
Abstract
The Genitourinary (GU) Medicine Service was transferred from the Home Office to the NHS from April 2006 at this female prison to give prisoners access to the same quality of health care as the general public. Medline search showed no published data on the prevalence of sexually transmitted infections (STIs) among female prisoners in the UK. The main aim was to develop a one stop sexual health shop and to determine the prevalence and risk factors for STIs, to determine the uptake rate for HIV testing, hepatitis B vaccination and cervical cytology along with requests for usage of contraceptive services. Challenges were met when introducing change to bring the services in line with the local GU medicine clinic. Review of the service at one year along with retrospective case note review from May 2006 to August 2007 was done. Of the 545 new patients seen, history of substance abuse, IVDU, sexual abuse, sex worker and past history of hepatitis C virus and chlamydia were 86%, 41%,12%, 6%, 17% and 24% respectively. The uptake rate for both STI screen and blood-borne viruses (BBVs) testing was high at 87% and 69.3% respectively. STI was diagnosed in 19.6%. Prevalence rates were: Trichomonas vaginalis (TV) 8.2%, chlamydia 5.3%, gonorrhoea 0.2%, genital warts 5.3%, HIV 0.8%, hepatitis C virus 12% and hepatitis B virus 11%. The uptake rate for 1st dose hepatitis B vaccination and cervical cytology were 70% and 92% respectively, 36 accessed contraceptive services.
Provision of one stop shop in a female prison is feasible and practical. STIs, particularly TV, and BBVs prevalence is high among the female inmates. Prevention methods targeting this population needs to be intensified.
Keywords
Introduction
Traditionally prison health-care services in the UK had been provided by the Home Office. The transfer of prison health-care system to the National Health Service (NHS) from April 2004 was recommended to give prisoners access to the same quality of health care as the general public. 1 In response, the local primary care trust (PCT) commissioned the sexual health services in partnership with the Prison Services at Styal since April 2006.
There are several studies assessing the prevalence of HIV and blood-borne viruses (BBVs) in the UK in both male and female prison populations. 2 4 There is some data relating to sexually transmitted infections’ (STIs) prevalence among male prisoners and male youth offenders institute in the UK.5,6 However, Medline search showed no published data on prevalence of STIs among the female prisoners in the UK. Various studies have shown an association between substance abuse and commercial sex work among incarcerated women to elevated risks of reproductive health problems, including high-risk pregnancies and increased rates of STIs and HIV.7,8 Accurate information on prevalence of STIs and frequency of risk behaviours is important for developing preventive strategies, health-care planning and clinical intervention. 9
The Prison Performance Indicators 2007/2008 under the sexual health section mention that all prisoners should have access to a genitourinary (GU) medicine service, have access to a chlamydia screening programme, access to condom/barrier protection and lubricants. It recommends that all new receptions to prison where there is no verifiable evidence of previous vaccination to hepatitis B should be offered hepatitis B vaccination or where there is evidence of a started course it is continued and there is an uptake greater than 80%. 10
Her Majesty's Prison (HMP) Styal, is one of the largest of the 17 female prisons in the UK. It is a closed, medium security, training prison that holds adult women and young offenders. It has an operational capacity of approximately 459 inmates at any given time 11 and the annual turnover is approximately 3000. Prior to May 2006, the GU medicine service was provided by a visiting consultant employed by the Prison services.
A health needs assessment conducted by the local PCT in 2005 12 highlighted the need of a female doctor. In May 2006, a female consultant with dual qualifications in both GU medicine and family planning along with a female nurse with experience in both the above fields were appointed in addition to the existing GU medicine nurse.
There is currently one consultant-led session and four nurse-led clinics per week.
Patients attending the clinic are either self referred on individual request or in response to a question in the prison admission health - screening questionnaire or referred by the prison nurse or general practitioner.
The clinic is run in the health-care wing. There is availability of onsite wet film microscopy along with access to tests. Testing facilities include high vaginal swab for culture of candida, Gram stain of specimens from vagina for clue cells for bacterial vaginosis, Trichomonas vaginalis (TV) is tested by acridine orange on vaginal specimen, gonorrhoea culture on endocervical swab, nucleic acid amplification tests for both chlamydia and gonorrhoea (Aptima Combo 2 assay [Gen-Probe Inc., San Diego, CA, USA]) available on both invasive (endocervical) and non-invasive samples (self-taken vulvovaginal swab/firstvoid urine sample) and liquid-based cervical cytology. Serological tests includes testing for syphilis, HIV and BBVs including hepatitis B and C.
All women with bacterial, parasitic and viral infections are offered treatment according to the national guidelines for the treatment of STIs. 13
Prisoners are allowed to keep their own treatment if they live in dormitories, if in cells, then it is held by the nursing staff.
Objective
The main aim of the new service was to provide sexual health care in-line with the local GU medicine clinic based at Macclesfield, to determine the prevalence and risk factors for STIs, ascertain the hepatitis B vaccine uptake rate and requests for the usage of contraceptive services.
Method
Retrospective case-note review of all patients attending the clinic from May 2006 to August 2007 was done. Data on demographics, clinical information, hepatitis B vaccination status, diagnoses made, contraceptive service usage were collected. Data were entered on excel and analysed using SPSS (SPSS Inc., Chicago, IL, USA).
A general review of the service at just over one year since being transferred to the NHS was done.
Results
The total number of attendances was 865 (both new and followup patients). Of the 545 new patients seen, the mean age was 30.6 (range 17-68) and the average number of sexual partners in the previous six months was four. Table 1 and Table 2 show the characteristics of inmates and investigations done/reasons for attending and diagnoses made, respectively.
Demographics and characteristics of inmates
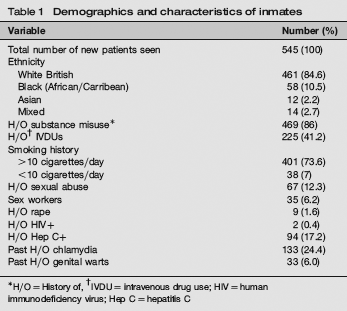
H/O = History of,
IVDU = intravenous drug use;
HIV = human immunodeficiency virus; Hep C = hepatitis C
Investigations/reasons for attending clinic and diagnoses made in new patients

HIV = human immunodeficiency virus; Hep C = hepatitis C; BV = bacterial vaginosis; TV = Trichomonas vaginalis; BBV = blood-borne virus infection; STI = sexually transmitted infections; PCR = polymerase chain reaction; Hep B = hepatitis B
Discussion
Styal prison falls under the green performance category when measured against the sexual health section of performance indicators standards 10 as all facilities mentioned above are available and accessible.
The majority (85%) of the inmates are white. The uptake rate for both STI screen and HIV/BBVs testing was high at 87% and 70%, respectively. Of those having an STI screen, 19.6% (93/474) were diagnosed with an STI. This study shows that STIs and BBVs prevalence in female inmates is high, particularly TV, hepatitis C and hepatitis B virus infection. Nearly half of the patients who had indulged in substance misuse had also been intravenous drug users (IVDUs). Various studies have found the association of IVDU and BBVs to be strong.14,15
The prevalence of anti-HIV, hepatitis C infection and the presence of hepatitis B core antibodies in our study population was very similar to that of Wield et al. 2 ‘s female substudy population (0.8%, 12.2% and 11.4% versus 1%, 11% and 12%, respectively). Wield et al. 2 in their survey of eight of the 135 prisons in England and Wales, one being a female prison found that 7% of adult males and females reported injecting inside the prison and three quarters of those who injected in prison reported sharing needles or syringes whilst inside.
Women in prison are also particularly at a high risk of unplanned pregnancies when leaving prison. These women may contribute to heterosexual and perinatal transmission of HIV, BBVs and STIs and, therefore, represent a high yield group for prevention strategies. Prevention efforts for IVDUs both in the community and during imprisonment need to be intensified. In the prison, the measures to reduce BBVs include health promotion, vaccination against hepatitis B, 16 various options for coming off drugs 17 and treatment with methadone for opiate withdrawal. 18 Those patient needing treatment for HIV and active hepatitis B and C infection were referred to local specialist clinics.
Styal prison has a unique ‘first night centre’. 19 The unit provides support for women during their first 48 hours in custody and includes access to health care, probation and other agencies within the prison. Although there is a policy of offering hepatitis B vaccination to all inmates on ‘first night screen’, this does not always happen as from the data given from Table 3, where majority were unvaccinated when presenting to sexual health clinic. Bird et al. 20 in their Scottish prison study found that only 4% of inmates had ever been offered vaccination against hepatitis B. Plugge et al. 21 in a questionnaire survey in two female prisons in England found that of the 505 responders, 46.8% reported of having received one vaccine against hepatitis B at some time and 27.3% had had at least thee injections. Although the sexual health clinic has performed well with a 70% uptake rate of first dose of hepatitis B vaccination, this needs to increase further to 100%. The regimen used is the accelerated regimen, where the first three dosages are given a week apart and the last dose at one year. Uptake of the three dosages has been difficult to evaluate for patients receiving the first dose of hepatitis B vaccination in our clinic, as they are booked in a separate clinic under the prison number and this is recorded separately. Means of improving data collection need to be looked into.
Hep B vaccination status, cervical smear uptake rate and contraceptive usage
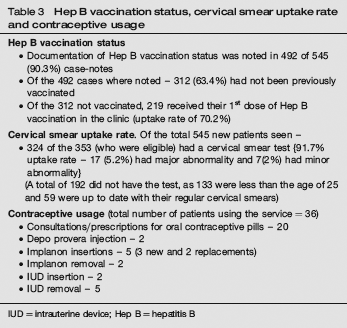
IUD = intrauterine device; Hep B = hepatitis B
When the waiting list was inherited in May 2006, it was up to six weeks long; however, with increase in staffing levels and increase in clinical sessions from one to five sessions per week, waiting list is virtually non-existent. However, high DNA (did not attend) rates of 38.4% is a major problem, often multifactorial, reasons similar to those as mentioned in Sherrard's 6 and Tang's 22 article, compounded by lack of escorts to bring patients from cells to the health care. Clinics are usually overbooked to compensate for this high-DNA rates.
Partner notification although being pursued is difficult. Majority of the inmates have had casual sex and, therefore, do not have details of their contacts. Where contacts are known, inmates are encouraged to disclose the nature of their infection to their sexual partners either by phone or during visits for being tested and treated in a GU medicine clinic.
As noted in other studies,23,24 we too found a strong association of IVDU with amenorrhoea. Of the 84 women who were amenorrhoeic, 78 (93%) were IVDUs (P < 0.001), chi-square test. The perceived importance of contraception is thus reduced in this population and likelihood of so-called unplanned pregnancy is increased. Although menstruation ceases, ovulation may continue. 25 Although not many women have used the contraceptive services in our study, certainly, we have been able to set-up a successful one-stop shop sexual health clinic to address the varied sexual health needs of this population and tailoring services to women's specific pregnancy attitude may aid in preventing unplanned pregnancy in such a high-risk population. Clarke et al. 25 found that women with negative pregnancy attitudes were significantly more likely to want to start or to continue a birth control method compared with those with ambivalent pregnancy attitudes (66% versus 47%). In another paper Clarke et al. 26 concluded that provision of contraceptive services to women during their incarceration greatly increased the birth control initiation when compared with providing services in the community. 26
Challenges were met when introducing change in May 2006. Particular difficulty was faced in changing the culture in working practices and constant staff shortages within the prison leading to the GU medicine nurse being taken away to dispense methadone, thus, leaving the clinic short of a nursing staff. However, with support from the PCT with increase in staffing levels, we have managed to bring the GU medicine service/sexual health care in-line with the NHS services as shown in Table 4.
Review of the genitourinary (GU) medicine service one year on, since being transferred to the National Health Service (NHS)

PCT = primary trust centre; STI = sexually transmitted infections; TV = Trichomonas vaginalis
KC60 code: (Each diagnosis at a clinic is assigned a KC60 code that defines the condition. KC60 data from GU medicine clinics in the UK are sent quarterly to the
CDSC (Communicable Disease Surveillance Centre)
Really, the transfer of the prison health care to the NHS has not only seen the development of a high-quality GU medicine service but also the provision of contraceptive services, thus, providing a holistic sexual health care under one roof within the prison.
Conclusion
Transfer of the prison health care to the NHS has made it feasible for prisoners to access the same quality of sexual health services as the general public. Provision of a one-stop sexual health clinic in a female prison is feasible and practical. STIs particularly TV and BBVs prevalence are high among the female inmates. Prevention methods targeting this population needs to be intensified.