
Abstract
HIV-associated nephropathy (HIVAN) is almost exclusively seen in African-Americans (AA) and is rare in Caucasians. The mechanisms responsible for the predilection of HIVAN in AA are not well understood. In transgenic mouse studies, genetic background plays a vital role in the development of the HIVAN phenotype. Larger studies in humans have been initiated to study genetic polymorphisms responsible for HIVAN. As our case illustrates, HIVAN should be considered in Caucasian patients with HIV infection complicated by nephrotic syndrome and renal failure.
INTRODUCTION
HIV-associated nephropathy (HIVAN) is a well-known complication of an HIV infection. It is almost exclusively seen in African-Americans (AA) and to some extent in Hispanics. Here, we report a case of HIVAN in a Caucasian patient, and we review the literature on HIVAN in Caucasians.
CASE REPORT
A 52-year-old Caucasian man with a history of AIDS and hepatitis C virus (HCV) was referred for chronic kidney disease. He had a history of IV drug abuse and contracted HIV about 20 years ago most likely from needle sharing. Both his parents are Caucasian. His serum creatinine increased from 194 to 273 µmol/L over four months before the nephrology consultation. His 24-hour urine protein increased from 1.9 to 6.2 g. His past history was significant for biopsy proven Indinavir-associated interstitial nephritis about 10 years ago. This patient had been non-complaint with his highly active antiretroviral therapy. The viral load was 8880 copies/mL and CD4 count was 180/µL. His hepatitis C was untreated. On evaluation, anti-nuclear antibody (ANA) was negative, C3, C4 levels were normal and his cryoglobulins were undetectable. Kidney ultrasound showed bilateral 10 cm kidneys. He had not been taking non-steroidal anti-inflammatory drugs. The differential diagnosis of increasing creatinine with nephrotic range proteinuria in a Caucasian patient with HIV and HCV includes immune complex GN (glomerulonephritis) secondary to HCV, postinfectious GN, lupus-like GN associated with HIV, IgA nephropathy (the majority of patients with HIV-associated IgA nephropathy are Caucasian or Hispanic 1 ) and rarely HIVAN. Thus, a kidney biopsy was done that demonstrated the classical histology of HIVAN (Figure 1).
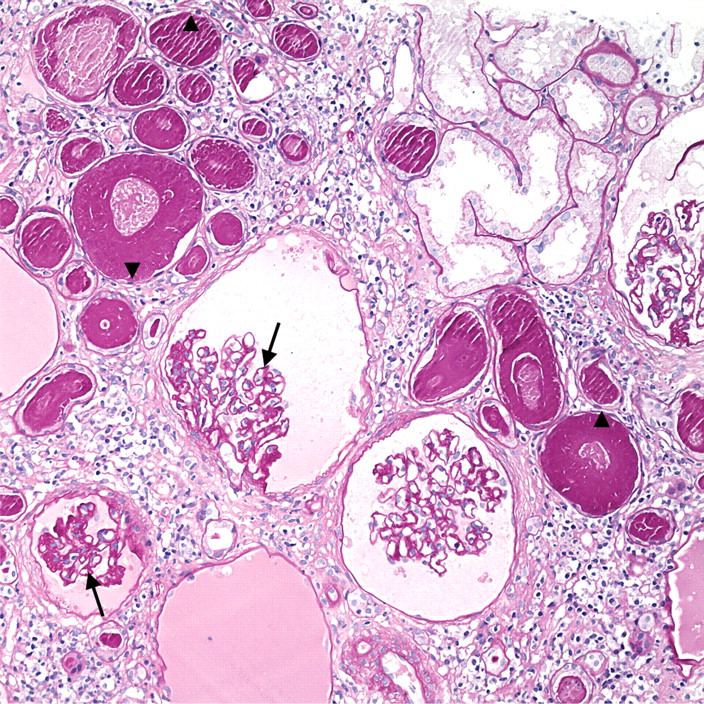
Renal biopsy characteristic of HIV-associated nephropathy: glomeruli show collapsing sclerosis (arrows) characterized by a global glomerular basement membrane wrinkling and collapse with narrowing and early obliteration of the capillary lumens. Adjacent tubules demonstrate marked microcystic dilation with flatting of the tubular epithelial cells (arrow heads) and are filled with proteinaceous casts. The interstitium shows an inflammatory cell infiltrate composed primarily of lymphocytes (periodic acid-Schiff, 200X)
DISCUSSION
HIVAN is one of the leading causes of end stage renal disease (ESRD) among AA. It is primarily a disease of AIDS but can occur at any stage of HIV infection. HIVAN is seen almost exclusively in people of African descent (Table 1). The mechanisms responsible for the predilection of HIVAN in AA are not well understood. In a study of inherited susceptibility to HIVAN, it was found that AA with HIVAN were 5.4 times more likely than AA controls to have close relatives with ESRD. This underscores the importance of a genetic predisposition to HIVAN in AA. 2 There are certain other factors that may explain the higher incidence of glomerulosclerosis in general in AA. These are larger glomerular volume and difference in the expression of growth factors especially transforming growth factor (TGF)-beta in AA. 3 Circulating TGF-beta protein levels in ESRD patients were found to be higher in AA when compared with Caucasians. 4 Increased TGF-beta is associated with increased extra cellular matrix in both humans and transgenic mice with HIVAN. 5,6 Individuals who are homozygous for a deletion mutation in the HIV-1 co-receptor, CCR5 (cc-chemokine receptor 5), are protected from HIV-1 infection, and this mutation is found exclusively in Caucasians. 7 Until now, the only gene that differs in AA with HIVAN and AA controls subjects is the angiotensin-converting enzyme gene. Larger studies in humans have been initiated to study genetic polymorphisms responsible for HIVAN. 8
HIV-associated nephropathy (HIVAN) in African-Americans
AA = African-Americans
CONCLUSION
HIVAN is predominantly seen in AA and is rare in Caucasians. In HIV-infected Caucasians, glomerular lesions are more likely to be immune-complex mediated. As our case with HCV and HIV illustrates, HIVAN should be considered in the differential diagnosis of nephrotic syndrome and renal failure in Caucasians with HIV infection.