reasonably good one given that Australian GPs are difficult to reach for research purposes. 29 The reasons for GPs' lack of participation in the survey are presented elsewhere. 30 It is possible that certain GPs within the sample are more likely to respond than others, perhaps because of their interest in the research area. Thus, the data probably presented a ‘best-case’ scenario in STI care. One of the other limitations of the study is that it was based on self-reported responses, where the possibility of idealistic responses (as opposed to realistic) cannot be ruled out. A qualitative study could explore providers' attitudes that can play a key role in creating supportive environment for STI prevention. 6
CONCLUSIONS AND POLICY IMPLICATIONS
The present study demonstrates clear evidence of inconsistent involvement of GPs in STI-prevention activities, and suggests that there is much to be gained from strengthening sexual-health promotion in general practice. Lack of time and funding appear to be the major barriers to sexual-health promotion, while there is a compelling case for improved medical education in this area. It is worth knowing about how promotional activities in general practice can be funded and which would be the most efficient reimbursement mechanism. There is also a need for an operational definition of ‘sexual-health promotion’, especially in the context of what is possible in primary care settings.
Footnotes
ACKNOWLEDGEMENTS
We are indebted to Dr David Bradford, Past President of the Australasian College of Sexual Health Physicians for his ongoing support and valuable advice during the study. We also thank Dr Suzanne Robertson, Dr Elizabeth Pringle, Dr Miriam Grotowski and Dr Jan Browne for their valuable input in developing the study instruments. We are very grateful to all GPs who participated in the study. An Institutional Research Grant from the University of New England supported the study. Ethical approval was obtained from the Human Research Ethics Committee of the University of New England, Australia.
a
Medicare is Australia's central health care insurance scheme that, in general, reimburses a major share of costs required for any particular medical service.