
Abstract
Summary
The aim of this study was to investigate consultant genitourinary (GU) physicians' and health advisers' views regarding acceptability of patient-delivered partner therapy (PDPT) in the United Kingdom (UK). A postal questionnaire was sent to all consultant GU physicians and senior health advisers: 206 (65%) physician questionnaires and 153 (77%) health-adviser questionnaires were returned. One hundred and three (50%) physicians and 31 (22%) health advisers reported ever having used PDPT. Approximately one-third of professionals are strongly opposed to PDPT. However, the majority of both professional groups are cautiously prepared to consider PDPT, but only if there is no other option and only if a health professional first makes contact with the partner. Chief concern among health professionals is the legal status of PDPT in the UK. Here, the current General Medical Council (GMC) guidance on remote prescribing is helpful. The outcome of the Medical Research Council randomized controlled trial on accelerated partner therapy, which fits in with GMC guidance, is eagerly awaited as professionals would welcome evidence-based national guidance.
INTRODUCTION
Sexually transmitted infections (STIs) have risen significantly over the past decade in the United Kingdom (UK). 1 Genitourinary (GU) medicine clinics have struggled to cope with the rising demand, undergoing considerable modernization and redesign of services. However, GU medicine clinics still need to continue to examine all aspects of the service they provide and explore new ways in which services can be delivered in the future in the face of continuing increasing demand and restricted resources.
Assuring treatment of infected patients' sexual partners has always been an essential component of STI control. 2 A recent systematic review in the BMJ 3 suggested that patient-delivered partner therapy (PDPT) might improve STI control particularly with regard to chlamydia and gonorrhoea. PDPT is the practice of treating the sexual partners of patients with STIs by providing prescriptions or medications to the index patient to take to his/her partner(s) without the health-care provider first seeing the partner. PDPT has not been used in the UK, but its use has been studied in the United States (US) and the Centre for Disease Control (CDC) has produced guidance on providing PDPT for US physicians. 4
We undertook a postal survey to investigate both consultant GU physicians' and health advisers' views regarding acceptability of PDPT and to determine the proportion of these professionals who might welcome this approach as an additional treatment option that would not replace traditional methods for partner management, but would complement them as one component of a coordinated strategy.
METHODS
A confidential questionnaire was sent to all consultant GU medicine physicians and to senior health advisers at GU medicine clinics listed in the A–Z Clinic Directory on the British Association for Sexual Health and HIV (BASHH) website. 5 A reminder letter was sent to non-responders after one month. The questionnaire asked whether professionals had given PDPT in the past, whether they might consider future PDPT use, which infections and which antibiotics might be suitable for PDPT. Attitudes about PDPT were assessed using a series of statements for which agreement was measured using a five-point Likert-like scale: strongly agree, agree, neutral, disagree and strongly disagree.
The data were anonymized and analysed in Excel. Statistical analysis was performed using a two-tailed test of proportions. Responses to attitude statements were dichotomized (strongly agree and agree versus other responses) for statistical comparison. Statistical significance was considered when a P value was 0.05 or less.
RESULTS
There are currently 315 consultant GU physicians in the UK (GU medicine Royal College of Physicians' Workforce Officer, 2007). A total of 206 questionnaires were returned from GU physicians giving a physician-response rate of 65%. Out of 200 senior-health-adviser questionnaires that were sent, 153 were returned giving a health-adviser-response rate of 77%.
Table 1 shows past use and attitudes of the two professional groups towards PDPT. Fifty per cent of GU physicians reported ever having used PDPT. They were significantly more likely than health advisers to report having given PDPT. A higher proportion of each professional group would consider giving a home-testing kit.
Past use and attitudes of GU physicians and health advisers towards PDPT
GU = genitourinary; CI = confidence interval; PDPT = patient-delivered partner therapy
Figure 1 shows positive attitudes towards PDPT for individual infections and Figure 2 shows positive attitudes to specific antibiotics. A smaller proportion of GU physicians compared with health advisers believed that no conditions and no antibiotics would be suitable for PDPT and a higher proportion thought individual infections and specific antibiotics would be appropriate for PDPT, but the differences were not significant.

Positive attitudes of patient-delivered partner therapy for various infections (GC = gonorrhoea; NSU = non-specific urethritis; PID = pelvic inflammatory disease; Trichs = trichomonas)
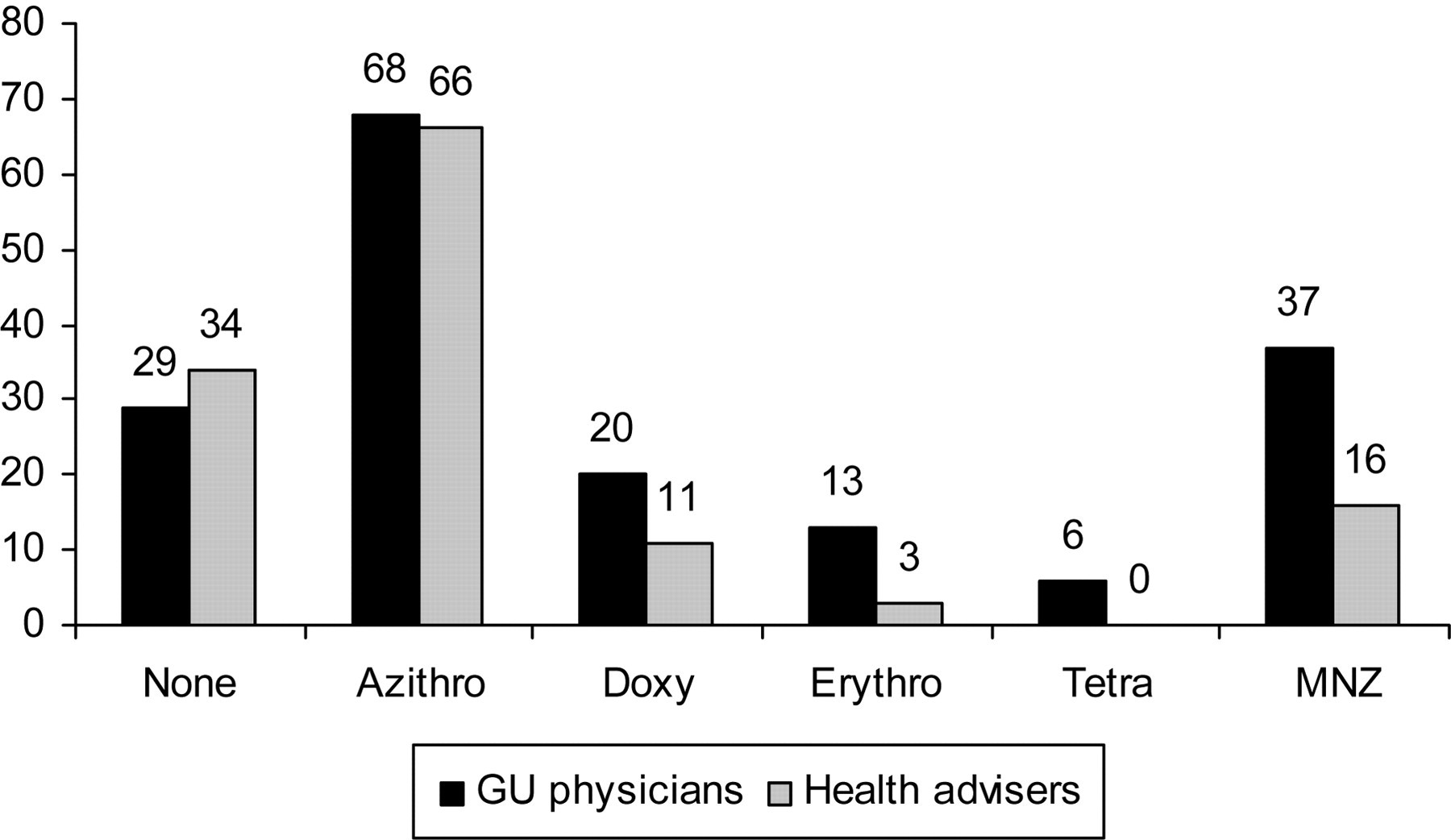
Positive attitudes of patient-delivered partner therapy for various antibiotics (Azithro = azithromycin; Doxy = doxycycline; Erythro = erythromycin; Tetra = tetracycline; MNZ = metronidazole)
Table 2 shows positive responses (strongly agree and agree) of GU physicians and health advisers towards the various statements. GU physicians were significantly more likely than health advisers to believe that PDPT could be useful in achieving better outcomes, that PDPT protects patients from re-infection and that benefits may outweigh disadvantages.
Positive attitudes (strongly agree and agree) to statements about patient-delivered partner therapy
CI = confidence interval
Free text responses
Comments were numerous and varied, but they could be divided into three main themes: those against PDPT, those with concerns over the legal position of PDPT and those who believed PDPT may sometimes be the only option or the ‘least harmful’ option. (Physicians' quotes are denoted by P and health advisers' by HA).
Against PDPT
‘I believe PDPT is unsafe. It undervalues the role of sexual health interventions including risk reduction strategies. It is a disaster – drop the idea!’ (P)
‘Do not go down this slippery slope!’ (P)
‘I do not think PDPT is the best long-term option for addressing disease control. It is a cheaper option to spending money on properly trained health advisers’ (HA).
Those with concerns over legal position of PDPT
‘Depends on agreement at a national level and medicolegal clarification’ (P).
‘The legal requirements for prescribing would need to be changed to allow PDPT’(P).
‘Legal aspects may be a barrier to use’ (HA).
The least harmful option
‘This is an important risk management issue. PDPT is illegal in many US states – What is the status in the UK? Treatment of any individual without having performed a clinical assessment is fraught with difficulties – both ethical and clinical. It should never be considered an alternative to proper partner notification. There may be circumstances in which this is the least bad option’ (P).
‘I think this is an excellent debate and agree that it would complement traditional methods if implemented within robust protocols’ (HA).
‘You don't ask about the fact that it is a treatment of last resort – it is better than nothing, but other infections will be missed. I would only use it if no other option’ (P).
DISCUSSION
There are limited data on UK health professionals' views of PDPT. 6,7 To our knowledge this is the first study to seek views of GU medicine professionals nationwide and many of those who responded made comments to the effect that this was an important and timely debate. We achieved a response rate of 65% from GU physicians and 77% from health advisers. In the first letter to the physicians, we failed to emphasize that the numbering on questionnaires was only to allow a reminder to be sent and that the data were to be analysed anonymously. This was corrected for all subsequent mailings and may have accounted for the better health-adviser-response rate.
Partner notification is key to controlling STIs, but current methods of partner notification only reach 40–60% of named sexual partners. 8 Health professionals, who are increasingly involved in managing chlamydia, are largely in favour of adopting new strategies for treating sexual partners. 6 We found that the majority of physicians and health advisers believe that chlamydia (67% P:60% HA) would be the most appropriate infection and azithromycin (68% P:66% HA) the most suitable therapy for PDPT. This is no surprise as chlamydia is the most prevalent infection 1 and azithromycin is an effective single-dose treatment with a good safety record. It is in keeping with the published data 3,6,7 and in keeping with the public consultation on the request to reclassify azithromycin 500 mg from POM (prescription only medicine) to P (Pharmacy). 9
This survey found that approximately one-third of health professionals are strongly opposed to PDPT on the grounds of ‘poor medicine,’ ‘further dumbing-down of GU medicine,’ concerns over missed infections, emergence of resistance, potential allergic responses to treatment, etc. It is not surprising that health advisers were generally less in favour of PDPT than physicians, as they see more of the complex issues surrounding partner notification. Also, many health advisers emphasized that PDPT would mean health promotion opportunities would be lost. However, the majority of both professional groups were cautiously prepared to consider PDPT, but only if there was no other option and only ‘if the partner has attended our clinic in the past’ or if a health professional had ‘at least spoken to the partner on the phone’.
The chief concern among health professionals is the legal status of PDPT. The General Medical Council (GMC) guidance in Good Medical Practice 10 appears to preclude PDPT. Good Medical Practice states: ‘In providing good clinical care you must prescribe drugs or treatment only when you have adequate knowledge of the patient's health and are satisfied that the drugs or treatment serve the patient's needs.’ Doctors ignoring this guidance would put themselves in a very exposed position. However, recently the GMC has produced guidance on remote prescribing 11 acknowledging that from time to time it may be appropriate to use a telephone or other non face-to-face medium to prescribe medicines. This guidance states that if a doctor is not providing continuing care for the patient, does not have access to the patient's medical records and is not deputizing for another doctor (as would be the situation with PDPT), the doctor must have an appropriate dialogue with the patient. This dialogue (whether by phone, fax, email, video link or website) must establish that the doctor is prescribing safely (medical, drug and allergy history, etc) and that the patient understands the need for the treatment. The doctor should also make arrangements to follow progress of the treatment. A telephone discussion with the partner could cover all these aspects. This would ensure that there would be full comprehension by the partner and that there was no element of deceit or coercion on the part of the index patient to the partner.
Expedited partner therapy (EPT) includes strategies which reduce the time for contacts to be treated and in the US is virtually synonymous with PDPT. Accelerated partner therapy (APT) includes strategies which reduce the time to be treated and includes assessment by a qualified health professional. PDPT has not been a standard approach in the UK for the reasons mentioned, although increasingly, it appears that PDPT would be an acceptable choice with health professionals 6,7 and popular with patients. 7,12 APT fits in with the GMC guidance on remote prescribing 11 and is therefore permissible within existing law. There is currently an on-going Medical Research Council funded randomized controlled trial (RCT) on APT (Dr Escourt, BASHH OGM, October 2007). This allows the partner to have a telephone conversation or accelerated appointment with a health professional and rapid access to treatment (the partner is also actively encouraged to attend for follow-up and a full sexual health check after the appropriate treatment interval). The results of the RCT will be eagerly awaited, as it has the potential to provide the basis for evidence-based national guidance, and therefore to add an additional strategy to the control and management of STIs in the UK that would not replace, but would complement traditional methods for partner management. As part of a coordinated approach, this could lead to an increase in the proportion of sexual partners known to be treated.
Footnotes
ACKNOWLEDGEMENTS
Ethical approval for the study was given by the Plymouth and Cornwall Local Research Ethics Committee.