
Abstract
Here, we present a 20-year-old man who presented with painful inguinal and femoral masses. He gave a history of sexual contact with a mare 14 days before his recent illness. He was diagnosed with lymphogranuloma venereum based on the histopathological findings and a high titre of IgG (1:1400).
Introduction
Lymphogranuloma venereum (LGV) is a sexually transmitted disease (STD) caused by Chlamydia trachomatis serotypes L1, L2, and L3. 1 LGV is a rare disease in industrialized countries, but it is endemic in parts of Africa, Asia, South America and Caribbean. 2 Recently, LGV infections have been encountered frequently in industrialized countries among men having sex with men. Here, we report another unusual LGV case in an industrialized country.
Case Report
A 20-year-old man, working as a shepherd, referred to our centre because of painful inguinal and femoral masses. He was not suffering from fever, malaise, weakness, rectal pain, tenesmus, urethral discharge but gave a history of small papules on his penis 10 days before admission. He was not married, and did deny having any sexual contact with anyone but had unprotected vaginal sexual contact with a mare 14 days prior to his present illness. At the time of admission, his temperature was 37° C and pulse rate was 90/min. Respiratory rate was 20/min and blood pressure was 105/ 80 mmHg. Two non-ulcerated, tender, firm, fluctuating and mobile masses were palpated in his right inguinal and femoral regions. Their sizes were 5 × 1 and 1 × 1 cm, respectively that caused the characteristic ‘groove sign’. The laboratory test results were as follows: leukocyte count 11.1 × 109/L (neutrophils 67%), platelet count 427 × 109 /L, erythrocyte sedimentation rate 35 mm/h. In smear examination from samples obtained from the swollen area, no intra- or extracellular bacteria was seen, but there were many polymorphonuclear cells. In the culture of the drained fluid from the lesion, no bacteria grew after four days. Immunoflourescence testing for C. trachomatis was positive (IgG [1:1280] and IgA [1:160]). In addition, the patient's serum was also reactive (IgG Biomerieux MIF, The Netherlands) for the LGV serotype of C. trachomatis (1:1400). Histopathological study of the tissue obtained by biopsy was consistent with the diagnosis of LGV (Figure 1). A tissue sample was examined for the presence of Chlamydiaceae-speciiic LPS
3
and the result was negative. Realtime polymerase chain reaction (PCR) (TaqMan) was used to assess the C. trachomatis DNA and LGV DNA
4
in the paraffin coupes of the tissue obtained by biopsy. No C. trachomatis or LGV DNA was detected. With these overall findings, the patient was diagnosed as having LGV. Doxycycline (2 × 100 mg/day p.o.) was started. The patient received this treatment for 10 days and then he was discharged from our centre. He was prescribed the remaining medication (doxycycline 2 × 100 mg/day p.o. for 11 days). At the time of discharge, patient was not suffering from any pain in the region and the swollen part had decreased in size significantly.
Histopathology of the lymph node: central, stellate necrosis with neutrophils, surrounded by a palisading of histocytes (stellate abscess) (Haematoxylin and eosin stain × 40)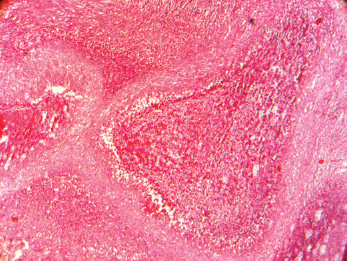
Discussion
Here, we presented a young man who developed LGV after reported sexual contact with a mare (a female donkey). The chlamydial IgG serology was very high (1:1200), a value not found in normal STD patients with non-LGV C. trachomatis ser-ovars (D-K). This has also been described previously in a study in Amsterdam, emphasizing a very high positive predictive value of IgG serology titres for LGV infection. 5 The fact that neither chlamydial membrane parts could be detected by immunohistochemistry nor chlamydial DNA could be shown by realtime PCR in this case, could be explained by the fact that the initial infectious origin was cleared at the stage of necrotizing granulomatous lymphadenitis. In The Netherlands in comparable cases among men who had sex with men also no LGV DNA was present in the biopsies or aspirates of the lymph nodes (personal communication S.A. Morré).
Although there are several studies on the occurrence of C. psittaci and C. pneumoniae in horses,6–9 C. trachomatis has not been found in female horses. 6 The situation in donkeys has not been studied yet, but it might be similar to horses. As LGV is not a natural pathogen in mares, either LGV has been transmitted through another man to the mare or the reported acquired route of transmission was reported to hide transmission with (homo) sexual contact. However, our patient denied having sex with a male or female person, and based on the social and economical status, and sexual and behavioural variables in his country, it is highly unlikely that the patient had acquired this LGV infection through sexual contact with a human person, but we cannot exclude this. Unfortunately, it was impossible to identify the mare and obtain material to further substantiate the alleged transmission route.
Until now, reports of LGV include patients who had sexual contact with a human partner, 1 but unlikely and unusual transmission of STDs has been described before, for instance the transmission of Neisseria gonorrhoeae through an inflatable doll. 10
We suggest taking a careful history of having sexual relation with animals in LGV patients who deny having sexual contact with a man or woman in those cultures where having sex with partners while being unmarried is unlikely and/or in cultures where zoosexual activities are known to take place.
Footnotes
Acknowledgement
We would like to thank Drs D Taheri and M Mahzad who provided histopathological document. The patient gave informed consent.