
Abstract
Summary
This study aimed to compare the outcome of an elderly group of AIDS patients with that of a younger group and their features at the time of the diagnosis of AIDS. We evaluated 58 patients aged >60 years and 114 aged 20–39 years, followed for 35.3 months. There was an obvious delay in diagnosing the elderly as they had more AIDS-defining diseases at diagnosis and their most frequent opportunistic infection was pulmonary tuberculosis. Mortality at the time of the diagnosis of AIDS was four times higher in the elderly (24.1% versus 6.1%, P < 0.001). However, when comparing only those submitted to highly active antiretroviral therapy, there was a similar frequency of favourable outcomes; 76.9% in the elderly against 83.1% in the young (P = 0.455). Mean CD4 lymphocyte was 438 cells/mm3 at the end of follow up in the young when compared with 442 cells/mm3 in the elderly (P = 0.945). The types of antiretroviral schema and the number of antivirals per patient were similar in both groups.
INTRODUCTION
Almost 474,273 cases of AIDS had been notified to the Brazilian Ministry of Health by June 2007. A total of 11,110 (2.3%) of these cases occurred in people aged 60 years or older. 1 However, this prevalence will probably increase as highly active antiretroviral therapy (HAART) contributes increasingly to the emergence of a larger contingent of those infected with HIV/AIDS surviving longer, and passing the threshold of 60 years. 2–4 Moreover, the drugs that improve male sexual function 5 , the difficulty of older age women in asking their partners to use condoms 6 , the physiological alterations of the climacterium 7 and the lack of preventive and specific educational measures for such a population 8,9 certainly contribute to the increasing frequency of the infection in this age group.
There is uncertainty about the efficacy of HAART in elderly patients. Most studies suggest that the control of viral replication is similar in the young and the old. 10–13 On the other hand, immune system reconstitution (recovery of the CD4 lymphocyte count) seems less intense and slower in older patients. 9,14,15
Brazil is a country with one of the world's fastest increase in the elderly population. 16 Although epidemiologists point to the growing number cases of AIDS in this age group 1 , there is little Brazilian data concerning the clinical and laboratorial outcomes elderly patients using HAART. We therefore conducted the present study in order to describe and compare the epidemiological and clinical aspects of elderly (>60 years) and young (20–39 years) patients with HIV/AIDS and to compare the virological and immunological outcomes of these patients when submitted to HAART.
PATIENTS AND METHODS
All the patients diagnosed as having AIDS by the Department of Infectious Diseases of the Hospital das Clinicas of the Federal University of Pernambuco and by the Hospital Correia Picanço of the State Department of Health located in Recife/Pernambuco aged 60 years or over, during the period of February 1996 to May 2005, were selected from the database of the State Department of Health's compulsory notification system. Both hospitals are references in the care of HIV/AIDS patients. The criteria for AIDS definition was that used by the Brazilian Ministry of Health, which included CD4 lymphocytes below 350 cells/mm3, or symptoms or opportunistic diseases related to AIDS. The study was approved by the Ethics Commission of the Health Sciences Center of the Federal University of Pernambuco (Protocol Number 057/2005 CEP/CCS).
The study had a hybrid design. In the first part, the biological, clinical and virological features of all the patients >60 years diagnosed with AIDS by the two hospitals during the period of the diagnosis of AIDS were described they were compared with the control group, which was composed of young people aged between 20 and 39 years with a diagnosis of AIDS, in a ratio of two controls for each case. The matching of cases and controls was done based on the date of the diagnosis of AIDS by the hospital where the patients were followed, and by sex. In the second part, a retrospective case-control study was carried out in which all the elderly patients included in the descriptive study, who had been submitted to HAART, were selected as cases.
Those patients who fulfilled the criteria of indication for antiretroviral treatment based on the 2002 Consensus in Antiretroviral Therapy for Adults of the Health Ministry (Brazilian Ministry of Health 2002), i.e. CD4 lymphocyte count below 350 cells/mm3, symptoms or opportunistic diseases related to AIDS, were given antiretroviral treatment funded by the Brazilian Government.
The patient was considered treated with HAART if a combination of two nucleoside reverse transcriptase inhibitors with a protease inhibitor (with or without booster) or a non-nucleoside reverse transcriptase inhibitor was used. For the analysis of the therapeutic response, those patients who died during their first hospitalization and those whose duration of treatment was less than six months were excluded from the analysis of the therapeutic response. Almost 9% of the cases and controls were excluded from the study because they had not been using HAART for more than six months (Figure 1).
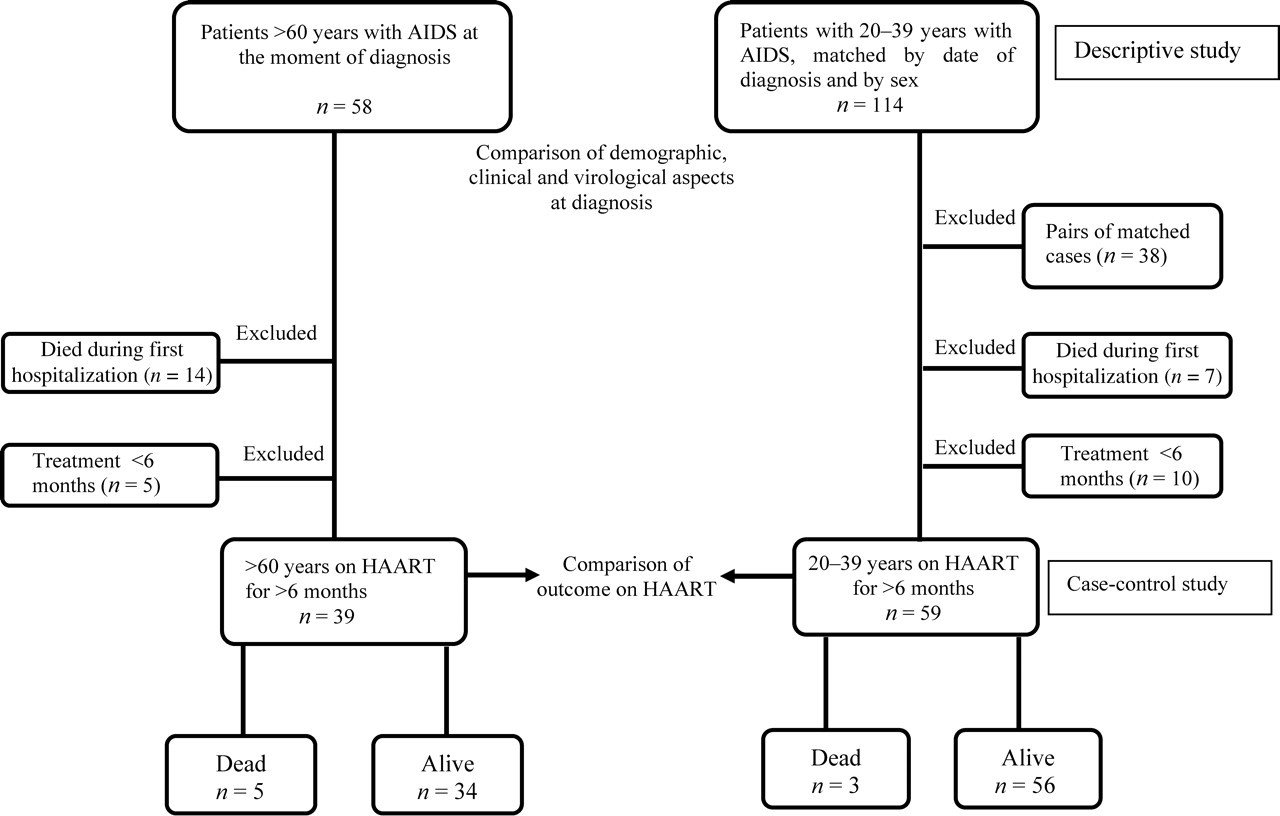
Flow chart showing the comparison of elderly with young patients with AIDS in a descriptive study of the period of diagnosis (first part) and in a case-control study of those with greater than six months on highly active antiretroviral therapy (second part)
Patients whose deaths occurred in one of the two hospitals, but who had initiated HAART in another hospital, and the individuals whose medical records contained insufficient information were also excluded from the study.
Laboratory assays
Laboratory data included the T-CD4 lymphocyte counts evaluated by flow cytometry, and the viral load in copies of RNA per millilitre measured in the plasma by the quantitative polymerase chain reaction with a minimum limit of detection of 400 copies/mL and maximum value of 750,000 copies/mL (Amplicor Roche, Diagnostic Systems, Somerville, NJ, USA).
Outcomes
Outcome was considered favourable when the patient achieved one of the following: (a) immunogical success – CD4 lymphocyte count >200/mm3 at the end of the study or an increase of 20% in the number of these cells when compared with the number at the start of HAART; (b) virological success – undetectable viral load (<400 copies/mL) at the end of the study; (c) viro-immunological success – patients who fulfilled both the abovementioned criteria. The outcome was considered unfavourable when one of following events occurred: (a) death; (b) loss to follow-up – patients who did not return for consultation after starting treatment; or (c) therapeutic failure – when the CD4 lymphocyte count was below 200 cells/mm3 at the end of the treatment or did not increase by even 20% in relation to the initial value or a viral load superior to 10,000 copies/mL, or the occurrence of a new opportunistic disease more than 180 days after the start of the antiretroviral therapy.
Statistical analysis
The quantitative variables were compared using the Student's t-test or Mann-Whitney test. Differences of proportions were evaluated through the Chi-squared test or, when the sample was small, by Fisher's exact test. For matched samples that did not meet the conditions for the Student's t-test, Wilcoxon's test of signalled positions was used. The level of significance of 0.05 was adopted in all tests. The Minitab 14.1 program (Minitab Inc, PA, USA) was used to perform the statistical analysis.
RESULTS
Epidemiological and clinical aspects
A total of 58 elderly patients (cases) and 114 young patients (controls) were included in the initial descriptive study. Table 1 summarizes the demographic and clinical characteristics of the patients. Only risk behaviour for HIV acquisition and AIDS index diseases did not present homogeneous distributions among the groups.
Clinical, biological and epidemiological features of 58 elderly and 114 young patients with AIDS at their first presentation
*Two cases and four controls have missing information about their marital status
†Sixteen cases and four controls have misssing information about their risk behaviour
‡Nine cases and 22 controls without information about CDC-AIDS classification
§One case without information about índex diseases
RMR = Recife metropolitan region; IVDU = intravenous drug user; CDC = Centers for Disease Control and Prevention classification of the HIV infection (1993)
Elderly patients were attacked significantly more often with AIDS index diseases at the time of HIV diagnosis than the young (P < 0.001). The most frequent diseases were consumption syndrome (36.6%) and oesophageal candidiasis (17.0%). The young group presented consumption syndrome (35.1%) and Pneumocystis jiroveci pneumonia (24.5%) more frequently.
During the follow-up period, 31% of the elderly group and 36.4% of the control group presented with opportunistic infections. The former predominantly with pulmonary tuberculosis (25%), oesophageal candidiasis (20.8%) and P. jiroveci pneumonia (12.5%). The young patients were more frequently attacked by neurotoxoplasmosis (19%), P. jiroveci pneumonia (15.8%), pulmonary tuberculosis (11.1%) and herpes zoster (11.1%).
The proportion of deaths was higher among elderly patients (P < 0.001); 19 deaths (32.8%) occurred among the cases and 10 (8.8%) among the controls. Fourteen cases and seven controls died during their first hospitalization, when they were diagnosed for the first time as having AIDS, when they had little chance of benefitting from treatment with HAART. In this situation, the risk of death for an elderly patient was about four times higher than for a young one (24.1% versus 6.1%; P < 0.001). The elderly presented the following causes of death: sepsis syndrome (7), acute respiratory failure (4), acute renal failure (3), upper digestive tract haemorrhage (2) and acute respiratory infection (2). In one case, the cause of death was not determined. Interestingly, the young patients died from almost the same causes as the elderly: sepsis syndrome (5), acute respiratory failure (3), acute renal failure (1) and respiratory infection (1).
Case-control study
Of the 58 elderly patients, 14 died during their first hospitalization and five did not received HAART for more than six months. Therefore, a total of 39 patients was submitted to HAART and were included as cases in the case-control study. Among the 114 controls in the descriptive evaluation, 38 corresponded to the pairs of excluded elderly patients of the case-control study, while another seven patients died during their first hospitalization and 10 were not submitted to HAART for more than six months. The remaining 59 controls were compared with the cases.
The mean initial and final T-CD4 lymphocyte counts of cases and controls were similar, and were significantly higher at the end of the treatment (Table 2).
Basal and final values of CD4 lymphocytes and viral load of HIV
*Missing data from six young and 10 elderly patients
†Missing data from nine young and 13 elderly patients
The mean values of initial and final viral load were similar in both groups and there was a significant and similar reduction among cases and controls (Table 2).
Table 3 presents the distribution of patients according to age and characteristics of the HAART. There were no significant differences between the type of antiviral schema (P = 0.536), the number of antivirals per patient (P = 0.176), the period of follow up (P = 0.254), the mean period of time between the diagnosis of AIDS and death (P = 0.104), or between the mortality of seniors and young persons submitted to HAART (P = 0.15).
Features of highly active antiretroviral therapy scheme used in young and elderly patients
NRTI-Nucleoside analogue reverse transcriptase inhibitor; *PI-Protease inhibitor; NNRTI-Non-nucleoside analogue reverse transcriptase inhibitor
The outcomes of the elderly and young patients are shown in Table 4. There were no differences in the favourable and unfavourable outcomes (P = 0.455) between the two groups. The viro-immunological success was also similar in both groups and occurred in 69.2% of the elderly and 71.2% of the young people (P = 0.314).
Distribution of patients by age and outcome
*Comparison between favourable and unfavourable outcomes (P = 0.455)
The frequency of patients who achieved an undetectable viral load (<400 copies/mL) in their final examination was 88.5% in the elderly and 76% in the young submitted to HAART (P = 0.238). Among the elderly patients submitted to HAART, 82% achieved a CD4 count of over 200 cells/mm3 or a rise in more than 20% when compared with the initial values against 78.3% of the 53 controls who had this count evaluated (P = 0.653).
DISCUSSION
The present study has elicited two important findings. The first was the exceedingly high mortality among the elderly patients with AIDS, almost four times that of the young. Secondly, this mortality often occurred the first time they presented for hospitalization, which was almost always when they first became aware of their HIV-positive condition. On the other hand, the study also showed that when they were submitted to HAART, the immunological and the virological responses and the mortatily did not differ between the groups.
Several aspects observed in the present study suggest that there was a delay in the diagnosis of AIDS and difficulty in detecting risk behaviors among the elderly: a lower detection of homosexuality, a higher frequency of immunosuppression and AIDS index diseases at the time of diagnosis of HIV infection among the elderly (although the difference was not significant): and, finally, the early mortality that was much more intense in this age group. The low rate of clinical suspicion of AIDS among the elderly has already been reported by El-Sadr and Welter 12 . In their study they found 5.05% of HIV-positive patients among a cohort of elderly who died in a general hospital from causes not related to HIV and in whom the infection was not identified. The large number of comorbidities in the geriatric population may modify the presentation and clinical course of the disorders associated with the virus, increasing the complexity of the diagnosis. 13 Moreover, the occurrence of atypical presentations can also delay the diagnosis of HIV infection or the diagnosis of other disorders associated with AIDS. 17 Regarding risk behaviours for HIV acquisition, two North American studies conducted in Baltimore and Michigan showed that there were significantly more homosexual patients <50 years of age when compared with those >50 years. 18,19 Other studies have not detected any significant differences between forms of sexual infections when comparing the older groups with younger ones. 19–21 Possible difficulties in the approach to sexuality in the elderly group could have resulted in the under-reporting of homosexuality in this age group in the present study.
Considering that (1) overall mortality among AIDS patients has decreased significantly since the introduction of HAART (2) that the probability of a five-year survival of AIDS patients attending or hospitalized in the Department of Infectious Diseases of the Hospital das Clinicas of the Federal University of Pernambuco is almost 75% 22 and (3) that there is a free access to medication for all AIDS patients in the region as part of the Brazilian Ministry of Health's National AIDS/STD Programme, we can conclude that there is still an exceedingly high mortality among elderly patients with AIDS as detected by Nogueras et al. 23 in Spain.
Pulmonary tuberculosis, oesophageal candidiasis and P. jiroveci pneumonia were the most frequent opportunistic infections among the elderly patients in the present study, unlike studies performed in developed countries. 24,25 In an evaluation made before the introduction of HAART, Raviglione et al. 25 described tuberculosis as the most frequent opportunistic infection in several developing countries. The high prevalence of this infection in Recife, and in Brazil as a whole, must have been responsible for the high frequency of the disease in this study.
On the other hand, when considering only the patients who were submitted to HAART (case-control study), there were a high percentage of favourable outcomes in the two groups evaluated, with no statistical differences between them. When virological and immunological responses of the two groups were compared, we again observed a high percentage of favourable outcomes.
The frequency of patients who obtained a 20% increase in cells from the initial count, or attained CD4 counts of over 200/mm3 at the end of the study, was high and statistically different from the initial values in both groups. Regarding the viral load, the same results were obtained regarding the goal of making it undetectable in the groups evaluated. We thus suggest that both elderly and young patients seem to have a similar immunological and virological response to HAART.
Other authors have reported similar outcomes among young and senior patients. 18,21 In a recent study, in Rome, Tumbarello et al. 24 prospectively evaluated 120 individuals >50 years of age and compared them with 476, aged 20–35 years, undergoing treatment with HAART. Although the older group presented initial CD4 counts lower than those of the controls, the multivariate analysis showed that there were no statistically significant differences in viro-immunological outcome between the groups.
On the other hand, the results of this study are at variance with those of other studies, in which there was a similar virological response in young and senior patients submitted to HAART, but a poor immunological response regarding both intensity 14,15 and speed. 26 Even among the authors who describe a worse immunological response in the elderly, there is a certain consensus that virological outcomes resemble those of young people. 14 However, there seems to be no association between an inadequate immunological response and worse clinical outcomes in older patients. 14 In these studies, the authors argued that factors associated with the ageing of the immune system are responsible for the unfavourable progression of the CD4 counts.
Thyme involution may play an important role in this process by reducing the regenerative capacity of the immunological system in the elderly. 14,26,27 Other physiological changes previously described in older individuals were a reduction in the number and in the immune response capacity of the mature T cells, a decrease in the production of cytokines, diminution of granulocyte function and primary defects in B cells. 28 However, the exact role of these changes and their repercussion on the physiopathogenesis of HIV infection in the elderly remains unclear.
The average period of follow up of patients submitted to HAART in our study was long – almost three years. Shorter periods of follow up can produce bias, as the viral load usually becomes undetectable rapidly in the first month of treatment, while CD4 cells need a longer time to recover. 21 Grabar et al. 29 followed a prospective cohort of patients with ages above and below 50 years of age for an average of 31.5 months, and noted that, although there was an immunological response, the time required for immune restoration in the older age group was significantly longer than in the younger group. They suggested that this would produce an increased risk of clinical progression of AIDS. Thus, the studies that demonstrated an insufficient immune recovery might have suffered a bias, owing to insufficient time required for immune restoration.
There were no statistical differences in mortality between the two groups of patients submitted to HAART. Five elderly patients died – three from sepsis, one from acute renal failure and one from an unrecorded cause – compared with only three young people – two from sepsis and one from pneumocystis pneumonia – during the period of evaluation of those submitted to HAART.
The delay in diagnosing HIV infection as well as the AIDS index diseases resulted in elderly patients being admitted at an advanced phase of the disease, and this seems to be one of the main obstacles to the recovery of geriatric patients in the region. However, data from this study demonstrate the feasibility of treatment of the senior population suffering from AIDS and strongly suggest that there be no restrictions on the use of antiretroviral therapy in the geriatric population.